A recent study, funded by the Centers for Disease Control and Prevention (CDC) and published in the American Journal of Public Health, focused on two years of opioid and stimulant seizure data from the Indianapolis police. The researchers examined how these seizures impacted fatal and non-fatal overdoses in the areas where the seizures took place within specific time frames.
-
Throughout 2020-2021, I wrote many pieces about COVID in an effort to highlight both the severity of the disease and the failure of capitalist governments to ensure the health and safety of their citizens, especially the most vulnerable of them, in the face of a global pandemic. I also edited a series, “Dispatches from the Frontlines of Care,” where I tried to center the voices of essential…
-
In a new report from the Centers for Disease Control and Prevention (CDC), federal researchers acknowledge in detail that police-perpetrated killings are a major cause of violent death in the United States, and Black and Indigenous men are disproportionally killed by police compared to all other groups tracked in the data. Experts say the analysis is a step forward for the CDC, but crucial data on…
This post was originally published on Latest – Truthout.
-
Before Missouri resident Amanda K. Finley had heard of COVID-19 or long COVID, she worked as an archeologist. Although her work schedule was erratic, she was frequently hired by engineering firms to make sure that the development sites they intended to build on conserved the cultural integrity of the land. She did this for 14 years. Then, in March 2020, 10 months before the COVID vaccine became…
This post was originally published on Latest – Truthout.
-
This is the third episode in our three-part series taking listeners inside the failed federal response to COVID-19. Series host Jessica Malaty Rivera and reporters Artis Curiskis and Kara Oehler bring us the conclusion of The COVID Tracking Project story and an interview with the current CDC director, Dr. Rochelle Walensky.
We look at the myth that COVID-19 was “the great equalizer,” an idea touted by celebrities and politicians from Madonna to then-New York Gov. Andrew Cuomo. Ibram X. Kendi and Boston University’s Center for Antiracist Research worked with The COVID Tracking Project to compile national numbers on how COVID-19 affected people of color in the U.S. Their effort, The COVID Racial Data Tracker, showed that people of color died from the disease at around twice the rate of White people.
The COVID Tracking Project’s volunteer data collection team waited months for the CDC to release COVID-19 testing data. But when the CDC finally started publishing the data, it was different from what states were publishing – in some instances, it was off by hundreds of thousands of tests. With no clear answers about why, The COVID Tracking Project’s quest to keep national data flowing every day continued until March 2021.
Lastly, Rivera talks with the director of the CDC, Walensky, to try to understand what went wrong in the agency’s response to the pandemic and ask whether it’s prepared for the next one.
Check out our whole COVID Tracking Project series here.
Support Reveal’s journalism at Revealnews.org/donatenow
Subscribe to our weekly newsletter to get the scoop on new episodes at Revealnews.org/newsletter
This post was originally published on Reveal.
-
This is the second episode in our three-part series taking listeners inside the failed federal response to COVID-19. In episode two, series host Jessica Malaty Rivera, along with reporters Artis Curiskis and Kara Oehler, asks a profound question: Why was there no good U.S. data about COVID-19?
In March 2020, White House Coronavirus Task Force coordinator Dr. Deborah Birx had a daunting task for healthcare technologist Amy Gleason, a new member of her data team. Her job was to figure out where people were testing positive for COVID-19 across the country, how many were in hospitals and how many had died from the disease. Accounting for national numbers about the disease was extremely difficult, because when COVID-19 hit, the federal government had no system set up to get data from each state.
Gleason was shocked to find that data from the Centers for Disease Control and Prevention wasn’t reflecting the immediate impact of the coronavirus. At the same time, the country was suffering from another huge shortfall: a lack of COVID-19 tests. As a congressional hearing in March 2020 clearly exposed, the CDC had created only 75,000 tests and had no plans to create the millions needed to make testing available nationwide. Dr. Birx and the Task Force also faced national shortages of medical supplies like masks and ventilators and lacked basic information about COVID-19 hospitalizations that would help them know where to send supplies.
Realizing that the federal government was failing to collect national data, reporters at The Atlantic formed The COVID Tracking Project. Across all 50 states, hundreds of volunteers began gathering crucial information on the number of cases, deaths and hospitalizations. Each day, they compiled the state COVID-19 data in a massive spreadsheet, creating the nation’s most reliable picture of the spread of the deadly disease.
Check out our whole COVID Tracking Project series here.
Support Reveal’s journalism at Revealnews.org/donatenow
Subscribe to our weekly newsletter to get the scoop on new episodes at Revealnews.org/newsletter
This post was originally published on Reveal.
-


The COVID Tracking Project
This three-part series exposes the Centers for Disease Control and Prevention’s bungled response to COVID-19 in the early days of the pandemic and takes listeners inside the massive volunteer effort to collect data about tests, cases, hospitalizations and deaths in the U.S.
The United States has 4% of the world’s population, but 16% of COVID-19 deaths. This series investigates the failures that led to over 1 million Americans dying from COVID-19 and what that tells us about the nation’s ability to respond to the next pandemic. This three-part series was reported by Artis Curiskis and Kara Oehler and hosted by infectious disease expert Jessica Malaty Rivera.

Credit: Illustration by Amanda Northrup The COVID Tracking Project Part 1
In February 2020, reporters Rob Meyer and Alexis Madrigal from The Atlantic were trying to find solid data about the rising pandemic. They published a story that revealed a scary truth: The U.S. didn’t know where COVID-19 was spreading because few tests were available. The CDC also didn’t have public data to tell citizens or federal agencies how many people were infected or where the outbreaks were happening.

Credit: Illustration by Amanda Northrup The COVID Tracking Project Part 2
In March 2020, White House Coronavirus Task Force coordinator Dr. Deborah Birx had a daunting task for technologist Amy Gleason, a new member of her data team. Her job was to figure out where people were testing positive for COVID-19 across the country, how many were in hospitals and how many had died from the disease. Gleason was shocked to find that data from the CDC wasn’t reflecting the immediate impact of the coronavirus.

Credit: Illustration by Amanda Northrup The COVID Tracking Project Part 3
The COVID Tracking Project closes with a look at racial disparities in deaths from the disease and what the CDC has learned. Jessica Malaty Rivera talks with the current CDC director, Dr. Rochelle Walensky, to try to understand what went wrong in the agency’s response to the pandemic – and ask whether it’s prepared for the next one.
SUBSCRIBE TO REVEAL ON YOUR FAVORITE PODCAST APP
Subscribe to our newsletter
Get the latest updates on this project by signing up for The Weekly Reveal.
Processing…Success! You're on the list.Whoops! There was an error and we couldn't process your subscription. Please reload the page and try again.Credits

Special thanks to The COVID Tracking Project at The Atlantic. This series is presented by Tableau.
Host: Jessica Malaty Rivera
Executive producer and reporter: Kara Oehler
Executive producer and reporter: Artis Curiskis
Lead editor: Michael I Schiller
Production assistants: Max Maldonado, Kori Suzuki and Aarushi Sahejpal | Fact checker: Nikki Frick | Production manager: Steven Rascón | Digital producer: Sarah Mirk | Episode art: Amanda Northrup | Original score and sound design: Jim Briggs and Fernando Arruda | Post-production team: Kathryn Styer Martinez and Michael Montgomery | Interim executive producers: Brett Myers and Taki Telonidis
Support for Reveal is provided by the Reva and David Logan Foundation, the John D. and Catherine T. MacArthur Foundation, the Jonathan Logan Family Foundation, the Ford Foundation, the Hellman Foundation, the Robert Wood Johnson Foundation, and the Park Foundation.
The COVID Tracking Project is a story from Reveal. Reveal is a registered trademark of The Center for Investigative Reporting and is a 501(c)(3) tax exempt organization.
This post was originally published on Reveal.
-
The United States has 4% of the world’s population but 16% of COVID-19 deaths. This series investigates the failures by federal agencies that led to over 1 million Americans dying from COVID-19 and what that tells us about the nation’s ability to fight the next pandemic. Epidemiologist Jessica Malaty Rivera is the host for this three-part series.
The first episode takes us back to February 2020, when reporters Rob Meyer and Alexis Madrigal from The Atlantic were trying to find solid data about the rising pandemic. They published a story that revealed a scary truth: The U.S. didn’t know where COVID-19 was spreading because few tests were available. The Centers for Disease Control and Prevention also didn’t have public data to tell citizens or federal agencies how many people were infected or where the outbreaks were happening.
Their reporting led to a massive volunteer effort by hundreds of people across the country who gathered the data themselves. The COVID Tracking Project became a de facto source of data amid the chaos of COVID-19. With case counts rising quickly, volunteers scrambled to document tests, hospitalizations and deaths in an effort to show where the virus was and who was dying.
Support Reveal’s journalism at Revealnews.org/donatenow
Subscribe to our weekly newsletter to get the scoop on new episodes at Revealnews.org/newsletter
This post was originally published on Reveal.
-
Canberra Data Centres has committed an additional $1 billion to expand its data centre campus at Eastern Creek, Sydney as it officially opened the facility on Wednesday. Four data centres are currently housed at the $1.5 billion facility currently representing a combined capacity of 123MW, with plans to begin construction on two additional data centres…
The post Canberra Data Centres plans $1bn expansion in Sydney appeared first on InnovationAus.com.
This post was originally published on InnovationAus.com.
-
As covid-19 raged, roughly 4,000 highly skilled epidemiologists, communication specialists, and public health nurses were hired by a nonprofit tied to the Centers for Disease Control and Prevention to plug the holes at battered public health departments on the front lines.
But over the past few months, the majority of the CDC Foundation’s contracts for those public health workers at local and state departments have ended as the group has spent nearly all of its almost $289 million in covid relief funding. The CDC Foundation, an independent nonprofit that supports the CDC’s work, anticipates that no more than about 800 of its 4,000 hires will ultimately staff those jurisdictions, spokesperson Pierce Nelson said.
That has left many local and state health departments facing staffing shortages as the nation eyes a possible winter uptick in covid cases and grapples with the ongoing threat of monkeypox, exploding caseloads of sexually transmitted infections, and other public health issues.
The public health workforce in the U.S. has been underfunded for decades — just before the start of the pandemic, only 28% of local health departments had an epidemiologist or statistician, a 2020 Associated Press–KHN investigation found. Then, after the pandemic began, public health officials left in droves as they were lambasted for instituting covid rules, blamed for the economic downturn, and grappled with burnout.
And even if funding were available to retain all 4,000 foundation employees, that would not have met public health staffing needs, according to new research in the Journal of Public Health Management and Practice. The research says at least 80,000 new employees are required for state and local public health departments to implement the minimum package of public health services.
However, the funding for the foundation jobs was always time-limited because it was intended to help the emergency response to covid. And although the American public’s covid concerns have waned, public health experts warn this is yet another example of the failure to properly fund the public health sector with annual, guaranteed money — leaving the country unable to prevent and properly fight outbreaks.
“So the boom-and-the-bust cycle continues despite losing a million American lives to covid,” said Brian Castrucci, who co-authored the report and heads the de Beaumont Foundation, which advocates for increasing support for the nation’s public health. “How many American deaths is it going to take until we fix this problem?”
Unlike the thousands of inexperienced contact tracers hired to follow up with covid patients to stem the spread amid the surge, this CDC Foundation workforce typically had public health expertise that also could fill preexisting gaps. The foundation’s head, Dr. Judy Monroe, said local and state officials loved the foundation’s ability to cut through hiring red tape, telling her “it was like the cavalry showed up.”
In Chicago, CDC Foundation employees made up about as much as a tenth of the city’s public health workforce, said Dr. Allison Arwady, commissioner of the city’s public health department. Although she got 26 of those 66 employees extended into December, she said it’ll hurt to lose the rest. They’ve contributed to everything from public health nursing to communicating the latest guidance about the pandemic to Chicagoans.
Cayenne Levorse, a CDC Foundation leader who helped organize the foundation’s response in Ohio until her contract ended in October, said her 20 employees had to set down not only covid projects but also helping local health departments track cancer clusters, rural health disparities, and environmental health problems.
“Those jobs are just sitting there, all that work left unfinished,” she said.
Five people hired for CDC Foundation covid contracts told KHN they were under the impression their contracts would likely be extended or they would be hired by local or state governments receiving a flood of covid dollars. Only one of them had a contract as of Nov. 8.
Senior epidemiologist Katie Schenk, who has a doctorate in public health, did covid surveillance for the CDC Foundation at the Illinois and Washington, D.C., health departments. Both contracts ran out, and she was left without a job this summer.
“How do you explain that there is no funding for employment in our field when there is clearly so much work to be done?” she asked. “It’s to the detriment of the public health system, which is shedding staff like there’s no tomorrow.”
Sometime in November, state and local health officials are expecting $3 billion in covid relief money targeted at buttressing the public health workforce. But that funding is coming after most of the CDC Foundation contracts have expired and those employees have moved on with their lives.
Although that sum is substantial and will help close the 80,000-worker gap, many public health officials and experts stressed that the cash is short-term and slated to last five years — which can make positions harder to fill as candidates seek job stability. It also is divided among 50 states, U.S. territories, and multiple large health departments. And some state and local officials, such as those in Missouri and Michigan, have refused to spend covid dollars on public health departments amid the backlash against the pandemic response.
State and local governments sometimes have caps on hiring full-time employees even if federal money is available to do so, Monroe said. Some localities have pay freezes or are not willing to spend more on health officials than on other government employees, making highly skilled workers such as epidemiologists harder to hire, she said. And the CDC Foundation salaries and benefits were sometimes better than what is available at local and state-level jobs, Monroe said. Many of the foundation workers could face a pay cut if they wanted to stay on with the local departments.
“You certainly don’t go into public health to get rich,” said epidemiologist Susan Knoll, who took a private-sector job as a health consultant after working for the CDC Foundation in Ohio. “You get a grant-funded job. And then you’re always looking for another job.”
That’s “the reality of how we fund public health in this country,” said Chrissie Juliano, executive director of the Big Cities Health Coalition.
“We ramp up, and we ramp down, and we don’t think about routine work,” she said. “We should not as a field be losing qualified people who are committed to working in public health. Those are the people who need to be saved.”
At least 38,000 public health jobs at the state and local level were lost from the 2008 recession through 2019. Then covid hit, and 1 in 5 Americans lost a local public health leader amid the political backlash of the first years of the pandemic, a 2021 AP–KHN investigation found.
Some of the remaining workforce is eyeing the door. The director of North Carolina’s Granville Vance Public Health department, Lisa Macon Harrison, said that even after instituting flexible benefits, she’s seeing 15% to 20% turnover, which she blames on burnout.
Levorse noted that epidemiologists and other staffers with advanced degrees have student loans to pay off and worry about losing health insurance each time a grant runs out.
The lack of a steady source of money from year to year is jeopardizing health department programs, Chicago’s Arwady said. She estimates the city will lose 86% of its current grant funding in two years, putting wastewater tracking, some of her department’s IT staff, and community-based outreach on the possible chopping block.
“We’re not going to be able to do half a dozen things that the city of Chicago clearly expects we should be able to do. Forget ‘Can I bring vaccine to your house?’ It’s ‘Can I even stand up, like, a vaccine clinic in your neighborhood?’” she said. “It’s that level of how far backwards I’m afraid we’re going to slide.”
Harrison said she’s seen this all before: A flood of funding for pandemic preparedness came after 9/11, and then the money for staffing went away, leaving departments flat-footed for covid.
Castrucci, of the de Beaumont Foundation, rued how the current funding structure ensures that the public health sector, which exists to prevent outbreaks and disease, won’t be given the staff to do so until an emergency arrives.
“You’re basically saying, ‘We will wait for the fire to burn until we hire the firefighters,’” he said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
-
New research from the Centers for Disease Control (CDC) reveals deep racial disparities in access to Paxlovid, a drug commonly used to treat COVID-19 infections for higher-risk patients, raising longstanding concerns about racism within the health system as officials fear an explosion of COVID cases over the winter.
The CDC’s Morbidity and Mortality Weekly Report released on Friday includes data showing that Black patients were prescribed Paxlovid for out-patient COVID treatment 36 percent less often than white patients from April to July 2022, a period of time when Paxlovid became widely available and use of the drug surged.
Compared to white patients, Latinx patients received Paxlovid for out-patient COVID-19 treatment 30 percent less often; patients reporting more than one racial background received the drug 25 percent less often; Indigenous patients (including Native Alaskans, Native Hawaiians and Pacific Islanders) saw treatment 23 percent less often, and Asian Americans received Paxlovid nearly 20 percent less often than white people.
By January of 2022, Paxlovid was one of four medications that received an emergency authorization from the Food and Drug Administration for outpatient treatment of COVID-19 infection. Paxlovid is by far the most common treatment, and use of the drug skyrocketed as the Biden administration made it free to patients with a doctor’s prescription.
The CDC found racial disparities in Paxlovid treatment across all age groups, but disparities were “generally somewhat higher among patients at high risk for severe COVID-19,” including immunocompromised patients and patients over the age of 50.
“Paxlovid was especially hard to get this spring,” said Kaiser Health News reporter Hannah Recht on Twitter after investigating Paxlovid access for months. “The much-hyped Test-to-Treat program had 0 (zero) sites in some states and launched almost entirely with CVS, which was at the time really hard to use and often expensive.”
