This past June, Ashley Voss-Barnes received a court summons in the mail. PrairieStar Health Center, a nonprofit community health center in south-central Kansas, was suing her for $675 and her wife for $732 in unpaid medical bills. Voss-Barnes knew the clinic received federal funding to make preventive health care accessible in a region where many families, including her own…
With a decidedly anti-choice Trump administration taking office at its start, 2025 was poised to be yet another brutal year for abortion rights. Advocates feared the imminent resurgence of the Comstock Act, an 1873 law that made it a criminal offense to share contraceptives, abortifacients, and information about either across state lines or through the mail. As of now, the last month of this…
Defenders of reproductive rights on Tuesday responded with alarm after President Donald Trump’s administration quietly imposed an abortion ban at the US Department of Veterans Affairs following a legal opinion penned by a deputy assistant attorney general. After the 2022 Roe v. Wade reversal, the Biden administration allowed the VA to provide abortion counseling and care for service members…
Dr. Thomas C. Weiner, the oncologist who was the subject of a 2024 ProPublica investigation, will never again practice medicine in the state of Montana.
Last week, medical board members revoked Weiner’s license, citing seven cases of malpractice. The board concluded that he had violated rules of professional conduct and provided substandard care. By law, it must report Weiner to a federal database that tracks doctors who’ve been disciplined — which will make it extremely difficult for him to practice medicine.
That decision comes more than a year after ProPublica exposed how, for years, Weiner had been suspected of hurting patients, including some who died, at St. Peter’s Health, the only major hospital serving the state capital of Helena. The story, built on court and medical records, showed Weiner subjected patients who didn’t have cancer to chemotherapy and other dangerous treatments, neglected to properly treat patients who were seriously ill, overprescribed addictive narcotics and was suspected by colleagues to have hastened the deaths of more than a half dozen people.
Weiner, 62, has denied mistreating patients. He did not respond to a request for comment about the board’s decision to revoke his license. St. Peter’s Health, which fired him in 2020, accusing him of malpractice, did not provide comment. The hospital has previously attributed the mistreatment of patients to a rogue doctor and says it provides high-quality care.
Weiner sued St. Peter’s for wrongful termination, a case the hospital ultimately won. Weiner also filed a defamation claim against Dr. Randy Sasich, a former St. Peter’s colleague who lodged complaints about his care. Sasich remains a defendant in that lawsuit.
Before his termination, Weiner was the highest paid doctor at St. Peter’s. Over the years, he made tens of millions of dollars and wielded his influence in the community to drive out hospital leaders who questioned his judgment. Colleagues feared him, and few challenged him. His firing prompted a public outcry, led by his nursing staff and former patients, many of whom continue to support him in a “We stand with Dr. Tom Weiner” Facebook group and on billboards expressing their support.
The ProPublica investigation identified scores of problematic cases. The medical board, though, focused on just seven. Among them was the case of Scot Warwick, whose death and subsequent autopsy was the catalyst for Weiner’s downfall.
As ProPublica reported, Weiner diagnosed Warwick in 2009 with Stage 4 lung cancer, a disease that kills most people in months. For the next 11 years, Weiner subjected his patient to round after round of debilitating therapies including chemo. In 2020, he started to decline rapidly, gaining the notice of Sasich, who couldn’t make sense of his original diagnosis and improbable survival span. But before Sasich could find answers, Warwick died an agonizing death. His widow, Lisa Warwick, ordered an autopsy. It came back negative for cancer — a finding Weiner has repeatedly dismissed — and concluded he likely died from the chemotherapy that Weiner had ordered.
Medical board members confirmed the autopsy’s findings. In its written order, the board concluded that Warwick died “due to gemcitabine-associated pulmonary toxicity.” In other words, the chemotherapy killed him.
The board noted that “Weiner disagrees with this finding and does not admit to it.”
In response to the board’s decision, Lisa Warwick said, “It’s definitely welcomed news — very happy to hear it — but with the caveat that this whole thing took way too long.” For five years, a board that’s supposed to protect patients, she added, “blatantly turned a blind eye.”
Lisa Warwick and her children, Peyton, left, and Brady, stand next to a collage of photographs of their late father, Scot.Louise Johns, special to ProPublica
According to a hospital spokesperson, after St. Peter’s fired Weiner in 2020, it provided the medical board with thousands of pages of documents detailing its allegations, including that Weiner took over complete control of his patients’ care, which made it difficult for other doctors to see or question his treatment. Those documents, many later obtained by ProPublica, languished for years without review by the board, a mystery its spokespeople have declined to explain.