The Biden administration launched the Test-to-Treat program earlier this year at thousands of pharmacy clinics, federally-funded health centers, nursing homes and other “community based sites,” where patients can get tested for COVID and receive Paxlovid or a different treatment in one visit.
The Biden administration expanded the program in May by adding more Test-to-Treat sites supported by federal dollars in an effort to reach vulnerable communities, and Recht said a number of states and cities have recently launched new sites that are searchable online. However, for patients who do not live near the sites or live in a (likely red) state that did not work with the administration to establish a Test-to-Treat program, Paxlovid is only available by visiting a doctor and receiving a prescription. That takes time and money, Recht said.
“This new data also mirrors what we saw with the first covid treatments in 2021,” Recht said. “Those too were massively underused in treating non-white patients.”
This is not the first time the CDC identified deep racial disparities in federal health data. Earlier this year, the CDC reported that skyrocketing rates of drug overdose deaths among Black and Brown people during the height of the pandemic in 2020 were likely the result of social isolation and unequal access to health care, harm reduction services and medications used to treat opioid addiction, among other factors. White people were far more likely to access effective addiction treatments than people of color.
The CDC did not say what caused the racial disparities in Paxlovid access, but they likely reflect a critically underfunded public health care system, unequal access to quality health care facilities, and racial bias among individual doctors and providers. Expanded programs “focused on equitable awareness of and access” to COVID-19 vaccines and treatments are needed to protect the most vulnerable from serious infection, the CDC said.
This post was originally published on Latest – Truthout.
-
Canberra Data Centres has booked more than $1 billion in Commonwealth contracts since launching in 2007 to meet the storage needs of the federal government, passing the milestone with the signing of a new 10-year deal with Defence last month. The $91.5 million Defence contract is double the value of its previous most lucrative contract…
The post CDC federal work passes $1b with new Defence deal appeared first on InnovationAus.com.
This post was originally published on InnovationAus.com.
-
Early carnivals offered political power a safety value. For a few days a year, rich and poor switched positions. The poor ran society (if in ritual only), except, when things were going badly in the everyday, the reversal suddenly turned into open rebellion from below.
In the present pandemic, it’s the powerful who are running a months-long masquerade, taking off masks ironically enough, in the face of all the evidence that the pandemic is marching on and mask mandates in combination with vaccines and other interventions can protect populations from infection.
The ruling class’s public health putsch aims to free a precarious just-in-time capitalism from supply chain gluts and social welfare obligations that a serious pandemic imposes. Better let people get sick or die than violate such a society’s prime directive placing profits first, the political class plots.
SARS-CoV-2, the COVID-19 virus, is cycling through new variants every two months, tinkering with both the human immune system and our already precarious vaccine coverage. The reduced deadliness the virus seems to represent at the moment, as some experts pronounce, isn’t a set outcome. It’s only one of multiple possibilities. As the hospitalizations, which doubled under the BA.5 variant underscore, sudden surges in virulence are also possible, perhaps even likely as the virus is being left to explore its evolutionary possibilities.
The virus, meanwhile, keeps knocking thousands into the Long COVID side pocket, where patients are lost to complex combinations of chronic conditions that medicine is finding difficult to treat.
The State of the Pandemic
Where are we in the global pandemic? The Johns Hopkins Coronavirus Resource Center reported another 7.16 million new COVID cases worldwide for the week ending July 31 (see the red time series on the right of the John Hopkins dashboard). That’s more new weekly cases than for any other COVID wave except Omicron this past winter.
The number of global weekly deaths underwent another increase to 16,400 deaths the week ending July 31, although representing fewer cases than in previous waves (the white time series on the right of the Johns Hopkins dashboard). Forty-two million new vaccinations were administered that week worldwide (the green time series).
The New York Times is mapping COVID hotspots in the Americas, Europe, Asia and Australasia. There in purple, France, Germany, Austria, Italy, Greece, Taiwan, Australia and New Zealand continue to be epicenters in average daily new cases per 100,000 population. In recent weeks, Costa Rica, Finland, Japan, South Korea, and Thailand all returned to hotspot status. Canada, Mexico, Brazil, Peru, Bolivia, Argentina, Tunisia, Armenia, Kazakhstan, Iran, Iraq and Mongolia hosted recent increases in caseloads. Panama, Botswana, Portugal, Spain and Norway saw declines from late June.
The seven-day average of daily confirmed COVID cases per million people from the beginning of the outbreak shows the present hotspots are trending in different directions. Taiwan and Italy’s outbreaks appear in decline. Greece and Finland are hosting large new spikes. Japan, South Korea, and Mongolia are hosting new surges. Australia, New Zealand, France, Italy and Germany continue to cycle through their months-long epidemics. The U.S., the U.K. and Brazil are reporting slow but steady increases. We see that none of the countries highlighted are reporting national testing data as of July 3 (click on “color by test positivity”).
For the COVID deaths per million people for these same countries, we see that the U.S., Brazil and Germany are showing slight increases. Italy, the U.K. and Australia are showing more robust increases, and Costa Rica, Finland and Greece are displaying sharp spikes.
The virus also continues to evolve. This is a family tree for COVID samples over the past six months, although, for the radial version of the tree, rooted from the beginning of the pandemic at the center of the diagram and branching outward as SARS-2 evolves. We see in dark blues and purples the early variants like Alpha and Beta. In the light blue are samples of the Delta variant. We see over the past six months that multiple Omicron subvariants — there in yellow BA.1 and 2, in the light and medium oranges BA.4 and 5, and the darker orange BA.2.12 — are continuing to explore SARS-2’s evolutionary space. Indeed, we see in the few red samples the arrival of subvariant BA.2.75 or the Centaurus variant found first in India in June.
Across the Omicron group, we find molecular changes from the root of the SARS-2 tree here numbering as high as 64 amino acid changes and 16 deletions. What that means is that the virus continues to evolve, along the way experimenting with the human immune system to the tune of over 7 million new infections a week during what governments worldwide are treating as the end of the pandemic.
Hospitalizations are all up in the countries in our highlighted set. These appear as a function of the surge in caseloads, the reemergence of deadlier subvariants such as BA.5, and a developing mismatch between Omicron and COVID vaccines. We also see across countries in our set a near-global retraction in nonpharmaceutical interventions since Omicron. These indices of the stringency of public health measures show that some countries at first attempted to differentiate masking mandates and the like for the vaccinated (in green) and for the unvaccinated (in brown) before largely abandoning that distinction.
That combo — evolving subvariants probing our defenses and a willful public health surrender — bodes ill for this winter’s likely surge.
The U.S. Outbreak
As of August 7, the U.S. continues to host a raised floor in COVID-19 caseloads post-winter Omicron. This summer marks the worst in U.S. COVID-19 incidence of the three summers so far in this pandemic.
The New York Times map shows Northeast and upper Midwest are presently characterized by a relative decline in COVID. But we also see the start of a possible new surge in New Jersey, New York City and now, Pennsylvania. We see sharp spikes in Appalachia, particularly in Kentucky and West Virginia. The South is hosting lifted floors, especially in North Carolina, northern Louisiana, the Florida panhandle, Miami, parts of Alabama and Georgia, Oklahoma overall, and select counties in west and south Texas. We see a slight decline along the West Coast, a steady surge in parts of the Southwest, and sharp spikes county-by-county across the Plains states. Alaska and Puerto Rico continue to be hit badly.
There are other ways of tracking COVID. The levels of SARS-2 virus detected in the wastewater that comes through our sewage plants as reported here (July 19-August 2) shows little change from earlier in July. Sewage plants in red represent loads at 80 to 100 percent their previously recorded levels. We see these scattered across the U.S., but especially in Nebraska, Illinois, Ohio, Kentucky, South Carolina and downstate New York. The cool blues of recorded lows in the Northeast are starting to be infiltrated by increased SARS-2 concentrations in orange from New Jersey up north. We do see cooling off in coastal Washington State, Oregon and northern California.
The map of percent change in the last 15 days underscores the West Coast’s cooling off. We see such declines in light blue of 10 to 90 percent across Utah, Colorado, Nebraska, and what we were worried about in the first wastewater map in downstate New York. These might represent only mean declines off very large peaks that still host widespread COVID. At the same time, we see new 15-day surges in Illinois, Ohio, upstate New York, Kentucky and North Carolina.
A standing problem in tracking COVID-19 stateside is that the U.S. appears to be willfully ignoring previous surveillance measures. In April, ABC News and other outlets reported that the Department of Health and Human Services ended the requirement that hospitals report daily COVID deaths, overflow and ventilated COVID patients, and critical staffing shortages. Some U.S. states outright ended reporting COVID metrics, hospital bed usage and availability, and ventilator use. Some states turned to delaying COVID-19 numbers to reports on a weekly basis.
The ABC News report continued that some hospitals are following the National Institute of Health’s lead in changing definitions of COVID cases, including to only those patients that receive antivirals remdesivir or dexamethasone. So COVID cases wouldn’t be counted unless the patient needed those drugs.
It appears the willful decline in monitoring is beginning to extract its public health costs. For instance, we see here in San Francisco that previously SARS-2 loads in sewage (in blue) tracked COVID caseloads (in red). That appears no longer to be the case, with COVID caseloads during BA.4 and 5 likely to be underreported.
To sum up U.S. COVID, we see almost the entire country — 94 percent of U.S. counties — under “Data Type: Community Transmission” in the CDC maps is filled in at the highest level of community transmission, including what were a month ago sites of COVID decline in Iowa, Pennsylvania and New York State. The summer surge is accumulating with much of the country still reporting in COVID-19 tests at 20 percent or more positive (click on “Nucleic Acid Amplification Tests (NAATs)”). And much of the country — especially through the South, Appalachia and the Plains states — with less than 30 percent of the population with two COVID vaccine shots, even before including subsequent boosters (click on “Vaccinations” on the left and “% of total population fully vaccinated” on the right).
Monkeypox Marks Another Roll of the Epidemiological Dice
As on the global stage, SARS-2 continues to evolve here in the U.S. We see here new variants first emerging and then dominating in cycles of every two months. The BA.2 Omicron subvariant in pink was replaced by the BA2.12 subvariant in orange, which is now being replaced by subvariants BA.4 and 5 in green, with BA.5 surging ahead to account for over 85 percent of new cases as of July 30.
Each new COVID variant marks the U.S.’s — and the world’s — concerted failure to control infectious disease. Entirely new pathogens underscore the point. Monkeypox — a previously marginal Orthopoxvirus that can induce at times very painful lesions in the anus, genitals and mouth — has spread to all but two U.S. states, with patients getting little access to follow-up care or the vaccines that at best offer disease mitigation.
Epidemiologist Kathryn Jacobsen reports that the federal government’s recent declaration that monkeypox represented a U.S. public health emergency opens up more of such resources. The declaration, while welcome, is a month too late from helping quash an outbreak once limited to a few urban epicenters. The declaration also serves more as a guideline for local public health departments as to reporting and treatment, but not how to intervene or to help the greater community respond, with schools about to reopen at the end of August.
That is, the failures of the COVID response stateside have been set on repeat. The damage isn’t merely a matter of the surprise of a new outbreak or which political party is in power. The fiasco is systemic and extends back into the disease cascade.
Each new emergent pathogen represents a roll of the socioecological dice. Deforestation and development in the far reaches of capitalist production are springing even the most marginal pathogens out onto global trade and travel networks to reach countries that have taken great pride in destroying their own public health systems in the name of open economies.
Here, Rebecca Levine’s team maps its ecological niche model of monkeypox distribution across Sub-Saharan Africa, including in a Congo Basin that since has suffered considerable deforestation, especially there in the purple.
While most land deals underlying extraction in the Congo Basin are European and Asian in origin, the Land Matrix Observatory identified seven deals with direct American investment, including a 348,000-hectare deal with U.S.-registered Congo Emissions Management and Groupe Blattner Elwyn. Although this latter deal appears to be pursued under the rubric of carbon offsets, such agreements in green capitalism score their damage in helping rationalize offshore capital’s right to the Global South.
Many of the European and Asian efforts in the Congo and across West Africa meanwhile end up supplying U.S. customers, including wood siding to retailers Home Depot and Menards.
The defacement only compounds in its effects. When the Global North refused to follow through with a promised $500 million to the Democratic Republic of the Congo (DRC) to preserve its rainforest, the DRC, looking to Angola and Nigeria’s path of development, turned to auctioning off its forest to oil companies, including Virunga National Park, the critical gorilla sanctuary.
Monkeypox in the U.S. may be a matter of blowback. It’s not that any one of these land deals let loose this strain of the virus, but that pathogens are in part sprung when this model of development turns food forests into cleared land and expropriated resources marked by a loss in the environmental complexity that once bottled in those pathogens.
Two Additional Dangers
The capital-led destruction is also found on this side of disease spillover. Two additional dangers other than acute infections and deaths — the latter now projected at 17.5 million or more — arise from letting SARS-2 run free.
The first is that the virus may experiment enough to figure out how to emerge from our vaccines’ disease immunity — the protection the vaccines offer us from getting too sick when we’re infected.
One Dutch team of microbiologists produced what’s called an antigenic map to track vaccine coverage. The map on the left shows that the Omicron subvariant BA.1 evolved out from underneath the protection provided by being infected with earlier variants like Alpha, Beta and Delta. The map on the right tracks the antibody neutralization the vaccines provide in comparison to the circulating COVID variants. That map shows Omicron (in pink) has escaped the antibodies produced by the vaccines we’ve used to this point.
That doesn’t mean the vaccines are useless, just that they don’t necessarily produce all the Omicron-specific antibodies.
Moderna is reporting its Omicron-specific vaccine in development to be successful. But we are likely in for boosters for years, with no guarantee a SARS-2 on a two-month schedule won’t continue to evolve out from underneath that protection.
The second danger is the Long COVID any one infection may induce or, perhaps, the cumulative impact of multiple COVID infections. A Weill Cornell Medicine team recently summarized the damage: On the left, the little graphs in red show the hazard ratios of all the body systems that have been documented to be impacted.
The “Long” in Long COVID isn’t just the length of time of such an infection, but also represents a foundational transition from an acute respiratory infection to a chronic condition of often devastating impact. We’re talking about various combinations of cognitive impairments, ulcers, pulmonary fibrosis, embolisms, diabetes, fatigue, and many more illnesses in the list to the left of the human figure shown.
To the right of the figure, we see all the different drugs Long COVID patients are found to be at a higher risk of having to take.
That’s why the People’s CDC — the coalition of public health practitioners and everyday people I’ve joined — is adamant that all efforts must be made to implement a full array of public health interventions that keep all people, whatever their starting health, from entering the horror of Long COVID.
Biden’s Mask Off Shows Us Another Trump
In contrast, a Biden administration elected to volte-face Trump on COVID turned its position 360 degrees back to Trump positions. In the face of an adaptive and ongoing pandemic that is producing nearly 7 million new infections a week worldwide and Omicron subvariants evolving out from under vaccine coverage, the Biden administration decided to declare victory on COVID-19.
NBC News reported that in February, Impact Research, the administration’s polling firm, recommended moving beyond merely dropping mask mandates and by default toward discouraging mask use.
Molly Murphy and Brian Stryker of Impact suggested that the administration make a play for November’s midterm elections and “declare the crisis phase of COVID over and push for feeling and acting more normal.” In what seem to be talking points from the problematic “Urgency of Normal” campaign that encouraged moving students back into schools without adjunct interventions, Murphy and Stryker cited learning loss at school and COVID’s effect on the economy as reasons to exit COVID as a reality.
Both problems arose out of decisions the Trump and Biden administrations made in refusing to provide adequate support for communities and households alike during a national crisis. At the same time, the Impact memo continued, aiming to eliminate COVID isn’t the answer. In effect, with language reminiscent of Trump’s Chief of Staff Mark Meadows, the memo admits that COVID will remain the reality, which Murphy and Stryker also suggest the Biden administration ignore.
The CDC, other administration officials, and outside epidemiologists would follow up the memo by warning the American people of upcoming COVID spikes, including this fall and winter when Americans go to the polls.
Such realities are socially structured. In early July, Anna Peele interviewed the soon-to-retire Anthony Fauci for the Washington Post magazine, under the headline, “The Pandemic Is Waning”:
I am also aware that it would be a moral crime to transmit the coronavirus to Fauci. So when I got COVID two weeks before our interview, I obsessively parsed the guidelines from the Centers for Disease Control and Prevention: As long as I waited 10 days after my first positive test, I could still meet Fauci in person, right? No, I was informed by Fauci, via a member of his communications team. I would need to test negative three days in a row and wear a mask, even outdoors.
So, no five-day quarantine for Fauci’s circle along the lines a CDC under employer pressure recommended for Americans. And Fauci treats the possibility of infection after 10 days as real. These are exactly the kinds of precautions the People’s CDC recommended for the rest of the country.
When Biden finally contracted COVID, showing up to work maskless while infected, CDC Director Rochelle Walensky took to the airwaves saying that, yes, the president would be treated with precautions above and beyond what the CDC recommended for the American people. After all, the Americans whom the administration abandoned make up the labor force that chooses to go to work sick or alongside sick coworkers. The CDC is only accommodating them:
Yeah, I think we can all agree that the president’s protocols likely go above and beyond and have the resources to go above and beyond what every American is able and has the capacity to do.
As we put forward our CDC guidance, we have to do so so that they are relevant, feasible, followable by Americans, and that is Americans that live in urban jurisdictions and rural jurisdictions, that have resources and less resources, that have, you know, work constraints and many other things. So, when we put forward our guidance, we do so so that they reflect such that every American is able to follow them.
A growing class divide, which mainstream public health must accommodate first and foremost in the folksiest of fatalism, is treated as more sacrosanct than the obligations to control and prevent an infectious pandemic.
The resulting damage is unlikely of any American’s choosing. “For the period from June 29 to July 11 [2022],” the Wall Street Journal reported, “3.9 million Americans said they didn’t work because they were sick with Covid-19 or were caring for someone with it, according to Census Bureau data. In the comparable period last year, 1.8 million people missed work for those reasons.”
Even steps forward act to fill in such continuing damage. The administration recently announced it would be establishing a new Department of Health and Human Services office dedicated to addressing the debilitating Long COVID that an estimated 23 million Americans are suffering beyond their initial acute infections. An associated National Research Action Plan on Long COVID is to be pursued alongside the administration’s efforts to “return to normal” and strip out programs in COVID prevention.
In other words, the supply of extremely difficult-to-treat Long COVID cases the administration now says it seeks to mitigate will continue apace to accommodate employers.
When Pandemic Play Turns Serious
Given the bipartisan push to end COVID as an idea (if not as an empirical fact), science writer Ed Yong’s sense of defeat may be more an acknowledgement that a different public health is possible. And that it’s already underway, with a passing reference to the People’s CDC:
In 2018, while reporting on pandemic preparedness in the Democratic Republic of Congo, I heard many people joking about the fictional 15th article of the country’s constitution: Débrouillez-vous, or ‘Figure it out yourself.’ It was a droll and weary acknowledgment that the government won’t save you, and you must make do with the resources you’ve got. The United States is now firmly in the débrouillez-vous era of the COVID-19 pandemic…
I have interviewed dozens of other local officials, community organizers, and grassroots groups who are also swimming furiously against the tide of governmental apathy to push some pandemic response forward, even if incrementally. This is an endeavor that all of American society would benefit from; it is currently concentrated among a network of exhausted individuals who are trying to figure out this pandemic, while living up to public health’s central tenet: Protect the health of all people, and the most vulnerable especially. The late Paul Farmer, who devoted his life to providing health care to the world’s poorest people, understood that when doing such work, victories would be hard-won, if ever won at all. Referencing a line from The Lord of the Rings, he once said, ‘I have fought the long defeat.’ In the third year of the COVID pandemic, that fight will determine how America fares against the variants and viruses still to come.
What Yong misses in his respectable summary is that the resulting patchwork isn’t just a reminder of what we have lost or what we might gain upon a reformation of a pivot, but perhaps a new world born out of the husk of the old.
With death and illness accumulating from one COVID variant to the next, and now with novel pathogen species like monkeypox joining the party, the ritualized protest that the capitalist carnival allows may suddenly lurch into open rebellion. Millions may organize to burn down that Venn diagram of going to work in an apocalypse. There is another option: they can refuse to get sick and die for profit’s sake.
-
In this story, we’ll explain what we know about the financial and conflict-of-interest disclosure requirements for Dr. Anthony Fauci, other National Institutes of Health higher-ups and members of two U.S. vaccine advisory committees.
The topic came up during a Senate hearing in June, when Republican Sen. Rand Paul of Kentucky questioned Fauci, director of the National Institute of Allergy and Infectious Diseases, about royalties paid to NIH and NIH inventors from third parties who have licensed NIH patents or inventions.
What do NIH officials have to disclose?
The NIH is one of several agencies within the U.S. Department of Health and Human Services, and the NIH itself is made up of 27 institutes and centers that conduct medical research, including the NIAID, which Fauci has directed since 1984.
 Each year, Fauci and other high-ranking NIH officials are among the many federal employees required to submit a public financial disclosure report (OGE Form 278e) to their employing agency or department. Less senior officials who do not meet the pay or classification requirements for public disclosure submit a confidential report.
Each year, Fauci and other high-ranking NIH officials are among the many federal employees required to submit a public financial disclosure report (OGE Form 278e) to their employing agency or department. Less senior officials who do not meet the pay or classification requirements for public disclosure submit a confidential report. In 2020, the Office of Government Ethics, which oversees the financial disclosure program for employees of the executive branch, reported that nearly 27,000 people were required to submit the public report disclosing information about the assets, income and other personal financial interests of the filer, the filer’s spouse and any dependent children.
The Congressional Research Service has explained that the reports filed by “the most senior officials in the executive branch — the President, Vice President, and appointees and nominees to positions classified at Level I and Level II of the Executive Schedule — are available directly from the OGE website.” However, for NIH officials such as Fauci, the public financial disclosures are only available upon request.
In January, we wrote about the multistep process we followed to obtain one of Fauci’s reports, which required emailing the federal health department at Ethics.FinancialDisclosure@hhs.gov, and then completing and submitting OGE Form 201 to the National Institutes of Health’s FOIA office at nihfoia@mail.nih.gov. It took us one business day to receive a redacted version of Fauci’s 42-page report that covered his financial activity for 2019, which was the most recent report available at the time.
But the response time varies, based on the accounts of others who have requested the same documents from NIH.
Republican Sen. Roger Marshall later obtained copies of Fauci’s largely unredacted financial disclosure forms covering the calendar years 2019 and 2020.
What does not have to be disclosed?
Federal laws enacted in the 1980s authorize government agencies, including the NIH, to license their inventions to third parties in exchange for royalties that can be used to fund additional research. A statutory formula determines the portion of the royalties that NIH institutes and centers have to share with the NIH employee, or former employee, listed as the inventor.
As Fauci indicated in his response to Paul, he and other NIH officials who must submit the financial disclosure report are not required to include details about royalty payments they have received for products or treatments they developed for the government.
“NIH inventors that receive royalties in the performance of their government duties do not have to disclose such royalties on their financial disclosure reports because they are considered income from the government,” the NIH said in a statement emailed to FactCheck.org. “If the NIH researcher is receiving royalty payments from a non-government institution where they may have worked previously, those royalties are required to be reported in financial disclosure forms and reviewed by NIH Ethics officials.”
NIH told us that it has a policy requiring the hundreds of researchers or investigators in its Intramural Research Program, including Fauci, to notify an NIH Institutional Review Board if the researcher is a recipient of government royalties related to clinical research.
“The NIH IRB will then determine whether additional measures are required to protect human subjects,” the NIH said. Those measures may include “disclosure of government royalty rights related to this research in the informed consent document, or if other circumstances exist in which there may be a financial conflict of interest, a statement that an actual or apparent conflict of interest may exist.”
What information about NIH royalties is publicly available?
Comprehensive information about royalties paid to the NIH and NIH inventors is not available online nor is it readily accessible by the public. On its website, the NIH publishes limited information about the payments, such as the total amounts received by the NIH and other agencies by fiscal year, as well as how those yearly amounts were divided between the NIH and its employee-inventors.
In FY 2021, for example, the NIH received more than $108 million in royalities and NIH inventors received a little over $11 million, according to NIH figures.
More detailed information is hard to come by, even for organizations that file requests under the Freedom of Information Act.
In early May, OpenTheBooks.com, a self-described government watchdog organization, said it had to pursue legal action to get the NIH to release thousands of pages of documents on royalties paid to the agency. But the group said the documents it has received thus far — covering royalties paid between September 2009 and September 2014 — were heavily redacted, excluding important information about which parties paid the royalties, which inventions the royalties were for, and the individual amounts paid to the NIH inventors.
“This makes the court-mandated production virtually worthless,” Adam Andrzejewski, the organization’s founder and CEO, wrote in the May 9 report.
But the redactions are necessary, the NIH has argued.
In another emailed statement, the agency said: “Detailed information about royalties received by NIH and NIH inventors named on [U.S. government] owned patents is considered Confidential Commercial Information and is appropriately withheld from disclosure under FOIA exemptions 3 and 4.” Exemption 3 allows for the withholding of information prohibited from disclosure by another federal law, and Exemption 4 protects trade secrets and commercial or financial information obtained that is privileged or confidential.
In a 2020 report, the Government Accountability Office recommended that the NIH provide more information to the public about the licensing of its intellectual property.
What are the requirements to serve on the CDC’s Advisory Committee on Immunization Practices?
The Advisory Committee on Immunization Practices is a federal advisory committee with 15 voting members, eight members from federal agencies related to immunization programs and 30 liaison representatives from professional organizations. The committee writes recommendations for the administration of vaccines for adults and children, and provides advice and guidance to the Centers for Disease Control and Prevention on vaccine safety.
Members of federal advisory committees, such as the ACIP, are considered Special Government Employees. That is, employees of the executive branch appointed to perform services for a limited amount of time. SGEs are required to file financial disclosure statements and are subject to federal law (18 U.S.C. §208) that prohibits them from participating “in matters in which, to their knowledge, they, their spouse, minor child, or organization has a financial interest.”
According to the committee’s policies and procedures document, ACIP members need to consent to these requirements during their four-year term:
ACIP Policies and Procedures, June 2022
- No member, his or her spouse, or a member of his or her immediate family can be directly employed by a vaccine manufacturer or its parent company.
- Members cannot hold stock in any vaccine manufacturer or its parent company in excess of the OGE de minimus amounts [threshold values established by the OGE]. Members also agree that they, their spouse and minor children will not purchase such stock during their tenure on the committee.
- Members cannot be holders of or otherwise be entitled to royalties or other compensation for a patent on a vaccine product or process, immunologic agent, adjunct or preservative that can be used for a vaccine that may come before ACIP during the anticipated term of appointment under consideration.
- Members agree to resign any advisory or consulting roles, whether paid or unpaid, to a vaccine manufacturer (except participation in clinical trials or service on data monitoring boards) and to forego such consultation or membership on any vaccine manufacturer advisory committees (except participation in clinical trials or service on data monitoring boards), during his/her tenure on ACIP.
- Members forego solicitation or acceptance of funds from vaccine manufacturers on behalf of themselves or others.
- During their tenure on ACIP, members do not serve as a paid litigation consultant or expert witness in litigation involving a vaccine manufacturer.
- Members do not accept honoraria or travel reimbursement with a funding source from a vaccine manufacturer for attendance at scientific meetings, with the exception that they may receive travel reimbursement for CME [Continuing Medical Education] presentations where the source of funding is an unrestricted grant to the CME provider by a vaccine manufacturer.
What do they have to disclose?
ACIP voting members are required to file an annual financial disclosure statement with the Office of Government Ethics.
The report — OGE form 450 — is confidential and must include assets greater than $1,000 for the member, spouse and dependent children; sources of earned income, honoraria and other non-investment income for the preceding 12 months; liabilities that exceeded $10,000 for the member, spouse and dependent children as of the date of filing; all positions held during the last year, and agreements and arrangements with former or future employers as of the date of filing. Those renewing a disclosure report are also required to disclose gifts and travel reimbursements over $166 and totaling more than $415 from “any one source” for themselves, their spouses and dependent children.
The CDC can “determine whether the need for the individual’s services outweighs the potential for conflicts of interest created by the financial interests involved” and issue limited waivers, in accordance with regulations by the OGE. According to ACIP’s policies, limited waivers “generally allow members to fully participate in committee discussions related to waived interests, with the condition that they will be prohibited from voting on such matters.”
Is it publicly available?
As we said, ACIP members’ financial disclosure statements are confidential, unlike those required for more senior officials in the executive branch, which are public.
But voting ACIP members are required to publicly disclose “all vaccine-related interests and work, including participation in clinical trials” at the opening of each meeting and prior to any vote. The ACIP holds three regular public meetings each year, plus emergency sessions. The public can view videos of those meetings, going back to June 2013 on the ACIP channel on YouTube.
According to the CDC, at several meetings during the coronavirus pandemic one ACIP member, Dr. Wilbur Chen, disclosed that his institution, the University of Maryland, received support from Emergent BioSolutions for the development of a different vaccine (shigella). Emergent is a biotechnology company based in Maryland that ruined millions of COVID-19 vaccine doses at a manufacturing plant because of cross-contamination. “This was disclosed although was not determined to be a conflict,” the CDC told us in an email.
What about royalties?
As we said, one of the conditions of ACIP membership is that members can’t be holders of or entitled to royalties or compensation for a patent for vaccine products or processes that “may come” before the ACIP during their tenure. And although a waiver could be granted if the need of a member’s services outweighs the potential conflict of interest, the CDC told us that it “has not provided a waiver based on a patent since these policies and procedures were first drafted over 20 years ago.”
What about the FDA’s Vaccines and Related Biological Products Advisory Committee?
The Vaccines and Related Biological Products Advisory Committee is one of 31 committees used by the Food and Drug Administration to get independent expert advice on different issues. The VRBPAC, composed of 15 voting members, reviews and evaluates data on the safety and effectiveness of vaccines and other biological products intended to prevent, treat or diagnose diseases.
The FDA privately screens members of all advisory committees before every meeting, requiring them to provide information of their financial interests to detect potential conflict of interests. The agency evaluates “potentially disqualifying interests or relationships” before meetings and make changes to the rosters if needed, an FDA spokesperson told us in an email.
“For the VRBPAC meetings focused on the COVID-19 vaccine EUAs, the FDA screened and cleared all committee members and consultants for any relevant disqualifying interests or relationships, per our established standard practice, prior to their participation,” the FDA’s Abby Capobianco wrote.
What do they have to disclose?
VRBPAC members are also considered Special Government Employees, and therefore are required to file financial disclosure reports. But instead of filing OGE Form 450, members of FDA advisory committees use an alternate confidential financial disclosure report — FDA Form 3410 — which they have to file prior to each meeting.
The report asks members to disclose any involvement or financial link that they, their family, their employer or other organization they are associated with have with the products or issues to be discussed at the meeting. Those include current investments, employment or grants, and also past financial interests or other involvements. The FDA then reviews the reports to determine if there is any direct conflict of interest with the issues to be discussed in the meetings, or something that may create the “appearance” of a lack of impartiality.
If the FDA determines there is a “direct and predictable effect” on a member’s financial interests, he or she will not be able to serve on the FDA advisory committee for that matter. The FDA can grant the member an exception or a waiver to serve on the advisory committee if the FDA determines the conflicts of interests “are too remote or too inconsequential to affect the integrity of the services” or if the need for the member’s services “outweighs the potential for a conflict of interest.”
Is it publicly available?
No, the reports are confidential.
What about royalties?
FDA Form 3410 requires members to disclose patents, royalties and trademarks and indicate if they are related to the products, indications or issues to be discussed at the upcoming meeting. If they are related, the member is required to indicate the income received. The FDA then reviews the information for conflicts of interest, as we described above.
Editor’s note: FactCheck.org does not accept advertising. We rely on grants and individual donations from people like you. Please consider a donation. Credit card donations may be made through our “Donate” page. If you prefer to give by check, send to: FactCheck.org, Annenberg Public Policy Center, 202 S. 36th St., Philadelphia, PA 19104.
The post Q&A on Financial Disclosures by Government Scientists appeared first on FactCheck.org.
This post was originally published on FactCheck.org.
-
One million deaths. An unthinkable milestone when this pandemic started — and even this gruesome number doesn’t capture who and what we have lost. One million lives lost, dreams unfulfilled, families heartbroken and futures cut short. This loss is unimaginable, and we have only just begun to scratch the surface of how our communities will continue to grapple with this mass death and violence, surely for generations to come. According to the Centers for Disease Control and Prevention, COVID-19 has become the third leading cause of death in the United States, after heart disease and cancer.
As a working Latina mother of two, I feel the ongoing pain and frustration of the pandemic in so many ways. I have lost family members and neighbors to COVID — both old and young. My children, isolated and separated from their best friends during a time in their lives that should be filled with joy and connection, struggled with their mental health and lost critical in-person education. My elderly father had a crushing fall, and his physical therapy, and path to wellness, was greatly delayed. My aunt, Lilia, who suffered from Lupus, died alone because none of us could be with her.
Amid all of this pain, President Joe Biden has dropped most pandemic restrictions, stopped most national tracking, and failed to act on even the most basic federal actions to reign this pandemic in. Disabled and chronically ill Americans have been left adrift — in a maskless world many of my colleagues and friends are unable to safely leave their homes.
We need swift, immediate action at a global level. Fighting this pandemic as if we can defeat it alone has failed. It’s time: President Biden must work with Congress immediately to ensure that supplemental COVID funding includes significant global investments to end the pandemic. Our lives are at stake — and we cannot wait another moment.
Heading into our third year of the pandemic, billions worldwide still don’t have access to COVID vaccines and treatments, continuing to suffer even as pharmaceutical companies reach record profits. Globally, less-wealthy nations have been abandoned to vaccine apartheid, as pharmaceutical companies are selling and distributing vaccines, tests and treatments almost exclusively to wealthy nations. Here in the U.S., it’s communities of color, low-income people and the disabled who face the greatest burden of COVID-19, in terms of death rates but also economically and socially. Those working in lower-wage fields like food and agriculture, warehouse operations, transportation and construction saw higher rates of death than in most other occupations. Working in a nursing home has become one of the deadliest jobs in the country.
The consequences of this pandemic are far reaching and devastating, not just for those we have lost but for the ones they’ve left behind. We have the tools and resources necessary to support our communities and fight health inequity right now — but it’s clear that what is missing is the political will to do so.