The board renewed Weiner’s license in 2021 and 2023. After ProPublica’s investigation publicly revealed the hospital’s allegations against Weiner, the board renewed his license for a third time this year.
Weiner’s troubles extend beyond losing his license. Last year, the U.S. Department of Justice sued him, accusing him of prescribing needless treatments, double billing, seeing patients more frequently than necessary and “upcoding” — billing for more expensive treatments than he delivered. Weiner has denied the charges. For its part, St. Peter’s already agreed to a $10.8 million settlement for numerous violations of the False Claims Act related to Weiner’s billing of federal insurance programs.
Separately, the parents of a deceased 16-year-old girl whose case was prominently featured in the ProPublica investigation have filed a wrongful death lawsuit against Weiner, the hospital and other staff, accusing them of substandard care and fraud, which is ongoing. In a lengthy interview with ProPublica, Weiner denied that his treatment led to her death.
A criminal investigation is also underway, led by the Montana Department of Justice with help from federal investigators, according to several people who’ve been interviewed by law enforcement. That office did not respond to a request for comment. Weiner has not provided comment on the ongoing criminal investigation.
Weiner sold his home in Helena this year, leaving behind a city deeply divided over his legacy and many people who still believe he was a world-class doctor who has been unfairly targeted by the hospital and the media.
Anthony Olson, a former patient whom Weiner prescribed nine years of chemotherapy for a cancer that never existed, was among that group of supporters until doctors at St. Peter’s helped him accept what had happened to him. His body is still recovering from being poisoned for so long. He has thought about joining the Weiner Facebook group to share his story. But, he said: “I assume there is nothing I can say to them that will bring them around to reason. I’m just glad that no one else is going to be injured.”
In August, I traveled to Kakuma, Kenya, to try to understand what happened when the U.S. cut off food to the world’s third-largest refugee camp.
Soon after President Donald Trump froze foreign aid on his first day in office, my colleague Brett Murphy and I began hearing from government experts. We learned that despite explicit promises from Secretary of State Marco Rubio that food and other life-saving care would continue during the administration’s review of foreign aid, programs were shutting down, putting millions of lives at risk. I’ve covered health in the U.S. and abroad for 15 years, and Brett has covered both the State Department and public health in the U.S. Brett and I teamed up, interviewing dozens of government officials and aid workers, and pouring over reams of internal government documents. Then, we traveled to Kakuma (and South Sudan) to see for ourselves how these policies were affecting people.
In an investigation we published last week, we wrote about how food rations were slashed throughout the camp of more than 308,000 people. We learned first-hand how the Trump administration’s decision to withhold funding for the World Food Program’s operations in Kenya led children to starve and forced thousands of families to make impossible decisions. One of the groups hit hardest by the cuts was pregnant women.
We arrived on a hot, dry day in August with Kenyan photographer Brian Otieno and went straight to the camp’s only hospital, which is run by the International Rescue Committee. The only physician working the hospital’s wards at the time, Dr. Kefa Otieno (no relation to the photographer), gave us a tour.
Dr. Kefa Otieno, right, was the only physician working at the hospital in Kakuma through much of August.Otieno tends to an infant in the maternity ward.
As we entered the maternity unit, a large yellow room with around 45 beds, the majority of them occupied, the doctor explained that the aid cuts were causing an epidemic of life-threatening pregnancy complications. Starving women were giving birth to premature babies. Even those who made it to term were often dangerously underweight. The hospital was understaffed, and people in the camp were so anemic that they couldn’t get enough blood donations. Otieno had twice donated himself while he was midsurgery in order to save a pregnant woman’s life.
Two women embrace in front of the maternity unit.Otieno performs a cesarean section.
Off one side of the maternity ward was a small, stark room with a bench along one wall and two wheeled, metal beds. Otieno called it the kangaroo room. Inside were moms and premature babies too small to safely return home. The hospital had no functional incubators, so medical staff ascribe to a method called kangaroo mother care, where moms hold their babies against their skin to keep them warm and help them grow.
Otieno speaks to a patient.
There, we met Monica and her baby Mary, and Binti and her son Nuru. Both women had difficult pregnancies that the medical staff ascribed to malnourishment. Both had given birth prematurely to underweight babies. And when we visited, both had been trapped in the room for weeks, desperately trying to help their babies gain weight.
Monica feeds Mary.Monica and her husband, Ramazani. They met at church, when she was singing in the choir.
Monica, 21, is funny, with a dry, sharp wit. She met her husband Ramazani at church, when she was singing in the choir. They’d dated for a couple of years before she found out she was pregnant in December last year. They were both scared and excited to be parents, but the timing of the pregnancy was unlucky: As Monica’s belly grew, food rations shrank.