Our nation hasn’t seen mass death on a scale like this since World War II, when about 418,000 Americans died. The Atlantic’s Ed Yong puts it into perspective: “The U.S. reported more deaths from Covid-19 last Friday [March 4] than deaths from Hurricane Katrina, more on any two recent weekdays than deaths during the 9/11 terrorist attacks, more last month than deaths from flu in a bad season, and more in two years than deaths from HIV during the four decades of the AIDS epidemic.”
Where is our great reckoning of this mass violence and pain? And more importantly, where is the political will to fight for our futures, for our families, for a road ahead away from this destruction and toward justice, equality, health and resources for all those still suffering and at risk of death?
Since it rejected a $15 billion supplemental for pandemic preparedness that included global vaccine outreach and funding for free vaccines and testing here in the U.S., Congress has not provided us with the funding we need to continue a robust COVID response, even amid new variants and continued pandemic-related economic stress. With cases rising abroad, experts are sounding the alarm that we should expect a rise in cases here in the U.S. as well. Failure to adequately fund these efforts now will have severe and far-reaching consequences, impacting our ability to deal with a future surge.
Moreover, despite widespread messaging that COVID testing is free, many patients have found themselves facing bills for testing — some for over $1,000. According to The New York Times, about 2.4 percent of coronavirus tests billed to insurers in 2020 left the patient responsible for some portion of payment, adding up to hundreds of thousands of Americans who received unexpected bills. Patients were left with these high bills due to gaps in protections that Congress and the Trump administration put in place early in the pandemic — and our communities are still suffering. While ensuring that people trust the vaccine is a high priority, it is also critical that unexpected costs for testing and treatment don’t deter individuals from getting vaccinated.
As we work to ensure the safety of the global community, Democrats must pass supplemental funding without giving in to Republican demands to tie COVID funds to oppressive immigration policies. We cannot allow partisan distractions and anti-immigrant cruelty to distract from this urgent need. The time to act is now, and we cannot leave anyone behind.
A new way of life is here — seemingly forever. But adjusting to the “new normal” is hardly enough, not when an average of 26,000 new cases are recorded every single day, bringing with them the threat of more death, more loss, more futures taken too soon. Mask mandates are being lifted across the country. We have no national funding to support those infected. Uninsured Americans have little to no support.
The time to act has long gone by — our communities, our children and our families deserve better.
This post was originally published on Latest – Truthout.
-
As the Biden administration contemplates its options in the wake of a judge’s ruling ending mask mandates for federally-regulated travel, a new poll shows that a majority of Americans would likely have supported keeping masking rules in place, at least through May.
The Centers for Disease Control and Prevention (CDC) recently extended a mask mandate on travel — including on buses, trains and planes — until May 3. But a ruling earlier this week from Florida U.S. District Judge Kathryn Kimball Mizelle abruptly ended those rules, finding them unconstitutional and inconsistent with the laws defining the regulatory powers of the CDC.
In response to the ruling, several major airlines have already relaxed their rules on masking, making mask-wearing optional for passengers. However, many legal experts have questioned the soundness of the arguments Mizelle made in her ruling, pointing out that the judge took statutory terminology out of context when she made her decision. The Department of Justice (DOJ) has said that it will soon decide whether to appeal Mizelle’s ruling to a higher court.
That decision will rest on the CDC’s opinion on whether masking rules are needed, the Justice Department said. In other words, if the CDC thinks the mandate can be allowed to expire — if it believes, for example, that it’s close enough to the original May 3 deadline, and that there wasn’t a high likelihood it would have needed to issue another extension — the DOJ may not appeal the decision at all.
However, not seeking an appeal could create a dangerous precedent for how the U.S. can react to future pandemics, based on the unusual interpretation Mizelle made in her ruling.
Recent polling shows that a majority of Americans support keeping mask mandates for travel in place.
A Politico/Morning Consult poll conducted just before Mizelle’s ruling was issued asked respondents to give their opinion on the CDC’s decision to extend the mask mandate for travel to May 3. Close to 6 in 10 Americans (59 percent) said they backed that decision, while only 32 percent said they opposed it.
In a separate question on the subject, 49 percent of respondents said that it was “too early” to end any rules on masks for travel — outweighing the combined 43 percent of respondents who said it’s the right time to end the mandate, that the mandate should have already ended, or that it never should have been in place to begin with.
Many are clamoring for the Biden administration to appeal Mizelle’s ruling, particularly due to the way she was appointed to her position. An appointee of former President Donald Trump, Mizelle was deemed “not qualified” by the American Bar Association for her lack of experience, but was approved by the then-Republican-controlled Senate to her post. While she has clerked for several judges, Mizelle has never actually held a judgeship herself, much less even argued a case on her own. (Mizelle’s only trial experience, prior to becoming a judge, was as an intern.)
Her decision to end the mask mandate for travel comes as the coronavirus pandemic — particularly the BA.2 subvariant — continues to pose a threat to the U.S. and the world. More than 400 individuals in the country are dying each day, on average, and with recorded COVID cases increasing by 47 percent over the past two weeks, that number is likely to go up.
Nearly 990,000 Americans have died of COVID-19 so far since the start of the pandemic, with more than 80 million cases recorded since March of 2020.
This post was originally published on Latest – Truthout.
-
The Centers for Disease Control and Prevention (CDC) announced the termination of the harmful Title 42 expulsion policy on April 1, but immigration advocates are frustrated that the implementation won’t begin until May 23. According to the CDC website, the extra time is meant to implement COVID-19 mitigation protocols, including COVID-19 vaccinations for migrants and preparing for the resumption of regular migration under Title 8, which lists an extensive series of reasons why a person could be deported, including having committed a crime within five years of being admitted into the U.S., violating a protective order, and being found in possession of drugs. It was a welcome announcement for immigration advocates who have been fighting for the end of what they say is a racist policy. But advocates say many questions remain with regards to implementing the end of the policy and, most importantly, that migrants seeking safety cannot wait almost two months for help.
“The announcement to terminate Title 42 is long overdue,” said Haddy Gassama, the UndocuBlack Network’s national director of policy and advocacy. “Organizations such as UndocuBlack and Haitian Bridge Alliance and many others have been pushing for the end of this policy for pretty much the two years since its inception. But, we weren’t able to celebrate immediately because there were so many questions around the implementation of that termination and what it would look like. There’s still quite a bit of advocacy, but it’s certainly a welcomed first step.”
Title 42 is a 76-year-old, World War II-era public health law that allows the CDC to bar certain individuals from entering the U.S. if it fears the spread of diseases or viruses. In March 2020, former President Donald Trump enacted the policy, despite the CDC’s scientists saying there was no evidence it would slow the spread of the coronavirus. Since then, President Joe Biden has continued the illegal policy of denying lawful asylum and turning away the vast majority of migrants at the U.S.-Mexico border. Under the policy, the U.S. has expelled over 1.7 million people at the Southern border without due process, with recidivism rates soaring immediately after the policy was enacted.
Advocates say the policy exposes migrants to violence in Mexico, deprives them of their right to seek lawful asylum, forces them to return to the dangerous and unstable conditions they were trying to flee in the first place, and disproportionately impacts Black and brown migrants. According to Witness at the Border, there have been 175 ICE Air removal flights to Haiti since September 2021, returning around 19,000 Haitian migrants. Since January 2021, there have been 212 ICE Air return flights to Haiti, returning about 21,000 Haitian migrants. As the clock continues to tick until May 23, migrants will continue to be expelled under the policy.
“The harm that Title 42 is inflicting is still happening,” said Ronald Claude, the director of policy and advocacy for Black Alliance for Just Immigration (BAJI). “There is a lot of concern about what is to come and how that is going to negatively impact Black migrants.”
Claude and other advocates are concerned the termination of Title 42 will result in more enforcement of “Remain in Mexico,” another policy that deters migrants and asylum-seekers from safely entering the U.S. “Remain in Mexico,” or “Migrant Protection Protocols,” makes them wait in Mexico during their immigration proceedings.
“We can’t switch one evil for the other,” said Cynthia Garcia, United We Dream’s national campaigns manager for community protection. “We have to continue to build out an infrastructure that advances racial justice in the immigration lens.”
Claude said there should be a community-oriented approach to welcoming migrants into the country that collaborates with advocates for the Black migrant community to create a “fair, just, compassionate, and dignified system that was promised from the onset of this administration and that has not been reciprocated.”
Garcia said the Biden administration should support border community groups that are already supporting migrants by connecting them with health care, secure housing, and the ability to provide for their families.
“Instead of falling for the false choice of increasing the budget for ICE and CBP, or increasing the number of detention centers, we should actually increase funding for community centers, for relief for folks to have access to health care,” Garcia said. “That doesn’t just impact immigrants, it impacts the community at large.”
The news follows the Biden administration’s national messaging that the COVID-19 pandemic is in decline and the public can return to normal life. In March, the breadth of Title 42’s implementation was also limited. The U.S. Court of Appeals for the District of Columbia said the administration could not send migrants to countries where they would face persecution or torture. Separately, the CDC terminated the policy for unaccompanied minors altogether. Advocates say the termination should apply to all migrants, regardless of demographics, including single adults.
“Prioritizing family units over single adults could result again in disproportionately harming and endangering not only Black migrants, but also migrants who identify as LGBTQ+ who oftentimes present at the southern border as single adults,” Gassama said. “This interim period is one that is very dangerous. We hope that between now and May 23, while the administration is getting their ducks in a row, that there shouldn’t be any expulsion flights.”
Since the CDC made its announcement, Republican lawmakers have been trying to pass a coronavirus relief bill with a Title 42 amendment by the end of this week. Additionally, three Republican-led states (Missouri, Arizona, and Louisiana) have already sued the Biden administration over the decision to lift Title 42.
“We need to be able to push back against that harmful narrative that Republicans are driving,” Garcia said. “We need to continue to push against the fearmongering and lean into the Biden administration to continue to open up the asylum process.”
Until May 23, Claude, Garcia, and Gassama say they want to see the complete end of Title 42 immediately, for the Biden administration to fully restore the asylum system, and to create a process for addressing the millions of migrants who were unjustly deported under the policy.
“This decision is the result of the hard work and fighting of almost two years from Black immigrants rights organizations and local community members,” Gassama said. “But we know the fight is far from over.”
Prism is an independent and nonprofit newsroom led by journalists of color. We report from the ground up and at the intersections of injustice.
This post was originally published on Latest – Truthout.
-
Released four days before the State of the Union, the new CDC measures and the narrative they created let President Biden claim victory over the virus via sleight of hand: a switch from standard reporting of community transmissions to measures of risk based largely on contentious hospital-based metrics. The previous guidelines called anything over 50 cases per 100,000 people “substantial or high.” Now, they say 200 cases per 100,000 is “low” as long as hospitalizations are also low.
The resulting shift from a red map to a green one reflected no real reduction in transmission risk. It was a resort to rhetoric: an effort to craft a success story that would explain away hundreds of thousands of preventable deaths and the continued threat the virus poses.
The post The CDC Is Beholden To Corporations And Lost Our Trust. We Need To Start Our Own appeared first on PopularResistance.Org.
This post was originally published on PopularResistance.Org.
-

From the federal mask recommendations suspended in May to White House COVID coordinator Jeffrey Zients’s December pronouncement that the unvaccinated are to blame for “the hospitals you may soon overwhelm,” the Biden administration has organized its COVID response around an ethos of personal responsibility.
COVID is spun as a pandemic of the unvaccinated even as the vaccinated can also spread the virus. Vaccines and their boosters, importantly protecting the vaccinated from hospitalization and death, appear nothing of the public health silver bullet they’ve been positioned to be, presently offering only 10 weeks’ protection against symptomatic infection with the now circulating Omicron variant.
Such a campaign against the unvaccinated represents both bad politics and bad public health.
Many of the unvaccinated aren’t ideologically motivated. Skepticism and hesitancy mark as much a failure of vaccine access, including the absence of a national door-to-door campaign to convince the 84 million Americans walking around without a single COVID shot to get vaccinated or to physically transport them to an appointment. Winning their trust is critical in controlling the outbreak stateside.
Other patients may refrain from vaccination even when it puts them in great personal danger. Jesse Rouse, photographed here in November suffering his second bout of COVID in Minneapolis, was reported to be unvaccinated at the time after he previously underwent a double lung transplant. Researchers have proposed that lung transplantees are especially vulnerable to respiratory infection and should be vaccinated for COVID.
Some people may refrain from vaccination for medical reasons – including confusion or conflicting information about how vaccination might interact with their health conditions or treatments.
Regardless of why particular people remain unvaccinated, thrusting culpability fully onto individuals is a harmful move. Like Ronald Reagan’s campaign against “welfare queens,” presuming public health problems emerge primarily from bad actors and individual decision-making obfuscates the systemic and structural roots of the failure of the U.S.’s response to the pandemic.
Much like Trump, the Biden administration appears repeatedly intent on turning the COVID page, no matter the state of the pandemic itself. The May mask recommendations, which stated that vaccinated people could stop wearing masks in most indoor spaces, were textbook on that account. The administration later ignored an October report from public health experts recommending free testing at a pace of 732 million tests per month in preparation for a holiday COVID surge:
The plan, in effect, was a blueprint for how to avoid what is happening at this very moment — endless lines of desperate Americans clamoring for tests in order to safeguard holiday gatherings, just as COVID-19 is exploding again.
Yesterday, President Biden told David Muir of ABC News, “I wish I had thought about ordering” 500 million at-home tests “two months ago.” But the proposal shared at the meeting in October, disclosed here for the first time, included a “Bold Plan for Impact” and a provision for “Every American Household to Receive Free Rapid Tests for the Holidays/New Year.”
Early in December, Biden spokesperson Jen Psaki scoffed at reporter Mara Liasson’s query about why the U.S. doesn’t just pay for home COVID tests for every American household like other countries do instead of making Americans submit for reimbursement from insurance companies that have routinely failed to pick up the bill. “How much is that going to cost?” Psaki asked.
Should a government that had voted $768 billion for the Pentagon, $24 billion more than Biden requested, just pay for COVID tests? Yes, April Wallace replied in the Washington Post. Yes, it should:
I am a dual citizen of the United States and Britain, now living in Edinburgh, Scotland, and I am able get rapid antigen tests anytime I want to, at no cost and with no hoops to jump through. I know that Americans pay more than $20 for a package of two tests — if they’re in stock. Here you can walk into your local pharmacy, and they will just hand you packs of seven tests at no charge. In my neighborhood I can also go to the local recreational center and collect packs of tests free for my family, or swing by a coronavirus testing center.
It turns out the reimbursement for home tests wasn’t to start until mid-January anyway:
The administration has already said that the plan will not provide retroactive reimbursement for tests that have already been purchased, which means that any tests you buy for the holidays will not be covered.
The Biden no-plan, expanded to a whole four rapid tests per household and three masks for each American, appeared to be phase one of a campaign of further eroding American expectations. As self-described “shitposter” @fingerblaster tweeted about what’s missing:
Wild that the most unhinged republican president in history sent us $2000 checks back when we had like 12k cases a day and now we have 300k cases a day and a dem president who’s like “lol not my problem go to work jack”
The more august New York Times reported on the end of monthly child benefits millions of Americans were depending on:
The end of the extra assistance for parents is the latest in a long line of benefits “cliffs” that Americans have encountered as pandemic aid programs have expired. The Paycheck Protection Program, which supported hundreds of thousands of small businesses, ended in March. Expanded unemployment benefits ended in September, and earlier in some states. The federal eviction moratorium expired last summer. The last round of stimulus payments landed in Americans’ bank accounts last spring.
These benefit programs, as modest as they were, saved thousands of Americans from COVID deaths.
A March 2021 FamiliesUSA report summarized research showing a third of COVID deaths were tied to the lack of health insurance. The effect was multiplicative: “Each 10% increase in the proportion of a county’s residents who lacked health insurance was associated with a 70% increase in COVID-19 cases and a 48% increase in COVID-19 deaths.”
Controlling for stay-at-home orders, school closures and mask mandates, another study, first posted November 2020, estimated that lifting eviction moratoriums state-to-state resulted in between 365,200 and 502,200 excess coronavirus cases and between 8,900 and 12,500 excess deaths.
Omicron’s Delta Strain
So, public health clearly extends beyond necessary prophylaxes into necessary social interventions. But if there was any doubt about which constituency the political class serves instead, in December, the Centers for Disease Control and Prevention (CDC) cut down its recommendation for quarantine upon COVID exposure from 10 days to five. The act was decidedly in response to pressure from employers, notoriously Delta Air Lines’ CEO Ed Bastian in a letter that Delta proudly posted.
The Delta letter summarized the scientific literature in favor of its request in two sentences. The science is in reality more nuanced, marked by a variety of definitional complications.
Omicron, like new variants before it, is almost certain to evolve out from underneath the vaccine effectiveness that Delta Airlines cites as, full-stop, protection enough. Permitting COVID variants to circulate on Delta planes or elsewhere increases the chances they can evolve enough to circumvent medical and non-pharmaceutical controls.
Other drawbacks refute such summary boosterism. Omicron is already associated with increased reinfection. The variant’s other impacts on clinical courses and epidemiology are likely to be geographically specific, depending on a variety of local factors, including pre-existing immunity and the state of non-pharmaceutical interventions. What works as an intervention under one set of conditions does not necessarily hold under all.
More meta, the speed at which new variants are being allowed to evolve is outpacing even the frantic pace of the research conducted. “Flattening the curve” extends beyond our hospitals to research efforts aimed at discovering how to better control COVID.
In other words, under a more infectious Omicron, a variety of interventions, one layered atop another, is necessary, rather than stripping them back to serve criteria pretending to be scientific.
This isn’t the first time the airline industry tried to bend basic COVID science to its financial advantage. JetBlue CEO and reopen proponent David Neeleman funded and helped coordinate a Stanford University study that whistleblower complaints showed used a testing kit that erred on the side of false positives. By these tests, the study concluded the COVID virus was more widespread in the public and therefore, given the underlying number of deaths in the study population, was less dangerous of a pathogen.
National Institute of Allergy and Infectious Diseases Director Anthony Fauci, proving Lysenko on the Potomac, ran interference for Delta and other employers in the face of the twists and turns obvious in the COVID literature. Fauci parroted Bastian’s arguments nearly to the letter:
There is the danger that there will be so many people who are being isolated who are asymptomatic for the full ten days, that you could have a major negative impact on our ability to keep society running. So the decision was made of saying let’s get that cut in half.
CDC Director Rochelle Walensky once fought back tears over the likelihood of COVID mass deaths. Now, like a meat plant manager thinking only of the bottom line, she defends sending people back to work still infectious:
There are a lot of studies [from other variants] that show the maximum transmissibility is in those first five days. And [with Omicron] we are about to face hundreds of thousands more cases a day, and it was becoming very, very clear from the health care system that we would have people who were [positive but] asymptomatic and not able to work, and that was a harbinger of what was going to come in all other essential functions of society.
In short, the combination of economic compulsion and traumatic bonding that sent millions of workers into unprotected workplaces the pandemic’s first two years now represents state policy. The denialism for which liberals punch down on Trumpists is the labor law of the land. It is now a key part of the administration’s public health campaign.
“I’m not letting COVID-19 take my shifts,” one recent CDC ad declared. “My job puts me at high risk for COVID-19 exposure. I got vaccinated because it’s better to be protected than to be out sick.”
Another CDC post shamelessly used the U.S.’s privatized health care system as a cudgel of class discipline: “Hospital stays can be expensive, but COVID-19 vaccines are free. Help protect yourself from being hospitalized with #COVID19 by getting vaccinated.”
In that spirit, Biden economic advisor Jared Bernstein waxed optimistic on the economy. The depletion of personal savings would drive low-paid workers back into the labor market during a pandemic, Bernstein cheered.
“We are intent,” Jeff Zients declared mid-December, “on not letting Omicron disrupt work and school for the vaccinated. You’ve done the right thing, and we will get through this.” The vaccinated are presented as pure enough of soul to get back to working the gears of the economic machine. The unvaccinated are cast, to appropriate Hillary Clinton’s characterization, as a basket of eschatological deplorables.
Zients, a Biden campaign donor, was the CEO of investment firm Cranemere and director of Obama’s National Economic Council before becoming COVID czar with no public health experience. His primary portfolio of priorities was always apparent.
The quarantine switcheroo follows CDC’s changing recommendations for school distancing from six feet to three, which it now pretends is the virus’s limit. In reality, even six feet isn’t enough for the airborne virus. But in changing it to three, CDC could legally accommodate efforts to stuff students back in brick-and-mortar schools without changing day-to-day public health precautions.
Keeping kids out of school can have terrible impacts on learning outcomes and emotional well-being. Keeping kids in school, potentially leading to the deaths of other students or teachers in school, and older adults back home, can incur a different kind of emotional damage. Both risks serve as more the reason for bringing the outbreak under control with a full-spectrum intervention.
The CDC’s position, sending students back to school without controlling the outbreak, is geared toward other aims. It’s about putting the economic cart before the epidemiological horse. The kids need to go to school so that the parents can go to work.
Such misguided campaigns extend beyond the administration. Among the American Heart Association’s new interim pandemic recommendations for medical staff is starting CPR without personal protective equipment.
Artist Rob Sheridan designed a series of counter-CDC posters:
- We Can Do It! We Can Sacrifice Grandma So Dave & Buster’s Can Stay in Business!
- Quiet! Don’t Cough! Pretend to be OK! Your Boss’s 8th Boat Depends on It!
- America’s Youth is Ready to March Back to School! The Economy Demands Sacrifice!
Across the internet — over the political spectrum — other observers expressed outrage in scathing terms:
- Comedian Zak Toscani: CDC recommends splitting up your quarantine over your two 15 min breaks.
- Sociologist Jennifer Jennings: I guess I missed that rewrite of the Hippocratic Oath: first, do no harm to late capitalism.
- Comedian Roy Wood Jr: CDC just said you only need to quarantine if you on a ventilator. But if ya ventilator got wheels and a battery pack you gotta take yo ass to work.
- Songwriter Certified Lover Girl: Y’all keep talking about the CDC, the CDC, the CDC….The CDC left you fa dead hoe.
- Author Alexander Chee: If you have to deploy the military to support hospitals you may have spent your budget on the wrong part of the system given the challenges we actually face.
- Designer Char: CDC okays pull-out method as “eh, good enough.”
The administration is too full of itself to see it is losing the country. Its caustic claims about “the science” aren’t supported by the science, further undercutting research as a trusted source of both state strategy and public response.
The original 10-day quarantine that the CDC changed was grounded in the evidence-based realities of the virus itself, specifically its incubation time, generation time and serial interval. At the same time, the 10 days aren’t a matter of essentialist measures of central tendency.
Against CDC Director Walensky’s characterization, it’s about the variation in patients’ infectious periods. Some patients exit out of their infectiousness early, in the five days Walensky cited. Others can be infectious much longer. No one knows who’s a late bloomer in transmission. As a matter of practical public health intervention, it’s an unknown.
A public health campaign must therefore institute mask and quarantine policies that cover for the late transmissions, so that they don’t serve as the means by which the outbreak rolls on — particularly as Omicron’s infectiousness approaches that of measles and a 100% attack rate can still result from even a small group of infectious people walking around.
Instead, we have slashed public assistance, shortened quarantines, offered no-to-little remote schooling, hired few community health workers, conducted little genomic sequencing of the virus, and let hospitals get overrun. The CDC gave in upon the subsequent furor around the shortened quarantine by adding only a recommendation — not a requirement — of a negative rapid antigen test before workers returned to work.
Beyond trying to circumvent the rancor of partisan criticism, why did Trump and Biden alike aim at pretending the pandemic away? Biden’s trajectory is illustrative that capitalist realism has a way of eating away at even good faith efforts at addressing existential threats.
In October 2020, candidate Biden put the failings of his opposition in perspective: “We’re eight months into this pandemic, and Donald Trump still doesn’t have a plan to get this virus under control. I do.”
“This crisis,” President-elect Biden added, “demands a robust and immediate federal response.”
A year later, President Biden pivoted: “There is no federal solution. This gets solved at a state level,” months after many state governors had lost or abandoned their emergency powers to impose mask mandates and shelter-at-home orders.
Other countries see federal jurisdiction differently, as if the very health of their ostensible constituencies has something to do with governance.
While the U.S. daily breaks record COVID caseloads, some other countries appear to be of another world. COVID long-hauler Ravi Veriah Jacques reported these January 2 caseloads from abroad:
- New Zealand – 51
- China – 191
- Taiwan – 20
- Japan – 477
- Hong Kong – 18
China’s reactions are both broader and triggered more quickly, with the public health results to show for it. Xi’an, a metropolis of 13 million people in Shaanxi Province, underwent an arguably arduous lockdown upon the emergence of 175 COVID cases. Western media has played on the difficulties in obtaining food in the city over the 12 days’ quarantine, but not the campaigns to alleviate those problems.
Some may argue the Biden administration’s reaction is better late than never, but that’s not how controlling COVID’s lightning strikes works.
As epidemiologist Rodrick Wallace models, whatever the intervention, there’s nothing worse than dithering. Given the insidious nature of the virus, we are routinely six weeks too late if spikes in cases, rather than anticipatory planning, are the trigger. Repeated delays mark U.S. COVID planning — among them, the spread of the original wave out of coastal cities to the rest of the country in spring 2020 and the arrivals since of Delta and Omicron stateside.
Rapid Confusion Test
It happens that the mass at-home testing the Biden administration passed over in October, setting up a program several months too late, is itself already a failure. Big picture, like vaccination, it represents yet another technicist intervention that, while necessary, is also insufficient. It’s more of a grand gesture that detracts from the administration’s refusal to pursue multilevel systemic public health programming.
The specifics of such a rollout and the tests themselves also get in the way. It’s much more than a matter of rapid tests permitting an exit out of the shots for the deplorable unvaccinated, as the Biden administration feared. It’s also not merely a matter of doctors defending their testing territory, as rapid test proponents argued.
Among several intrinsic errors that biotech consultant Dale Harrison explores around the rapid tests, there is the difficulty of self-administering them:
One important note is that at-home antigen tests will give VERY poor results (both high false-positives and high false-negatives) if you are sloppy or misuse them.
These are complex molecular assays and the EXACT usage is critical. You MUST read and follow every single detail in the instructions to get a reliable outcome….
The difficulties extend beyond administering the tests. Interpreting them is a difficult task; it is swayed by our hopes as well as by technical matter:
Now comes the tricky part… what happens if you get conflicting test results.
Let’s say you get a positive result on an at-home antigen test (like the BinaxNow) and decide to take it again “just to be sure”.
Then you get a negative result on the 2nd Binax test. Now you schedule an appointment to get a PCR test.
A couple of days later, it comes back negative.
ARE YOU INFECTED? Absolutely positively YES!
If you’re non-symptomatic and get a [Binax+ Binax- PCR-] set of results … a positive and two negatives in any order.
In that case, it is 56-times MORE likely that you’re infected than not infected … 5600% more likely!
And if you’re FULLY symptomatic and get a [Binax+ Binax- PCR-] set of results, it is 20-times MORE likely that you’re infected than not infected … 2000% more likely!
Even if you get ANOTHER PCR test and THAT test comes back negative as well [Binax+ Binax- PCR- PCR-] you are still 4-times more likely to be infected than not … 400% more likely!
And it does NOT matter the order of the test results … the math holds true regardless.
Even medical doctors conducting these tests in clinics stumble:
I know this seems VERY counter-intuitive and even most doctors who prescribe these tests (other than Infectious Disease specialists) tend to NOT understand this!
And when faced with multiple conflicting test results, most medical people will incorrectly select the LAST result as the “correct one”.
This is a DANGEROUS mistake! Again, outside of certain specialties, few medical staff are trained to think in terms of Bayesian statistics.
Vanity Fair’s palace intrigue set the COVID Collaborative of high-end epidemiologists recommending the holiday testing surge against the administration that ignored them. But that isn’t quite right. Both sides agree on turning public health into an individualistic (and commodifiable) option:
Once [ex-Harvard epidemiologist and now chief science officer at the eMed diagnostic company Michael] Mina began to advocate for rapid home tests, he encountered the same mindset: doctors “trying to guard their domain.” Some doctors had long opposed home testing, even for pregnancy and HIV, arguing that patients who learned on their own about a given condition would not be able to act on the information effectively. Testing, in this view, should be used only by doctors as a diagnostic instrument, not by individuals as a public-health tool for influencing decisions.
The U.S. approach sticks the American people with the job of administering and then interpreting the conflicting results of multiple tests. The false positives might be low in part because nearly 100 percent specificity aligns with peak viral load. But, as Harrison describes, even should the test be administered correctly, the false negatives are legion and the results of one test do not necessarily change the implications of previous ones.
Techno-utopianism offers another iteration of blaming the victim if the outcome goes south: “It’s your own fault you didn’t do the test right.” Don’t let the easy lines on the lateral flow ag card confuse matters. Against Mina’s insinuation, it’s decidedly unlike a pregnancy test.
There is also the matter of what happens when organizing society’s access to work and recreation around such tests collides with a run on the tests at local stores already suffering supply chain problems, making the tests both unavailable and priced beyond working people’s budgets.
If, on the other hand, the Biden administration hired and trained a million community health workers to go door-to-door across the country administering these tests for free — like really free — we wouldn’t be in such a free-for-all, if you’ll excuse the phrasing.
If such teams had been put in place from the beginning, they may have been able to build the trust necessary to successfully introduce a variety of time- and place-specific public health interventions that would likely have minimized the duration and impact of each wave of the pandemic.
Surprising the Supposedly Surprised
What’s interesting about Harrison’s direct and clearly written posts is that his recommendations are framed by the context of what the U.S. can, or is willing to, offer right now: not much.
Yes, everyone should be able to test themselves whenever they wish, all the time. But the U.S. chooses to position itself as unable to pursue such a public health program. Should the sensitivity and specificity reported on the test boxes match their actual outcomes? Yes, they should, however righteous the original testing went into bringing the products to market. Should the efficaciousness and effectiveness of vaccines match? Yes, that would be nice.
There are expectations that individual American consumers hold about solutions — cheap and immediately effective — that the market repeatedly promises but can’t deliver. In this case, the multifactorial virus doesn’t cater to such an ideal of a single packet solution. And the public health response we need, and the market treats as a rival, is starved to near-death.
The U.S. government, and governments around the world, treat the capitalism that helped spring the COVID virus out of commoditized forests as more real than the ecologies and epidemiologies upon which the global system depends. To protect that mirage of a difference, each new variant that has since emerged is strangely presented as the beginning of the pandemic’s end, resetting the next round of denialism, instead of alerting us that in reality, without a change in public health practice, we’re caught in a daisy chain of viral evolution.
Each “surprise” that the COVID virus refuses to cooperate with such an expectation, acting in its own interests instead of ours, also serves to protect the system from the implications of its refusal to act. Surprise — pretending we don’t know what we know — is itself an ideological project. The business of governing a system in decline, after all, is about managing expectations. All is well, get back to work, until, suddenly, it isn’t, as it always was.
From the virus’s vantage, the resulting public health dithering and half-measures serve the virus as both escape hatch out of our control efforts and selection pressure to evolve around those campaigns. A combo that leads to the worst of epidemiological outcomes.
If we wish to unplug out of this trap, we have to organize together against our rulers and their financers. We must deploy a full-spectrum intervention that drives the COVID virus under its rate of replacement.
That requires we reject not only Washington’s business bipartisanism, but also the core model of our economy around which our civilization is organized. That’s no small matter, of course, but with climate change and other pandemics also in the wings, likely our sole option out.
This post was originally published on Latest – Truthout.
-

When Cherriese Thompson heard the Centers for Disease Control and Prevention’s decision last week to cut quarantine time down from 10 days to five days, she was upset. At a time when hospitalizations were surging and isolation and quarantine procedures were already tricky for people to understand, Thompson, a third-year medicine resident in Northern California, felt the short quarantine window would only add confusion and put more people at risk of contracting the highly contagious Omicron variant.
“It’s just so upsetting,” Thompson said. “I feel like this is going to end up fueling the surge even more. It’s come to the point that we value money more than we value people’s livelihoods.”
The CDC made the decision to reduce the amount of time asymptomatic people with COVID-19 infections have to quarantine in order to ease labor shortages for the stressed airline industry. But health care workers say the new guidelines are ignoring their needs when hospitals are already in the midst of a surge and dealing with critical staffing shortages. Now, they say shorter quarantine times could only add to an already stressed health care system and disproportionately impact BIPOC health care workers and patients.
A recent study by Mercer found that the U.S. is facing a severe health care worker shortage and that by 2025 the country will lose approximately 29,400 nurse practitioners. The U.S. Bureau of Labor Statistics reported in December that hospitals had lost 9,000 jobs during October alone. Since the beginning of the pandemic, health care employment has dropped by 524,000. According to the World Health Organization, about 115,000 health care workers died from COVID-19 between January 2020 to May 2021. In Los Angeles County alone, more than 49,000 health care workers and first responders have been sick with the virus since February 2020. According to data collected by Fierce Healthcare, about 11,000 health care workers in 58 health care systems across the country have been fired or resigned due to a refusal to meet vaccine mandates.
On the same day the guidance was issued, Thompson began developing symptoms of COVID-19. She had visited family in Maryland over the holidays when her grandmother developed some symptoms. She’d received her booster shot of the vaccine, but her grandmother was still experiencing a high fever and Thompson had to consider taking her to the hospital. But, being a Black Jamaican woman, Thompson was unsure her grandmother would receive the best care possible due to the implicit racial bias that makes white health care workers less likely to believe Black patients. In a 2003 study by the National Academy of Medicine, they found that “racial and ethnic minorities receive lower-quality health care than white people — even when insurance status, income, age, and severity of conditions are comparable.”
“I was terrified to take her to the hospital,” Thompson said. “I was thinking, ‘At least I’m the best person to advocate for her because I’m in health care,’ but we’re still Black women.”
Thompson was eventually able to break her grandmother’s fever at home and give her the care she needed so that her health improved, but by the time she got back to California, her father began developing symptoms as well.
“I’m going to need to fly over there and advocate for my dad,” Thompson said. “I’ve witnessed the disparities in the micro- and macroaggressions and the inadequate care that people of color have experienced, in general, and then exacerbated by COVID.”
On Friday, Dec. 31, Thompson considered taking herself to the hospital because her oxygen levels dropped to 92% and she was short of breath. Fortunately, Thompson’s symptoms stabilized and her clinic decided to continue following a 10-day quarantine guideline for now.