Monica began struggling with anemia and high blood pressure. Otieno told me the roots of these complications were undernourishment.
Monica doesn’t remember going into labor. Ramazani found her collapsed on the floor when he returned from one of the camp’s community showers. She was having seizures, and it took a few hours before they got her to the hospital. Medical staff rushed her in for an emergency cesarean section; she was in such dire shape that staff thought they were going to lose both Monica and her baby. When we met three weeks later, Monica still struggled to speak, her tongue contorted and swollen from biting on it for so long during the seizures.
Still, she was able to tell me about her pregnancy, including a time when she was about five months along and hadn’t eaten for two days. She went to a nearby vendor to beg for a samosa on loan, promising to pay him back later in the day. She then hid in her house for several days, pretending no one was home when he came by to collect the few cents she owed. (Ramazani eventually paid him back.)
At age 28, Nuru was Binti’s thirdchild. She’d had no complications with her previous pregnancies, but with Nuru, she barely gained weight. Binti had come to Kakuma in 2016 after fleeing violence in the Democratic Republic of Congo. When she first arrived at the camp, there was always food.
Binti and her son, Nuru. The child, her third, barely gained weight.
“I had other kinds of stress, but never with food,” she said one afternoon while sitting on the floor sewing curtains for the sparse hospital room.
But during this pregnancy, she said, food was all she thought about. She was so anemic and hungry that she resorted to eating clay, digging out the top layer of earth to get to the cleaner soil below, and charcoal. Her chart showed she gained fewer than 10 pounds during her entire pregnancy. Her baby, Nuru, was born at 33 weeks, weighing about 3.5 pounds.
Otieno wanted the babies to weigh 4 pounds before they went home, enough that they’d have a fighting chance against infection. Hospital staff put the babies on a scale every two days, and before each weigh in, Binti would get herself hyped up: “I can feel it, today is the day we are going home,” she said one afternoon. Monica tried not to think about what the scale would say. Both she and Mary had dropped weight in the preceding weeks. After so much loss, she didn’t want to get her hopes up.
Monica feeds Mary.Anna Maria Barry-Jester
But, while Binti and Monica were desperate to get out of the hospital and home to their families — Binti to her other children and Monica to her two younger siblings — leaving would come at a cost. If and when they went, they’d be cut off from food again.
At the hospital, staff brought around three simple meals every day, typically lentils and rice or sorghum porridge. Outside the hospital, they’d have almost nothing.
Facing dwindling supplies, WFP, which provides food for the camp, made the dramatic decision to only give rations to about half the camp’s residents in August. Families were placed into groups based on rough estimates of need. Even though Monica and Binti were stuck in the hospital precisely because they didn’t have enough to eat, Binti and Ramazani had both been placed in categories that meant they would get no food. Monica and her younger siblings were set to receive just 420 calories a day each.
Women receive porridge for breakfast at the maternity unit.Refugees line up at a World Food Program distribution point in Kakuma in August.
In the meantime, Binti and Monica bonded: They told stories and held one another’s babies while they showered or went to the bathroom. They took turns sleeping on the bench so the babies could have one of the beds. Monica and Ramazani, who spent almost every night at the hospital, made sure that a tiny copy of the Bible was always placed next to baby Mary’s head.
Monica places a Bible next to Mary.
One Saturday morning, Otieno came in to weigh the babies. Binti bounced back and forth on her feet like a boxer preparing for a bout. Nuru weighed in at just under 4 pounds. Binti raised her arms in victory: They could go home.
Binti holds Nuru after Otieno weighs her.
Then it was baby Mary’s turn. “This baby is refusing to gain weight,” Otieno mumbled, trying to still her wiggly legs to get an accurate measurement. Mary had gained 10 grams, equivalent to two-thirds of a tablespoon of water. After days of losing weight, it was perhaps a small victory, but not one that Monica would celebrate. She picked up Mary, held her against her chest, and sat back down on the bench.
I asked Monica about her hopes for the future. She said all she wanted was to be resettled in the U.S. with her siblings and Mary, so they could all go to school and have enough to eat. “Fill your notebook with that,” she said. “It’s the only thing I want.”
Monica and Otieno weigh Mary.
At the end of September, the administration gave WFP’s Kenya operations $66 million, 40% less than the U.S. gave in 2024 and nine months into the year. WFP has said the funds will be enough to provide food to the camp through March, though rations are still far below what humanitarians consider the daily minimum of calories.
In response to a series of questions, a senior State Department official told us that the U.S. still gives WFP hundreds of millions a year and the administration is shifting to investments that will better serve both the U.S. and key allies like Kenya over time.
The official also said that the Office of Management and Budget, not the State Department, has ultimate authority to approve new foreign aid money. When we asked OMB about the delays, communications director Rachel Cauley told us: “That’s absolutely false. And that’s not even how this process works.” She did not clarify what was false.
A new book edited by Kyle Ferrana, China Changes Everything, bills itself as an anthology by “social justice activists, journalists, and commentators” and brings together chapters about the People’s Republic of China written by prominent left-wing analysts, including Arnold August, Roger Harris, Radhika Desai, Carlos Martinez, Gerald Horne, Lee Siu Hin, Margaret Kimberley, Danny Haiphong, KJ Noh, Sara Flounders, and many more.
The publication covers a comprehensive range of subjects in the ongoing “China debate” and includes chapters on such hot topics as China’s relation to Palestine and China’s foreign affairs policies, its banking and healthcare system, its transportation infrastructure and the rail and air infrastructure that China has helped to build in developing nations, its achievements in green technology and poverty alleviation, China’s military expenditures and aims, its role in the “space race,” its alleged genocide of the Uyghurs, and the status of Taiwan and Tibet, among others.
It’s a fundamental tenet of health care in America: Generic drugs are just as safe and effective as brand-name ones. The only difference is the price.
“The same high quality, strength, purity and stability,” the Food and Drug Administration assured the public years ago as factories started to flood the market with their own, cheaper versions of commonly used drugs, from antibiotics to cancer treatments.
But the agency stakes that promise on a risky gamble.
It doesn’t routinely test generics for quality concerns or to see if they’re working as effectively as brand-name medications. Instead, the agency heavily relies on drug companies, often in countries as far away as India and China, to do their own testing and to report any problems.
In recent years, independent labs, universities and the Department of Defense have raised alarms about contaminants and other quality failures in a number of generic medications. So have doctors, who in some cases have gone on to create their own ad hoc lists of drugs they trust and those they learned to avoid.
Yet the FDA largely dismissed the warnings and has only sporadically tested a sampling of generic drugs, which now account for about 90% of prescriptions in the United States. That means the government can’t always say which ones may be compromised or how often that happens. And patients can’t make informed choices about which drugmakers to depend on.
“This ridiculous, small sample of testing that FDA does just cannot stand,” said Albinus D’Sa, a chemist who spent more than 25 years in drug safety at the FDA before retiring in 2023. “It’s not in the public interest.”
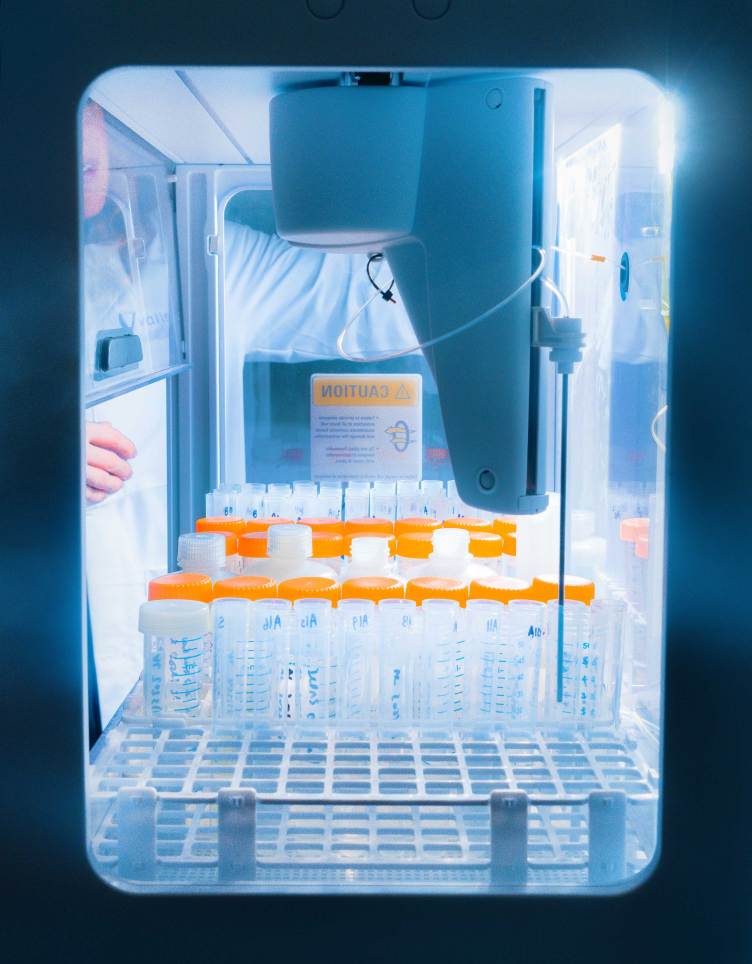
ProPublica decided to test several generic versions of three of the most widely prescribed drugs in the United States: the antidepressant bupropion XL, the generic for Wellbutrin XL; the heart medicine metoprolol succinate, the generic for Toprol XL; and the cholesterol drug atorvastatin, the generic for Lipitor. A total of 11 samples from readers, ProPublica employees and the independent testing lab Valisure were assessed, representing a cross section of manufacturers from around the world.