“I think [the CDC’s] response is inappropriate especially for a population of workers that are already under so much stress, instead of shutting down again and paying people to stay home and get these infections under control,” Thompson said.
Thompson worked in the Intensive Care Unit during one of the first surges of COVID-19 and said it immediately made her want to quit. She witnessed one string of deaths after another, with little time to recover after each one.
“It just kept happening. We had to keep working,” she said. “It’s not just caring for patients who have the illness, but also the fear that patients experience when they are separated from family.”
Thompson says that amongst her co-residents, it is the residents of color who have mostly contracted COVID-19. Additionally, Thompson says that most of the hospitalizations she’s seen are Black, Indigenous, and patients of color — and the national numbers reflect that. Black people accounting for 15% of COVID-19 deaths where race is known in the country despite accounting for about 12% of the population. According to the CDC, Black Americans are 2.6 times as likely to be hospitalized for COVID-19 as white, non-Hispanic Americans, and about twice as likely to die from the virus than white, non-Hispanic Americans. As of Jan. 1, Black people account for the highest demographic spike in COVID-19 cases, with 270.5 per 100,000 population.
So far, residents across the country have advocated for hazard pay and higher wages to no avail. A first-year medical resident makes $57,500, and on average they made $64,000 in 2021, according to a Medscape report. Most work a minimum of 80 hours a week, averaging less than $16 an hour. They’ve also argued the government should continue the pause on student loans.
“I wish the government would actually support us health care workers so that we’re better able to support our patients,” says Thompson.
This post was originally published on Latest – Truthout.
-
Flight Attendant union president and labor leader Sara Nelson is criticizing the Centers for Disease Control and Prevention (CDC) for changing its guidance on quarantining for COVID-19 after business leaders asked the agency to cut its recommendations by half, potentially at the cost of public health.
Nelson, the president of the Association of Flight Attendants-CWA International, accused the CDC in a statement of making its decision to benefit businesses that may be experiencing staffing issues, rather than stemming the spread of the virus.
The post Flight Attendant Union Criticizes CDC For Decision “Pushed By Corporate America” appeared first on PopularResistance.Org.
This post was originally published on PopularResistance.Org.
-

A few weeks ago, a ProPublica reporter decided to test his kids for COVID-19. They had the sniffles, and with a grandparent set to visit he wanted to minimize the risk that they were infectious.
This was the problem that quick, cheap COVID-19 tests were supposed to help fix. No need to go to a clinic or wait days for results. Just pick up a pack of tests at a local pharmacy whenever you want, swab your nose and learn within 15 minutes if you’re likely to pass the virus along.
So the ProPublican went to his neighborhood CVS, hoping to buy the required pack of two for $23.99. They were out of stock. Then he went to Rite Aid. They didn’t have the tests either. Then Walgreens, then another CVS. All out of stock. The only supplier with a few tests to offer was his sister, who happened to have a few tucked away.
It’s a familiar experience for many Americans. But not for people in Britain, who get free rapid tests delivered to their homes on demand. Or France, Germany or Belgium, where at-home tests are ubiquitous and as cheap as a decent cappuccino.
So why are at-home tests still so pricey and hard to find in the United States?
The answer appears to be a confounding combination of overzealous regulation and anemic government support — issues that have characterized America’s testing response from the beginning of the pandemic.
Companies trying to get the Food and Drug Administration’s approval for rapid COVID-19 tests describe an arbitrary, opaque process that meanders on, sometimes long after their products have been approved in other countries that prioritize accessibility and affordability over perfect accuracy.
After the FDA put out a call for more rapid tests in the summer of 2020, Los Angeles-based biotech company WHPM, Inc. began working on one. They did a peer-reviewed trial following the agency’s directions, then submitted the results this past March.
In late May, WHPM head of international sales Chris Patterson said, the company got a confusing email from its FDA reviewer asking for information that had in fact already been provided. WHPM responded within two days. Months passed. In September, after a bit more back and forth, the FDA wrote to say it had identified other deficiencies, and wouldn’t review the rest of the application. Even if WHPM fixed the issues, the application would be “deprioritized,” or moved to the back of the line.
“We spent our own million dollars developing this thing, at their encouragement, and then they just treat you like a criminal,” said Patterson. Meanwhile, the WHPM rapid test has been approved in Mexico and the European Union, where the company has received large orders.
An FDA scientist who vetted COVID-19 test applications told ProPublica he became so frustrated by delays that he quit the agency earlier this year. “They’re neither denying the bad ones or approving the good ones,” he said, asking to remain anonymous because his current work requires dealing with the agency.
FDA officials said they simply want to ensure that rapid tests detect even low levels of the virus, since false negative test results could cause people to unwittingly spread the disease. They blame the test shortages on an absence of the kind of sustained public funding that European governments have provided. Without it, manufacturers have lacked confidence that going through the FDA’s process would be financially worth the trouble.
“Where we have seen tests truly coming to the marketplace, the big difference has been government investment,” said Dr. Jeff Shuren, head of the FDA’s Center for Devices and Radiological Health, which authorizes tests. “Folks will come and do larger volumes because you’re supporting production, which can also help drive down prices.”
Both the Trump and Biden administrations banked on vaccines putting a swift end to the pandemic, holding off on large-scale purchases of COVID-19 tests that Americans could keep in their medicine cabinets.
As a result, one of the few companies that has successfully gotten tests authorized and onto shelves — Abbott Laboratories — has dominated the market. Its BinaxNOW tests account for around 75% of U.S. retail sales, according to data from NielsenIQ, even though they’re sold here for several times the price of the same Abbott tests in Europe.
In the past two months, the Biden administration has taken steps to make home tests more widely available. As more tests are authorized and more purchase orders are signed, pharmacy shelves are starting to fill up.
But that still may not be enough, as manufacturers scramble to build supply chains capable of delivering the tens of millions of tests per week that public health experts estimate will be necessary to keep schools and workplaces open and safe. Employers charged with testing their entire workforces have found themselves in bidding wars in order to secure adequate supply.
As with the slow ramp-up of lab testing at the beginning of the pandemic, the delays have come with a cost.
“It feels like in one place we’re in a rocket ship and in another place we’re on training wheels,” said Rep. Kim Schrier, D-Wash., contrasting vaccines and testing. Schrier, a former pediatrician who has been pushing the agency to authorize more rapid tests, said, “You can’t count on the free market during a pandemic.”
The U.S. testing response has been troubled from the beginning of the pandemic, seesawing between caution and overcorrection.
In February 2020, the Centers for Disease Control and Prevention took weeks to develop its own test, which later turned out to have falsely flagged other viruses, allowing the one that causes COVID-19 to gain a foothold in the U.S.
Then the FDA became more permissive, allowing privately developed tests that detected antibodies from previous infections to enter the market after only cursory review. When dozens of the tests turned out to be inaccurate, the FDA prohibited their use.
Meanwhile, the FDA grappled with thousands of applications for “emergency use authorizations,” or EUAs. The process for EUAs is less involved than for full approval but still requires extensive clinical and real-world evaluation. Most EUAs issued have been for PCR tests, which are highly sensitive — meaning they can detect even low levels of the virus — but typically take days to return results.
Another form of diagnostics, antigen tests, can return results quickly and cheaply, similar to a pregnancy test. They’re less sensitive, but usually good enough to determine whether someone is infectious.
Recognizing the potential market for antigen tests, companies began submitting more EUA applications in late 2020. But the FDA was wary about this type of test, mostly warning of the danger of false negatives in the earliest stages of infection.
FDA officials were particularly concerned about allowing tests to be administered outside the purview of a trained health care provider. “To mitigate the impact of false results, all Covid-19 tests authorized to date have been made available only by prescription, so that clinicians can interpret results for patients,” wrote Shuren and his deputy Dr. Tim Stenzel in an October 2020 column in The New England Journal of Medicine.
That cautious approach persisted all through the winter and early spring, despite rising agitation from the White House and Congress around the availability of tests.
“I actually have been saying that for months and months and months, we should be literally flooding the system with easily accessible, cheap, not needing a prescription, point of care, highly sensitive and highly specific” tests, White House chief medical advisor Dr. Anthony Fauci said under questioning from Schrier in a hearing on March 17.
Stenzel, a microbiology Ph.D. who in 2018 became director of the office that authorizes diagnostic tests, holds the most day-to-day power over whether a test gets approved. He worked at biotech companies for most of his career before coming to the FDA, leading some to wonder if those prior relationships played a role in determining which testmakers became the most important players in the market.
Among Stenzel’s former employers were Abbott and the San Diego-based Quidel Corporation, the first two companies to sell self-administered, prescription-free COVID tests in large volumes.
Quidel CEO Doug Bryant said in a promotional video that in early 2020, the company wasn’t planning on designing a COVID-19 test until he got a call from a trusted contact at the FDA. That contact was Stenzel, the agency confirmed.
Quidel and Abbott had their at-home tests approved about a year later. On an earnings call, Quidel’s Bryant said it was “the most significant inflection point for our company.” In the third quarter of 2021, Quidel made $406 million from its various COVID-19 tests, blowing past Wall Street’s expectations. “There is no denying Quidel has put itself in position to win big in COVID-19 testing,” wrote an analyst with the firm William Blair. Abbott made $1.9 billion globally on its COVID-19 tests.
Ethics disclosures show that Stenzel holds no Abbott or Quidel stock, and it’s been several years since he worked at either company. But Stenzel’s ties to the two major test manufacturers and the slow pace of authorizations for other companies’ at-home tests drew a letter from an anti-monopoly think tank, the American Economic Liberties Project, calling for an investigation.
Stenzel denied any improper conduct, and pointed out that his office issued recalls to both Abbott and Quidel for problems with other COVID-19 tests. He also noted that the office designed relatively easy-to-follow templates for new types of COVID-19 tests to help companies that hadn’t dealt with the FDA before.
“We understood that there were a bunch of companies that were new to the FDA, and we provided them an immense amount of support, saying, ‘This is how you do it,’” Stenzel said.
The FDA has said it “engaged with more than 100 test developers” about making diagnostics. The agency declined to provide the names, citing confidentiality concerns.
Quidel acknowledged the administration had reached out, but didn’t comment on its discussions with Stenzel, while Abbott said it had spoken to “many people across multiple areas of government” early in the pandemic.
Most companies don’t have the same familiarity with the people adjudicating their applications.
Nanōmix, a diagnostics designer based in Emeryville, California, developed a rapid test with the help of a federal grant and submitted it to the FDA in February. In early June, an FDA reviewer sent back a list of questions, giving Nanōmix a deadline of 48 hours to respond. The company couldn’t provide answers that quickly, so it was sent to the back of the line.
“We start development on a set of guidance,” said Nanōmix CEO David Ludvigson. “Then they change the guidance after we’re done, and expect us to have conformed to their revised guidance.”
The FDA has been particularly circumspect with more novel approaches to testing, such as an olfactory test that detects the common COVID-19 symptom of loss of smell. The agency’s reviewers deprioritized an application for the scratch-and-sniff card even though it had been proven to stem transmission, said inventor Derek Toomre, a professor at the Yale School of Medicine.
Other companies, big and small, have been tripped up by FDA demands that seem minor in view of the urgency of the situation.
For example, the biopharmaceutical giant Roche told ProPublica that it submitted a home test in early 2021, but it was rejected by the FDA because the trials had been done partly in Europe. The test had comparedfavorably with Abbott’s rapid test, and received European Union approval in June. The company plans to resubmit an application by the end of the year.
A smaller company, which didn’t want to be named because it has other contracts with the U.S. government, withdrew its pre-application for a rapid antigen test with integrated smartphone-based reporting because it heard its trial data from India — collected as the delta variant was surging there — wouldn’t be accepted. Doing the trials in the U.S. would have cost millions.
The FDA reviewer who quit this May described what the delays looked like from the inside. With a background in virology, he could evaluate the hundreds of pages in an application within a few days. But then, something strange happened: The applications would go nowhere for months as higher-up officials seemed paralyzed by indecision.
“I could easily process dozens of them, but I ended up with one or two in my queue constantly. They would stay there forever,” he said. “I had a lot of free time.”
His experience is reflected in an outside review of the EUA process conducted by the consulting firm Booz Allen Hamilton, which found that the median number of days it took the FDA to issue a decision on original applications rose to 99 in November 2020 from 29 the previous April, with denials taking substantially longer than authorizations. The assessment also found “limited understanding in the test developer community on how to appropriately validate a diagnostic test.”
Stenzel said that any delays were a consequence of careful review, and that the office received many applications that were incomplete or had shoddy data.
“If we have questions or concerns about a test, they will not be prioritized the same way a test will be that we have fewer questions about,” Stenzel said. “Those will be cycled to the front, and it makes good public health sense to move forward those tests that are most likely to pass muster and get authorized. … There are always good reasons for why something is delayed.”
European countries generally maintain similar guidelines for the accuracy of tests, but are less particular about how trials must be conducted. For example, test developers are allowed to limit their samples to subjects with high viral loads, for whom antigen tests perform better.
The FDA, however, remains concerned that the typical method for measuring viral load isn’t consistent, leading to the risk of overestimating the accuracy of the test. Advocates of the European approach point out that being able to identify an infection in its earliest stages won’t help much if a PCR result doesn’t come back for days, so even a less sensitive at-home antigen test is valuable — especially since people are much more likely to be able to access them in the first place than PCR tests.
Europe’s differing approach has resulted in 39 rapid self-administered antigen tests being authorized by the European Union, according to a database maintained by Arizona State University. The U.S. has authorized 12, nine of which are available without a prescription.
A consultant who works with smaller companies trying to get products through the FDA — and who asked for anonymity in order to protect his clients who have business before the agency — said he understands the argument that more robust applications from companies with larger manufacturing capacity should go first.
The problem with this logic, he said, is that it’s now fall and the pandemic is ongoing, with the possibility of new variants still unknown. “And it’s not like you can flip a switch with the Defense Production Act and you’re going to get magically much more capacity,” he said. “We needed a ‘thousand flowers bloom’ approach. We needed everyone and their brother pitching in with these tests.”
The federal government could also have buttressed the supply of rapid COVID-19 tests by purchasing large quantities from companies able to manufacture them in bulk, and then providing them to consumers at low or no cost.
Shuren and Stenzel recommended as much a year ago in their New England Journal of Medicine column. They wrote that the U.S. government should have authorized a handful of tests and had the CDC contract with those manufacturers, rather than trying to vet thousands of diagnostics, which they called “an inefficient use of resources.”
European countries essentially did both, authorizing dozens of rapid antigen tests to be sold while contracting with a few companies to provide millions of them free of charge to individuals. The U.K., for example, allocated $50 billion over two years to set up a national test and trace program that delivers rapid tests to anyone upon request. It hasn’t worked perfectly or averted lockdowns, but advocates argue it’s better than the U.S. alternative of rapid tests being nearly impossible to find.
For Germany’s free testing program, which ran from March through October, the government initially bought 800 million rapid tests and 200 million home tests from a shorter list of manufacturers that had undergone additional vetting. The country also required the unvaccinated to present fresh test results for most activities that involve congregating with other people.
Although the U.S. government has spent billions of dollars on testing — estimates of the total vary, given the number of funding streams — self-administered tests are usually not covered by insurance, and there is no centralized system for distributing them.
In the late winter and early spring of 2020-21, the federal government spent hundreds of millions of dollars to buy point-of-care tests, but they were mostly reserved for use in facilities like nursing homes and military bases. The economic stimulus bill that passed in March allocated $10 billion for screening in schools, which don’t usually rely on home tests. Then, the focus shifted to vaccines.
In May, the CDC leaned hard into the message that vaccines were almost completely protective, mitigating the need for frequent testing. Manufacturers took that as a bad sign for testing volume. Abbott ramped down manufacturing of its popular home test.
At that time, Stenzel seemed satisfied with the availability of tests. “We believe we’re doing a great job at meeting the public health need at this point,” he said in June on his weekly town hall call with test developers.
With no long-term government purchasing programs in place, companies had less interest in getting new tests through the pipeline, making it difficult for even promising concepts to get commercial pickup. With the help of a federal grant meant to accelerate COVID-related technologies, Iowa State University professor Nigel Reuel developed a mailable paper test in April, but he said he’s not sure it’ll be worth it to take the step of clinical trials.
It’s really hard, Reuel said, for a company to “say we’re going to invest tons in this when we don’t know what the long-term market for it is.”
All this meant that when the delta variant hit in July, not only were PCR appointments suddenly hard to get, but home tests became vanishingly rare and reliant on a single manufacturer: Abbott, whose BinaxNOW test peaked during late summer at 90% of the market in retail over-the-counter sales. That dipped somewhat in September, when a few additional companies were able to get on shelves.
On an earnings call in October, Abbott CEO Robert Ford said the company anticipated dropping its price to maintain its market share, but wouldn’t if competition didn’t make it necessary.
Asked why its rapid tests are abundant and cheap in Europe and scarce in the U.S., Abbott spokesperson John Koval chalked it up to Europe’s public support, both in its regulatory system and through government funding.
“It has taken more than a year for the American public, scientific experts and academia to accept the important role of rapid testing in the U.S.,” Koval said. “Overseas, that was not the case, because the value of rapid testing was better understood prior to the pandemic.”