Some were analyzed for impurities such as lead or whether their dosage levels matched the claims on their labels. Another test scrutinized the speed at which the tablets dissolved — a critical indicator of how medication is released in the body — and compared the results to the brand-name drugs.
While most of the samples passed, the findings showed that one version of bupropion and one version of metoprolol, dispensed at least tens of thousands of times in 2024 alone, had irregularities that experts say could compromise their effectiveness.
As part of ProPublica’s testing at the Connecticut-based lab Valisure, a scientist dropped samples of generic drugs into a solution to see how quickly they dissolved.Tonje Thielesen for ProPublica
The tablets dissolved slower than their brand-name counterparts, which could leave patients without the right therapeutic levels for treatment and no way of knowing if their medication might be at fault.
Metoprolol is a beta blocker used by about 15 million people for conditions like chest pain, heart failure and high blood pressure. Bupropion is a go-to drug for the treatment of depression, prescribed to about six million people in the U.S. each year.
Oregon psychiatrist Dr. James Hancey said receiving incorrect amounts of bupropion throughout the day is a serious quality threat that puts vulnerable patients at risk.
“One of the great potential dangers here is that people become discouraged and disillusioned,” he said when told about ProPublica’s findings.
Hancey said he worries that patients taking ineffective antidepressants can feel hopeless, increasing suicide risk. “Sort of like, ‘I must really be messed up. … I’ll never get any better,’” he said. “You can only lose so much hope.”
Irregular levels of metoprolol can also pose a danger, especially for people with congestive heart failure or a history of heart attacks, said Dr. Art Kellermann, a longtime member of the National Academy of Medicine and former senior vice president for health sciences at Virginia Commonwealth University.
“You may never get to the level your body needs to be safe,” he said.
A scientist preps samples of the antidepressant bupropion XL for ProPublica’s testing. Tonje Thielesen for ProPublica
Dozens of companies received approval from the FDA over the years to sell metoprolol and bupropion in the U.S. Yet from 2018 to 2024, the agency reported running only 2 tests on metoprolol and 7 on bupropion through its quality surveillance program — in each case, by pulling a sample from a single drugmaker. In many of those years, the drugs weren’t tested at all, FDA records show. Those that were assessed received passing results.
The FDA did not respond to questions about why the agency didn’t do more testing and how it can know that generics are safe without a more robust program. On its website, the FDA said it has relied on a “more targeted, risk-based” approach to testing since 2018, choosing samples of drugs that have safety, effectiveness or quality concerns. The agency publicly reports the results on its website and notes that a majority of the tested drugs meet its standards.
ProPublica, however, found the agency for years failed to routinely test not only the generics that have worried outside experts but also drugs coming from factories that amassed so many serious quality and safety violations they were ultimately banned from the U.S. market.
In 2023, the FDA barred two Intas Pharmaceuticals factories in India from shipping drugs to the U.S., in part because workers had manipulated drug-testing records to cover up bad results, government records show. An “egregious pattern,” regulators wrote in a letter to the company.
ProPublica’s testing, however, found the factory’s bupropion dissolved more slowly than the brand-name drug as well as versions of the medication made by other generic manufacturers.
Intas, whose U.S. subsidiary is Accord Healthcare, said in a statement that its bupropion is safe, effective and equivalent to the brand-name medication, and that the company has made improvements since the FDA’s inspections, including bringing in third-party experts focused on quality and data integrity. The company added it is no longer manufacturing bupropion for the U.S.
In recent years, the FDA’s own records show the agency has fielded thousands of complaints about generic versions of both bupropion and metoprolol. Some reports described seizures, cardiac arrest, nausea and other health problems. Others said the pills just didn’t control patients’ symptoms.
Kellermann and others said too many doctors shrug off those concerns, attributing them to bad luck or a patient’s underlying conditions without considering that the medication itself could be the problem.
“Before we blame God or biology, what are we doing with the best intentions that might be hurting this patient?” he said. “If we don’t entertain the possibility that the patient is right, then we might overlook the true cause of their problem. That’s why testing generic drugs to verify their quality and safety is so important.”
Though generic drugs have poured in from overseas factories, the FDA opted to conduct only sporadic testing for quality.Tonje Thielesen for ProPublica
“Afraid of What It Could Find”
Despite its reputation as one of the world’s toughest drug regulators, the FDA takes a decidedly hands-off approach to testing. Its position hasn’t wavered even though the drug supply chain is sprawling, with manufacturers scattered around the world. India produces about half of all generics used in the United States, and crucial ingredients are made in China.
When manufacturers from those countries send drugs to the European Union, they are required to use labs on EU soil to test every batch before releasing them to the public. There is no such requirement in the U.S.
In interviews with ProPublica, former FDA officials and others who have studied the safety of generics said the agency should have done more years ago to probe the drug supply.
Though billions of prescriptions for generic pills, tablets and vials of injectable medication are filled every year, the FDA reported conducting fewer than 650 tests under its quality surveillance program since 2018. That number includes many generic drugs, as well as some brand-name prescription drugs, over-the-counter medications like Children’s Tylenol, and various drug ingredients.
About 94% of those tests produced passing results, FDA data shows. In 2024, the most recent year with data, the agency reported the results of just over 50 tests.
The total does not include tests on hand sanitizers and supplements or any other quality testing that is not publicly reported. The FDA sometimes commissions studies about drugs, which are also not reflected in the tally.
D’Sa said the FDA’s efforts aren’t nearly enough.
Valisure tested drugs for impurities, such as lead and arsenic.Tonje Thielesen for ProPublica
As deputy director of the agency’s India office in 2009, he said he worried that inspections alone couldn’t guarantee Americans were receiving quality medication. His team was scouring facilities in every corner of the country and regularly reporting distressing results: factory after factory with no testing procedures to monitor the strength, quality or purity of drugs. Some factories weren’t being inspected at all.
In 2024, the FDA inspected a third of India’s nearly 600 manufacturing sites, agency data shows.
“Regular testing would be an objective measure of quality,” D’Sa said, noting that inspections only examine manufacturing practices at a single point in time.
Other agency insiders have also been concerned. One former official at the FDA’s Center for Drug Evaluation and Research still remembers a phone call almost 20 years ago from a sobbing woman in Texas who said her husband had switched to a generic version of bupropion that she said wasn’t effective. He killed himself.
“That used to keep me up at night,” said the former official, who did not want to be identified because they still have ties to the agency. The FDA needed more training at its testing labs, among other improvements, the official said, but changes were slow.
In an interview, Janet Woodcock, the longtime head of drug safety at the FDA, said the agency didn’t have the resources to do more testing and that she wasn’t overly concerned about widespread lapses in quality.
“A huge, huge majority of drugs on the U.S. market are totally fine,” said Woodcock, who retired from the agency early last year.
Woodcock did not respond to a question about how she knows that drugs are safe if the FDA hasn’t regularly tested them. Instead, she said, the best way to ensure quality is through training and improved manufacturing.
“I don’t believe random testing is an appropriate method for maintaining quality of the drug supply,” she said.
Some doctors and others said they believe the FDA decided against routine testing because it could undermine the public’s confidence in generics and raise questions about the agency’s oversight of the industry.
“The FDA doesn’t want to do the testing because it is afraid of what it could find,” said pharmacologist Joe Graedon, who for years has advocated for drug safety reforms on his website The People’s Pharmacy.
The FDA has even resisted when groups outside the agency offered to help.
At Valisure, tablets were crushed in advance of testing for heavy metals.Tonje Thielesen for ProPublica
“We Want to Find the Really, Really Horrible Ones”
Nearly every morning before dawn, a truck stocked with more than $2 million in prescription drugs arrives at the University of Kentucky’s hospital. Without fail, chemist Robert Lodder’s team of pharmacy technicians is there to greet it.
While other hospital employees ready the sterile injectables for use, Lodder’s technicians siphon off samples and whisk them off to a small lab tucked inside the pharmacy. There, they put the samples on a machine called a spectrophotometer to get a picture of each drug’s chemical composition.
If the medication is made properly, Lodder and his team would see a similar image for every batch. Too often, something doesn’t look right.
Lodder has screened hundreds of thousands of samples since 2020, representing about 350 different medications. About 10% of those drugs have failed the initial assessment and were removed from the hospital’s supply for further study. Some were cleared after Lodder looked at them a second time, but he was so concerned about 20 different drugs that he reported the problem to the FDA and urged the hospital to change suppliers if it could.
Lodder first became interested in drug quality when he was a graduate student at Indiana University in the 1980s. At the time, people were dying after someone tampered with over-the-counter pain relievers to lace them with cyanide, prompting Lodder to study the makeup of similar drugs. When he took the job at the University of Kentucky in 1988, he urged his bosses to set up a lab to screen medications.