Sentiment in Washington has been changing. In late October, Sen. Dick Durbin sent a letter urging “appropriate flexibility in regulatory standards” for at-home tests. And over the past month, the White House has thrown more weight behind rapid testing, announcing $1 billion in purchase commitments for home tests. Recognizing the difficulty of quickly securing the necessary volume of raw materials for tests, the Department of Health and Human Services awarded another $560 million to 13 companies for test components like swabs, pipette tips, packaging and other production capabilities.
Still, some of the government’s efforts haven’t added up to much.
In September, the White House announced that Walmart, Amazon and Kroger would sell COVID-19 tests at cost for the following three months. But no subsidy was involved, and for most of the first two months, the retailers were often out of stock. Tests available online are often sold by third-party distributors, and Amazon and Walmart said they don’t control those prices, so they remain high.
At CVS, which didn’t participate in the agreement with the White House, a Quidel kit — which costs $12 wholesale — still sells for $23.99.
Same with Rite Aid, but when one of us visited a store in Brooklyn this Wednesday, employees said they hadn’t received a shipment of BinaxNOW kits in a month, until they got seven the day before. “They immediately sold out. And that was limiting it to one per person,” said Roxanne, a pharmacy technician who declined to give her last name.
Meanwhile, the U.S. is moving to take on more responsibility over the validation of tests. Last week, the National Institutes of Health announced a new program to do much of the work for test developers, mitigating the back and forth around what’s good enough. That resembles the process run by some European governments, although Shuren said the U.S. will still maintain tougher standards.
All of those steps would have been more helpful when experts began calling for them a year ago.
“We need to have a rethinking, during and after this pandemic, to talk about the role of testing,” said Mara Aspinall, who co-founded the Biomedical Diagnostics program at Arizona State University’s College of Health Solutions. “It’s a fundamental piece of our fight. And that was realized too late.”
Do you have information about COVID-19 testing that we should know? Email lydia.depillis@propublica.org or message her on Signal at 202-913-3717. Email eric.umansky@propublica.org or message him on Signal at 917-687-8406.
This post was originally published on Latest – Truthout.
-

Not all opponents of mask mandates and anti-vaccine activists are alike. They constitute a diverse and heterogeneous group. But a certain segment of the anti-maskers and anti-vaxxers comprise extremists who represent a violent and nefarious influence in our country as we work to defeat this seemingly endless pandemic.
There is a small but loud and forceful group of people who object to wearing masks. Studies indicate that those people generally believe they are ineffective and are violating their civil liberties. Some of those people are increasingly behaving in violent and dangerous ways.
As early as July 2020, the Retail Industry Leaders Association expressed alarm over the number of instances of hostility and violence experienced by front-line employees. That same month, a survey of McDonald’s employees showed that 44% had experienced verbal or physical abuse from customers not wearing masks.
These repeated incidents necessitated the CDC to offer new guidance for retailers and restaurants on how to prevent workplace violence from customers. These suggestions included installing panic buttons and cameras, and recognizing the signs that angry customers might be on the verge of violence.
Things since then have only worsened.
In June 2021, a customer shot and killed a cashier and wounded a sheriff’s deputy at a supermarket after an argument about face masks.
In August 2021, Christopher Key, who calls himself the “vaccine police,” live streamed himself and his “Missouri Crew” entering a Walmart Supercenter. The group was targeting the pharmacists who they believe should be “executed” for administering the COVID-19 vaccine. They berated the workers, informing them they have been put “on notice” and that “if they give one more vaccine … they can be hung up … and executed.”
The group brought with them “sworn affidavits” that supposedly proved that 45,000 people had died within days of being vaccinated against COVID-19. That belief is based on a lawsuit filed by a group called America’s Frontline Doctors (AFLD), recently described in a Time magazine expose as “the 21st-century, digital version of snake-oil salesmen.” AFLD was founded by Dr. Simone Gold, who was arrested for her participation in the U.S. Capitol insurrection on Jan. 6, 2021.
A COVID-19 drive-through testing and vaccination site in Georgia was recently forced to shut down after being threatened by a group of anti-vax protesters. Reports indicated that the health care workers were harassed via email and on social media.
Health care workers have repeatedly faced threats for promoting vaccines, especially prominent public health experts like Dr. Anthony Fauci and Dr. Peter Hotez. Both have faced serious death threats. A man was arrested for allegedly sending threatening messages to Dr. Fauci, saying that he and his family would be “dragged into the street, beaten to death and set on fire.” Dr. Hotez notes that the threats faced by health care workers have created “an unprecedented culture of antiscience intimidation.”
Three men recently ambushed the principal of a school in Arizona. They brought plastic handcuffs, ready to perform a “citizen’s arrest.” They were upset about the “injustice” of the principal asking a child to quarantine because of possible exposure to COVID-19. One of the men, Kelly Walker, a well-known anti-masker, live-streamed the event on his business Instagram page.
That same victimized principal described some of the death threats she has been receiving, including this ominous warning: “Next time it will be a barrel pointed at your Nazi face.”
There is also evidence that extremist groups such as the Proud Boys are behind some of the anti-mask organizing. As some experts have noted, “violence is at the heart” of their ideology.
At a recent school board meeting in Florida, a woman stated that anyone who believes in vaccines or mask mandates in schools is a “demonic entity” and bears “the mark of the beast.” She then warned that “all of us Christians are sticking together to take them all out” adding that “all the police officers that kick us out … will also be going down with them.”
Not all anti-maskers and anti-vaxxers will become violent. But these cases illustrate the propensity of some to threaten and erupt into violence as they attempt to overwhelm others with their positions.
It may be easy to laugh off or dismiss these incidents, but minimizing or denying the potential violence associated with these groups and individuals is a grave mistake. Pretending it does not exist is irresponsible and gives implicit permission for further violence and destruction.
This post was originally published on Latest – Truthout.
-

This post was originally published on Latest – Truthout.
-

Meggan Ingram was fully vaccinated when she tested positive for COVID-19 early this month. The 37-year-old’s fever had spiked to 103 and her breath was coming in ragged bursts when an ambulance rushed her to an emergency room in Pasco, Washington, on Aug. 10. For three hours she was given oxygen and intravenous steroids, but she was ultimately sent home without being admitted.
Seven people in her house have now tested positive. Five were fully vaccinated and two of the children are too young to get a vaccine.
As the pandemic enters a critical new phase, public health authorities continue to lack data on crucial questions, just as they did when COVID-19 first tore through the United States in the spring of 2020. Today there remains no full understanding on how the aggressively contagious delta variant spreads among the nearly 200 million partially or fully vaccinated Americans like Ingram, or on how many are getting sick.
The nation is flying blind yet again, critics say, because on May 1 of this year — as the new variant found a foothold in the U.S. — the Centers for Disease Control and Prevention mostly stopped tracking COVID-19 in vaccinated people, also known as breakthrough cases, unless the illness was severe enough to cause hospitalization or death.
Individual states now set their own criteria for collecting data on breakthrough cases, resulting in a muddled grasp of COVID-19’s impact, leaving experts in the dark as to the true number of infections among the vaccinated, whether or not vaccinated people can develop long-haul illness, and the risks to unvaccinated children as they return to school.
“It’s like saying we don’t count,” said Ingram after learning of the CDC’s policy change. COVID-19 roared through her household, yet it is unlikely any of those cases will show up in federal data because no one died or was admitted to a hospital.
The CDC told ProPublica in an email that it continues to study breakthrough cases, just in a different way. “This shift will help maximize the quality of the data collected on cases of greatest clinical and public health importance,” the email said.
In addition to the hospitalization and death information, the CDC is working with Emerging Infections Program sites in 10 states to study breakthrough cases, including some mild and asymptomatic ones, the agency’s email said.
Under pressure from some health experts, the CDC announced Wednesday that it will create a new outbreak analysis and forecast center, tapping experts in the private sector and public health to guide it to better predict how diseases spread and to act quickly during an outbreak.
Tracking only some data and not releasing it sooner or more fully, critics say, leaves a gaping hole in the nation’s understanding of the disease at a time when it most needs information.
“They are missing a large portion of the infected,” said Dr. Randall Olsen, medical director of molecular diagnostics at Houston Methodist Hospital in Texas. “If you’re limiting yourself to a small subpopulation with only hospitalizations and deaths, you risk a biased viewpoint.”
On Wednesday, the CDC released a trio of reports that found that while the vaccine remained effective at keeping vaccinated people out of the hospital, the overall protection appears to be waning over time, especially against the delta variant.
Among nursing home residents, one of the studies showed vaccine effectiveness dropped from 74.7% in the spring to just 53.1% by midsummer. Similarly, another report found that the overall effectiveness among vaccinated New York adults dropped from 91.7% to just under 80% between May and July.
The new findings prompted the Biden administration to announce on Wednesday that people who got a Moderna or Pfizer vaccine will be offered a booster shot eight months after their second dose. The program is scheduled to begin the week of Sept. 20 but needs approval from the Food and Drug Administration and a CDC advisory committee.
This latest development is seen by some as another example of shifting public health messaging and backpedaling that has accompanied every phase of the pandemic for 19 months through two administrations. A little more than a month ago, the CDC and the FDA released a joint statement saying that those who have been fully vaccinated “do not need a booster shot at this time.”
The vaccine rollout late last year came with cautious optimism. No vaccine is 100% percent effective against transmission, health officials warned, but the three authorized vaccines proved exceedingly effective against the original COVID-19 strain. The CDC reported a breakthrough infection rate of 0.01% for the months between January and the end of April, although it acknowledged it could be an undercount.
As summer neared, the White House signaled it was time for the vaccinated to celebrate and resume their pre-pandemic lives.
Trouble, though, was looming. Outbreaks of a new, highly contagious variant swept India in the spring and soon began to appear in other nations. It was only a matter of time before it struck here, too.
“The world changed,” said Dr. Eric Topol, director of the Scripps Research Translational Institute, “when delta invaded.”
The current crush of U.S. cases — well over 100,000 per day — has hit the unvaccinated by far the hardest, leaving them at greater risk of serious illness or death. The delta variant is considered at least two or three times more infectious than the original strain of the coronavirus. For months much of the focus by health officials and the White House has been on convincing the resistant to get vaccinated, an effort that has so far produced mixed results.
Yet as spring turned to summer, scattered reports surfaced of clusters of vaccinated people testing positive for the coronavirus. In May, eight vaccinated members of the New York Yankees tested positive. In June, 11 employees of a Las Vegas hospital became infected, eight of whom were fully vaccinated. And then 469 people who visited the Provincetown, Massachusetts, area between July 3 and July 17 became infected even though 74% of them were fully vaccinated, according to the CDC’s Morbidity and Mortality Weekly Report.
While the vast majority of those cases were relatively mild, the Massachusetts outbreak contributed to the CDC reversing itself on July 27 and recommending that even vaccinated people wear masks indoors — 11 weeks after it had told them they could jettison the protection.
And as the new CDC data showed, vaccines continue to effectively shield vaccinated people against the worst outcomes. But those who get the virus are, in fact, often miserably sick and may chafe at the notion that their cases are not being fully counted.
“The vaccinated are not as protected as they think,” said Topol, “They are still in jeopardy.”
The CDC tracked all breakthrough cases until the end of April, then abruptly stopped without making a formal announcement. A reference to the policy switch appeared on the agency’s website in May about halfway down the homepage.
“I was shocked,” said Dr. Leana Wen, a physician and visiting professor of health policy and management at George Washington University. “I have yet to hear a coherent explanation of why they stopped tracking this information.”
The CDC said in an emailed statement to ProPublica that it decided to focus on the most serious cases because officials believed more targeted data collection would better inform “response research, decisions, and policy.”
Sen. Edward Markey, D-Mass., became alarmed after the Provincetown outbreak and wrote to CDC director Dr. Rochelle Walensky on July 22, questioning the decision to limit investigation of breakthrough cases. He asked what type of data was being compiled and how it would be shared publicly.
“The American public must be informed of the continued risk posed by COVID-19 and variants, and public health and medical officials, as well as health care providers, must have robust data and information to guide their decisions on public health measures,” the letter said.
Markey asked the agency to respond by Aug. 12. So far the senator has received no reply, and the CDC did not answer ProPublica’s question about it.
When the CDC halted its tracking of all but the most severe cases, local and state health departments were left to make up their own rules.
There is now little consistency from state to state or even county to county on what information is gathered about breakthrough cases, how often it is publicly shared, or if it is shared at all.
“We’ve had a patchwork of information between states since the beginning of the pandemic,” said Jen Kates, senior vice president and director of global health and HIV policy at Kaiser Family Foundation.
She is co-author of a July 30 study that found breakthrough cases across the U.S. remained rare, especially those leading to hospitalization or death. However, the study acknowledged that information was limited because state reporting was spotty. Only half the states provide some data on COVID-19 illnesses in vaccinated people.
“There is no single, public repository for data by state or data on breakthrough infections, since the CDC stopped monitoring them,” the report said.
In Texas, where COVID-19 cases are skyrocketing, a state Health and Human Services Commission spokesperson told ProPublica in an email the state agency was “collecting COVID-19 vaccine breakthrough cases of heightened public health interest that result in hospitalization or fatality only.”
Other breakthrough case information is not tracked by the state, so it is unclear how often breakthroughs occur or how widely cases are spreading among the vaccinated. And while Texas reports breakthrough deaths and hospitalizations to the CDC, the information is not included on the state’s public dashboard.
“We will be making some additions to what we are posting, and these data could be included in the future,” the spokesperson said.
South Carolina, on the other hand, makes public its breakthrough numbers on hospitalizations and deaths. Milder breakthrough cases may be included in the state’s overall COVID-19 numbers but they are not labeled as such, said Jane Kelly, an epidemiologist at the South Carolina Department of Health and Environmental Control.
“We agree with the CDC,” she said, “there’s no need to spend public health resources investigating every asymptomatic or mild infection.”
In Utah, state health officials take a different view. “From the beginning of the pandemic we have been committed to being transparent with our data reporting and … the decision to include breakthrough case data on our website is consistent with that approach,” said Tom Hudachko, director of communications for the Utah Department of Health.
Some county-level officials said they track as many breakthrough cases as possible even if their state and the CDC does not.
For instance, in Clark County, Nevada, home of Las Vegas, the public health website reported that as of last week there were 225 hospitalized breakthrough cases but 4,377 vaccinated people overall who have tested positive for the coronavirus.
That means that less than 5% of reported breakthrough cases resulted in hospitalization. “The Southern Nevada Health District tracks the total number of fully vaccinated individuals who test positive for COVID-19 and it is a method to provide a fuller picture of what is occurring in our community,” said Stephanie Bethel, a spokesperson for the health district in an email.
Sara Schmidt, a 44-year-old elementary school teacher in Alton, Illinois, is another person who has likely fallen through the data hole.
“I thought, ‘COVID is over and I’m going to Disney World,’” she said. She planned a five-day trip for the end of July with her parents. Not only had she been fully vaccinated, receiving her second shot in March, she is also sure she had COVID-19 in the summer of 2020. Back then she had all the symptoms but had a hard time getting tested. When she finally did, the result came back negative, but her doctor told her to assume it was inaccurate.
“My guard was down,” she said. She was less vigilant about wearing a mask in the Florida summer heat, assuming she was protected by the vaccination and her presumed earlier infection.
On the July 29 plane trip home, she felt mildly sick. Within days she was “absolutely miserable.” Her coughing continued to worsen, and each time she coughed her head pounded. On Aug. 1 she tested positive. Her parents were negative.
Now, three weeks later, she is far from fully recovered and classes are about to begin at her school. There’s a school mask mandate, but her students are too young to be vaccinated. “I’m worried I will give it to them, or I will get it for a third time,” she said.
But it is doubtful her case will be tracked because she was never hospitalized. That infuriates her, she said, because it downplays what is happening.
“Everyone has a right to know how many breakthrough cases there are,” she said, “I was under the impression that if I did get a breakthrough case, it would just be sniffles. They make it sound like everything is under control and it’s not.”
This post was originally published on Latest – Truthout.
-

Rep. Alexandria Ocasio-Cortez was among several critics on Friday who warned that the Biden administration’s plan to allow the Centers for Disease Control and Prevention’s eviction moratorium to expire on July 31 would have devastating consequences for millions of renters as well as threatening public health as Covid-19 cases surge.
President Joe Biden extended the moratorium by one month in June but has shown no signs that he plans to do the same this month.
According to U.S. Treasury Department data, dozens of jurisdictions across the country have yet to start distributing assistance funds for renters that were appropriated in March as part of the American Rescue Plan Act.
Millions of Americans on brink of eviction despite billions in aid passed by Congress. More than 80 jurisdictions hadn’t even started their distribution programs by end of May. June distribution increase (85%
 from May) is promising but not fast enough. https://t.co/1b0Dwqvx9y pic.twitter.com/IMn8NQ29ut
from May) is promising but not fast enough. https://t.co/1b0Dwqvx9y pic.twitter.com/IMn8NQ29ut— Emily A. Benfer (@emilyabenfer) July 23, 2021
“It is reckless not to extend the deadline when rental assistance funds have not gone out fast enough to protect people,” said Ocasio-Cortez on Friday. “Eviction filings have already spiked in anticipation of the deadline being lifted.”
According to analysis by the Center on Budget and Policy Priorities released this week, 11.4 million renters — or one in seven — are behind on rent payments. Advocates say about six million are at risk of promptly losing their homes if the eviction moratorium is not extended at the end of July.
According to Paul Williams, a fellow at the Jain Family Institute, about 80% of those six million people “live in counties with rapid, Delta variant-driven [Covid-1] case growth.”