Lodder knew the FDA assessed — and nearly always passed — samples from only a small number of drugs. For sterile injectable medication, which can be particularly dangerous if contaminated, Lodder wanted to look at every vial that came through the hospital’s doors.
“We want to find the really, really horrible ones,” he said. “There’s almost always … a few that you would not want to put out there.”
In 2023, Lodder traveled to Washington, D.C., to talk about his screening program with officials from the FDA and the White House Office of Science and Technology Policy. He had given the group a data file identifying the drugs that failed his initial screening, including chemotherapy drugs to treat leukemia and breast cancer. Lodder expected the FDA to dig into his findings.
But agency officials, he said, asked only a few questions.
“They weren’t listening to us,” he said. “People were indifferent, like, ‘Is this really necessary?’”
The way to ensure drug quality, Lodder recalled pitching the group, is to launch a large-scale testing program and publicize the results, which would force troubled manufacturers to make improvements. He suggested that academic medical centers could do the work: screening medications, pooling their data and reporting results to the FDA and to the public.
His own testing program cost less than 0.01% of the hospital pharmacy’s drug budget.
“Then the public will know who has the best,” he said. “That’s what we want out of all of this: You know who to buy from. You can judge on quality as well as price.”
The FDA did not respond to ProPublica’s questions about Lodder’s proposal.
He went back to Kentucky after that 2023 meeting, convinced little change would come from Washington. Lodder didn’t know the details at the time, but another arm of the U.S. government was just as concerned about the nation’s drug supply as he was.
Valisure’s lab tests for heavy metals. Tonje Thielesen for ProPublica
A Matter of National Security
As a global supply chain commander in the Army, Col. Vic Suarez didn’t rattle easily. But he kept hearing something that, if true, could put soldiers at risk: The military’s doctors were worried that some of the generic drugs they were prescribing, particularly from India and China, weren’t working as they should.
In 2019, Suarez recalled that at least one doctor was specifically troubled by tacrolimus, an immunosuppressant medication used by organ transplant patients to prevent rejection. Some generic versions didn’t appear to deliver the right dose, risking the lives of fragile patients. Suarez started advocating for additional drug-quality testing and took the idea to top leaders.
In 2023, the Defense Department decided to investigate generic medications commonly used by U.S. service members and veterans.
“We saw it as our responsibility to protect our own service members and their families,” Suarez said.
Suarez hoped to explore a collaboration with the FDA, an effort previously reported by Bloomberg. In June of that year, he and a group of officers met with the leaders of the Center for Drug Evaluation and Research.
At the meeting, which has not been previously reported, FDA officials pushed back on the plan. They questioned the kind of testing the Defense Department was planning and the independent lab that would do it, according to a transcript obtained by ProPublica. One said the Defense Department’s concerns about drug quality could damage public trust and “undermine confidence in the drug supply.”
After the meeting, the agency summarized the discussion in a confidential memo, noting that a majority of drugs tested by the agency over the years had met quality standards. The memo pointed to a 2020 FDA study that tested more than 250 so-called “difficult-to-make prescription” drugs and didn’t surface any problems.
The Department of Defense is also using Valisure to test generic drugs. “We saw it as our responsibility,” said Col. Vic Suarez. Tonje Thielesen for ProPublica
“As the agency with jurisdiction over the pharmaceutical industry due to our extensive experience with manufacturing and testing … FDA has substantial concerns about the proposed pilot,” the agency said in the unsigned memo, which was obtained by ProPublica.
The FDA did not respond to questions about the Defense Department’s initiative or the meeting.
The DOD is using the independent lab Valisure to test more than 40 drugs that officials consider the most essential in the military health system, representing roughly 2,000 versions of the medications. The vast majority are generic. Early results show about 10-15% of those drugs are high risk, meaning they were found with elevated levels of contaminants, didn’t have the right dosage or dissolved differently than higher-quality generic or brand versions.
“Ultimately, the people that are disproportionately affected are the most vulnerable,” Suarez said. “There is no other protection for them other than people trying to do the right thing … to literally fill the gap by basically testing and comparing.”
ProPublica also engaged Valisure to conduct drug testing. As part of that testing, the lab earlier this year tested generic tacrolimus made by Intas and found that the capsules dissolved up to three times faster than the name brand, which experts say could introduce too much of the drug too quickly and potentially cause tremors, headaches and kidney failure.
The FDA in 2023 said Intas’ tacrolimus may not provide the same therapeutic effect as the brand name but that the drug could still be prescribed.