Vast majority of that 6 million are in counties with rapid, Delta variant driven case growth.https://t.co/fCdFCjeDgK
— Paul E Williams (@PEWilliams_) July 23, 2021
Though the Biden administration has not signaled that it plans to extend aid for renters, the White House on Friday announced it will allow homeowners with Fannie Mae and Freddie Mac-backed mortgages to delay their payments until September, a measure that will help 1.8 million people in forbearance.
Diane Yentel, president and CEO of the National Low Income Housing Coalition, called on Biden to provide more assistance to renters as well.
“The CDC eviction moratorium is a necessary public health measure to lessen spread of [and] deaths from Covid-19,” Yentel said. “The need clearly remains as Delta surges.”
This post was originally published on Latest – Truthout.
-

New Centers for Disease Control and Prevention data out Wednesday shows that life expectancy in the U.S. fell by one and a half years in 2020, a decline fueled in large part by the deadly coronavirus pandemic.
“U.S. life expectancy at birth for 2020, based on nearly final data, was 77.3 years, the lowest it has been since 2003,” reads a new report from the CDC’s National Center for Health Statistics. “Mortality due to Covid-19 had, by far, the single greatest effect on the decline in life expectancy at birth between 2019 and 2020, overall.”
The new CDC figures indicate that 2020 saw the steepest single-year decline in life expectancy in the U.S. — from 78.8 years in 2019 to 77.3 last year — since World War II.
“I myself had never seen a change this big except in the history books,” Elizabeth Arias, a CDC demographer and lead author of the new report, told the Wall Street Journal.
U.S. life expectancy dropped by 1.5 years in 2020, the biggest decline since World War II.
Life expectancy decreased an average of 0.22 years in peer countrieshttps://t.co/sCYQBWoh7v pic.twitter.com/18A4Mn0Ajk
— Gabriel Zucman (@gabriel_zucman) July 21, 2021
Given that they are more likely to work jobs with a high risk of coronavirus exposure and lack adequate healthcare, Black and Hispanic people have been disproportionately affected by the pandemic and the resulting fall in life expectancy.
“Between 2019 and 2020, life expectancy decreased by 3 years for the Hispanic population (81.8 to 78.8),” the CDC found. “It decreased by 2.9 years for the non-Hispanic black population (74.7 to 71.8) and by 1.2 years for the non-Hispanic white population (78.8 to 77.6).”
Other factors contributing to the decline in life expectancy last year, according to the CDC, were drug overdoses, homicide, diabetes, and chronic liver disease and cirrhosis.
“It’s horrific,” Anne Case, a professor emeritus of economics and public affairs at Princeton University, told the Washington Post. “It’s not entirely unexpected given what we have already seen about mortality rates as the year went on, but that still doesn’t stop it from being just horrific, especially for non-Hispanic Blacks and for Hispanics.”
This post was originally published on Latest – Truthout.
-
How do you make a potentially dangerous and ineffective drug appear like a miracle of modern science? You could, for instance, enrol only certain people in clinical trials and exclude others or bring the study to a close as soon as you see a spike in the data that implies evidence of effectiveness.
There are many ways to do it.
According to health practitioner and writer Craig Stellpflug in his article ‘Big Pharma: Getting away with murder’ (2012), the strategy is to get in quick, design the study to get the result you want, get out fast and make lots of money.
Stellpflug says:
If a study comes up negative for your favorite drug, just don’t publish it! 68 per cent of all drug studies are swept under the carpet to keep those pesky side effects from being reported. Only 32 per cent of studies come up positive and a lot of those studies are ‘shortened’ to limit the long-term findings. Studies cut short were found to overestimate the study drug’s effectiveness and miss dangerous side effects and complications by an average of 30 per cent. This would explain the amazing 85 per cent drug study success rate in the hands of Big Pharma according to the Annals of Internal Medicine.
Of course, it helps to get the regulatory agencies on board and to convince the media and health officials of the need for your wonder product and its efficacy and safety. In the process, well-paid career scientists and ‘science’ effectively become shaped and led by corporate profit margins and political processes.
And what better way to make a financial killing than by making a mountain out of a molehill and calling it a ‘pandemic’?
COVID-19 vaccine concerns
The Wall Street Journal recently published an article by two health professors who said politics — not science — is behind the failure of health officials and the media to fully inform the public about the potential risks associated with COVID vaccines.
Although the article is available in full to subscribers only, the Children’s Health Defense (CHD) website provides an informative summary.
The CHD notes that Dr Joseph A Ladapo, associate professor of medicine at the David Geffen School of Medicine, and Dr Harvey A Risch, professor of epidemiology at Yale School of Public Health, wrote that while prominent scientists have raised concerns that the safety risks of Covid-19 vaccines have been underestimated, the politics of vaccination has relegated their concerns to the outskirts of scientific thinking.
The two professors noted that clinical studies do not always tell the full story about the safety of medications and that the health effects often remain unknown until the medicine is rolled out to the general public. Examples include Vioxx, a pain reliever that increased the risk of heart attack and stroke; antidepressants that appeared to increase suicide attempts among young adults; and an influenza vaccine used in the 2009-10 swine flu epidemic that was suspected of causing febrile convulsions and narcolepsy in children.
The authors added that clinical trials often enroll patients who are not representative of the general population and more is learnt about drug safety from real-world evidence. With this in mind, they said the large clustering of side effects following COVID vaccines is concerning as is the silence around these potential signals of harm.
Serious adverse events reported by the Vaccine Adverse Event Reporting System include low platelets, heart inflammation, deep-vein thrombosis and death. However, the two scientists argue this is likely to be a fraction of the total number of adverse events.
They criticise the Centers for Disease Control and Prevention (CDC) and the US Food and Drug Administration (FDA) for ignoring the reported serious COVID vaccine side effects.
The authors acknowledge the risks of COVID vaccines in certain populations, not least children, may outweigh the benefits. They also state that not a single published study has demonstrated that patients with a prior infection benefit from COVID-19 vaccination. Something which is not readily acknowledged by the CDC or Anthony Fauci, an indication, according to the authors, of how deeply entangled pandemic politics is in science.
They conclude that public health authorities are making a mistake and risking public erosion of trust by not being forthcoming about the possibility of harm from the vaccines.
Merck and Vioxx
It is revealing that the two scientists refer to Vioxx, which was once popular for treating the symptoms of arthritis. It was removed from the market in 2004 after concerns that it may have injured hundreds of thousands of patients, while possibly killing tens of thousands in the US.
Dr David Graham, whistleblower and senior FDA investigator, criticised the FDA’s approval process of Vioxx (rofecoxib), an anti-inflammatory drug administered orally. In various interviews and congressional hearings, he described the outcome of Vioxx as disastrous and unparalleled in the history of the US. He added that the saga surrounding Vioxx had constituted an unprecedented failure of the nation’s system of drug approval and oversight.
In 2004, Graham argued that the painkiller had caused 88,000 to 139,000 heart attacks in the US – 30-40 per cent of which were fatal – over the previous five years. Nevertheless, manufactured by Monsanto (a company with a proven track record of corrupt practices) and co-marketed by Merck, Vioxx became a leading drug in providing pain relief from the symptoms of various forms of arthritis.
Research presented to the FDA in early 2001 showed that patients taking Vioxx had a higher risk of heart attack compared to those taking some of the older alternatives.
However, the real game-changer came in 2004 when Dr Graham released the findings that found Vioxx increased the chance of heart attack and death from cardiac arrest significantly more than its biggest rival on the market. Dosages of Vioxx in excess of the recommended daily dose of 25 milligrams were also found to more than triple a patient’s risk compared to those who had not taken painkillers.
In September 2004, Vioxx was pulled from the market. But in 2006, more damning findings were revealed by a study that showed that some patients had likely suffered from a heart attack much sooner after starting treatment with Vioxx. Appearing in the Canadian Medical Association Journal, the study showed that 25 per cent of the patients who had heart attacks while taking Vioxx did so within two weeks of starting the drug. This indicated that Vioxx-related cardiovascular risks may occur much earlier than previously thought.
The FDA was criticised for its close relationship with Merck and witnesses at a senate finance committee hearing described how danger signals of Vioxx went ignored. Indeed, a 2007 article published by the National Institutes of Health alleged that even though scientists at Merck knew that the drug might adversely affect the cardiovascular system, none of the intervention studies submitted to the FDA in 1998 were designed to evaluate such risk.
Robber barons and guinea pigs
Merck reported over $11 billion in Vioxx sales during the five years the drug was on the market. To date, the company has paid nearly $6 billion in litigation settlements and criminal fines over Vioxx. Still, in hard-nosed commercial terms, it was a massive success, resulting in a $5 billion gain for the company.
In May 2021, it was reported that Covid-19 vaccines had created at least nine new billionaires. According to research by the People’s Vaccine Alliance, the new billionaires included Moderna CEO Stéphane Bancel and Ugur Sahin, the CEO of BioNTech, which has produced a vaccine with Pfizer. Both CEOs were then worth around $4 billion. Senior executives from China’s CanSino Biologics and early investors in Moderna have also become billionaires.
Although the nine new billionaires are worth a combined $19.3 billion, the vaccines were largely funded by public money. For instance, according to a May 2021 report by CNN, BioNTech received €325 million from the German government for the development of the vaccine. The company made a net profit of €1.1 billion in the first three months of the year, largely thanks to its share of sales from the Covid-19 vaccine, compared with a loss of €53.4 million for the same period last year.
Moderna’s Covid-19 vaccine sales reached $1.7 billion in the first three months of this year and it had its first profitable quarter ever. Moderna is expected to make $13.2 billion in Covid-19 vaccine revenue in 2021. The company received billions of dollars in funding from the US government for development of its vaccine.
Big Pharma has every reason to perpetuate the notion of a deadly global pandemic and to inflate the efficacy of and need for its vaccines. And it, along with its associates in government and at the WHO, has every reason to discredit alternative and arguably more effective treatments like Ivermectin (see the online article ‘The Campaign against Ivermectin: WHO’s Chief Scientist Served with Legal Notice for Disinformation and Suppression of Evidence‘).
There is no need to cover ground here that has been covered extensively elsewhere but it is now abundantly clear that many continue to question the overall official COVID-19 narrative, the fear propaganda, the specific data, the PCR testing protocols, the apparent conflicts of interest and vaccine efficacy.
Moreover, a group of 57 leading scientists, doctors and policy experts recently released a report calling in to question the safety and efficacy of the current Covid-19 vaccines. They are calling for an immediate end to all vaccine programmes.
There are hundreds of scientists who have questioned government and WHO strategy and who have brought attention to the extremely low risks posed by COVID to the bulk of the population as well as the destructive (ineffective) policies and decisions pertaining to lockdowns and other restrictions.
There are many other top scientists who are questioning the need for mass vaccination and who have also pointed out credible and extremely disturbing side effects (real and potential) of such a strategy, not least Dr Robert Malone, credited with developing mRNA vaccine technology, Dr Byram Bridle, a viral immunologist, and Dr Geert Vanden Bossche, a prominent virologist and vaccine expert.
Unlike Merck and Vioxx, it will be governments (the public) that foot any future indemnity costs of these experimental vaccines that have escaped proper (long-term) testing. And given the scale of the rollout, the damage caused could make the adverse effects of Vioxx seem a mere blip.
Vaccines that were brought to market via emergency authorisation use for an ‘emergency’ constructed on the basis of deaths so often wrongly attributed to COVID-19. Brought to market on the basis of flawed PCR test protocols with magnification cycles primed to create a ‘casedemic’.
To borrow from Dr David Graham: are we currently witnessing something more disastrous and unparalleled in the history of the world, let alone the US: an unprecedented failure of global drug approval and oversight?
In the meantime, while billions of vaccinated people serve as human guinea pigs, the newly crowned vaccine kings will make hay while the sun shines (and the fear continues).
The post Vaccine Billionaires and Human Guinea Pigs first appeared on Dissident Voice.This post was originally published on Dissident Voice.
-

The Centers for Disease Control and Prevention (CDC) announced on Thursday that it would be extending a moratorium on evictions until July 31. This will be the last time the CDC extends the moratorium, the Biden administration said.
The moratorium was originally scheduled to end at the end of this month on June 30. Over 6 million Americans are behind on rent payments, according to recent Census Bureau data, meaning that many are likely to face the possibility of eviction when the moratorium is lifted. The Biden administration is hoping that the extension will help to stymie a potential crisis, officials said, but emphasized that the postponement will last only “one final month.”
The goal, a senior administration official told reporters, per Politico, is to use “these 30 days to do everything possible to mitigate harmful evictions and prevent a flood of evictions when the moratorium ends.”
The administration also announced several other initiatives on Thursday meant to help mitigate a flood of evictions. Officials issued new guidance for state and local governments to use $47 billion in emergency rental assistance from Congress and the Associate Attorney General Vanita Gupta released a letter urging courts to actively explore alternatives to evictions.
Gupta in her letter warned that “eviction filings are expected to overwhelm courts across the country.” However, the federal guidance for governments and courts is not binding, and experts fear evictions will skyrocket despite these words of caution.
A group of House Democrats sent a letter to Joe Biden and CDC director Rochelle Walensky Tuesday asking the president and CDC to “extend and strengthen” the eviction moratorium.
“Without further action, in just eight days, the CDC moratorium will expire, and millions of renters will once again face the threat of eviction,” the letter signed by over 50 Democrats, including members of the progressive “squad,” read. “Evictions take lives and push households deeper into poverty, impacting everything from health outcomes to educational attainment.”
The Democrats also point out in their letter that eviction doesn’t threaten everyone equally. “The eviction crisis is a racial justice issue,” they write, pointing to data that shows that nonwhite households are more likely to report being behind on rent payments than their white counterparts. They did not specify the length of time they wanted the moratorium to be extended.
Rep. Ayanna Pressley (D-Massachusetts), who spearheaded the Democrats’ letter, thanked Biden for the extension on Twitter on Thursday night. “Thank you to [Biden] and [Walensky] for heeding our calls to extend the eviction moratorium. This pandemic isn’t over and housing is a human right.”
But housing advocates are skeptical that delaying the lifting of the moratorium for only one month would be effective. “We’re simply going to have a horrific crisis in August instead of July,” Diane Yentel, CEO of the National Low Income Housing Coalition, told Politico. Thirty days, Yentel pointed out, may not be enough time to distribute enough resources to the millions of renters in need.
Indeed, though the Biden administration is saying that this is the last time the moratorium will be extended, Rep. Cori Bush (D-Missouri) said on Twitter that it should be extended again. “We have urgent work to do over the next month to secure real rent relief for the millions of people still facing eviction and to further extend and strengthen the moratorium,” she wrote on Thursday evening.
State and local governments have also launched initiatives to help prevent an “eviction cliff.” California officials recently announced that they would be using $5.2 billion from federal pandemic aid to help renters pay off their past-due rent payments. The state’s eviction moratorium was set to expire at the end of the month, however, which likely wouldn’t have been enough time to help many renters secure relief. Additionally, the relief will only help a small portion of renters, pointed out Dean Preston, tenant attorney and progressive district supervisor in San Francisco.
Meanwhile, the eviction crisis overlaps with urgent public health concerns: Princeton’s Eviction Lab recently found that, in cities across the country, the neighborhoods with the most eviction filings are also the neighborhoods with the lowest vaccination rates, due partially to vaccine equity issues.
“The CDC eviction moratorium is, for many tenants behind on rent, the last remaining protection from the threat of displacement,” wrote the Eviction Lab. “As its expiration nears, few protections stand in the way of a family losing their home, and potentially contracting a life-threatening virus.”
This post was originally published on Latest – Truthout.
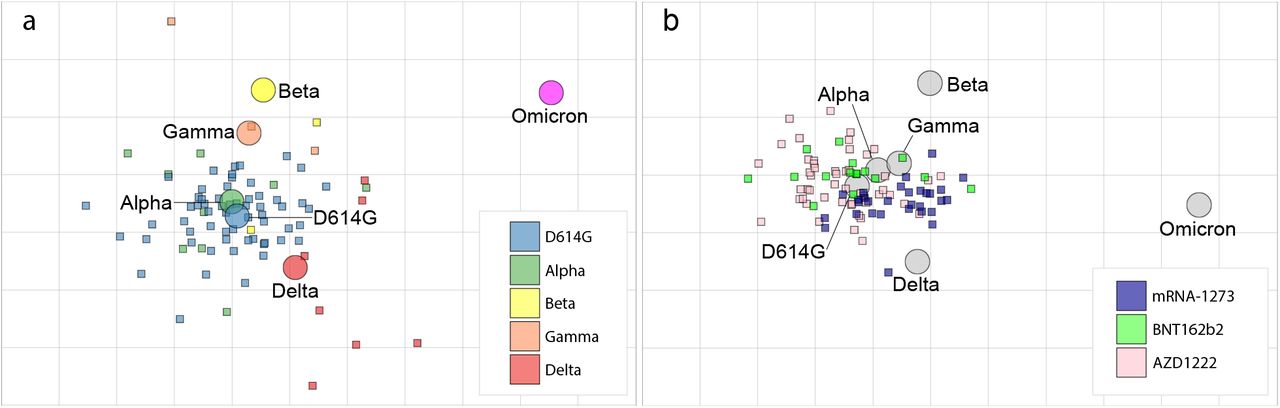{kind=link}
{kind=link}