In a previous statement, Intas said its tacrolimus is safe and effective and that the FDA had determined the drug was equivalent to the brand-name version when it was first approved for the U.S. market. The company said it “is dedicated to patient safety, product quality, and regulatory compliance.”
Valisure is testing more than 40 drugs that officials consider the most essential in the military health system.Tonje Thielesen for ProPublica
“You Don’t Want a Bad Batch”
Long before ProPublica launched its own testing, Graedon, the drug safety advocate at The People’s Pharmacy, asked another testing provider to assess a generic version of bupropion by Teva Pharmaceuticals, which is headquartered in Israel.
That testing showed the pills were dissolving more rapidly than branded ones. Patients with depression who had once found relief in Wellbutrin had described headaches, anxiety and, in some cases, suicidal thoughts. In 2007, Graedon urged the FDA to investigate, even sending dozens of pill bottles to agency headquarters in Maryland.
In 2012, after sponsoring its own study, the FDA announced that Teva’s version, which was made by Impax Laboratories, was not equivalent to the brand and Teva removed it from the U.S. market.
Teva did not respond to requests for comment. At the time, the company said the medication posed no safety concerns. In 2017, Impax announced it was merging with another company.
Since then, the FDA has only sporadically tested generic versions of bupropion, government data shows, even when drug companies appeared to have manufacturing issues.
India’s Sun Pharma has recalled its bupropion at least six times since 2016 because it wasn’t dissolving correctly, government records show. FDA inspectors have gone back to the Sun factory that made the drug time and again, reporting dirty equipment, fungus in areas that were supposed to be sterile, and bacteria and metal particles in injectable medication.
Still, the agency didn’t test Sun’s bupropion, according to the FDA’s publicly reported results. The FDA ultimately banned the factory from shipping most of its drugs to the U.S. in December 2022, including bupropion, more than a decade after the agency approved Sun’s version of the medication for the market. The factory is still banned.
The company has “acted responsibly and in accordance with good manufacturing practices,” Sun spokesperson James Freeman said about recalls in a statement. He added that the company has made significant investments in manufacturing capabilities in the past five years and is working with third-party experts to meet regulatory standards.
“All of our products remain subject to rigorous quality controls,” he said.
Dr. Douglas Throckmorton, a former deputy director at the Center for Drug Evaluation and Research, said the recalls suggest the agency’s reliance on manufacturers appears to be working.
“You could look at that result and say that’s a manufacturing culture that is doing the needed monitoring,” he said.
Graedon said he still hears from bupropion users, who have continued to post complaints and questions about the quality of various versions of the drug on social media.
“The FDA should be absolutely testing on a regular basis,” he said.
The testing at Valisure ultimately found that one version of the antidepressant bupropion and one version of the heart medication metoprolol dissolved more slowly than their brand-name counterparts, which could leave patients without the right therapeutic levels for treatment.Tonje Thielesen for ProPublica
Consumers have also described concerns about generic versions of metoprolol, the heart medication, but the FDA has not routinely tested that drug for quality problems, either, government records show.
ProPublica’s testing of metoprolol succinate found that a version by Teva, the company that pulled its bupropion from the market, dissolved three times more slowly over a period of six hours than the brand-name drug. The company did not respond to requests for comment.
To Dr. Harry Lever, a retired Cleveland Clinic cardiologist who raised alarms about metoprolol succinate more than a decade ago, the agency’s testing policy dramatically diminishes oversight of America’s drug supply.
“It comes down to the fact that the FDA is not doing its job. Everything you are swallowing should be tested — there should be no question about it,” Lever said. “You don’t want a bad batch coming to the drugstore. People won’t do well. And that’s the problem.”
Resident doctors – formerly known as junior doctors, a term referring to qualified physicians undergoing clinical training – in England are on strike again from December 17 to 22, after the Labour government failed to adequately address concerns over pay and job availability. “Resident doctors need jobs, and when they find those jobs, they need to be paid fairly for them,” the British Medical Association (BMA), which represents tens of thousands of physicians, said in outlining the strike demands.
The dispute over resident doctors’ pay restoration has been ongoing for years.
Los Angeles, CA – In early October, whistleblowers at White Memorial, a Boyle Heights Adventist hospital, leaked invaluable information. The whistleblowers stated that ICE agents were taking detainees from an inadequate ICE facility named “B-18” located within the Metropolitan Detention Center in downtown Los Angeles, to the Chicano neighborhood hospital.
Within the confines of White Memorial, in the emergency department, agents were terrorizing detainee patients. – with permission from hospital CEOs and directors.
Over the last several years, many red states have banned gender-affirming care for transgender youth. Since Trump returned to power, that campaign has shifted to blue states, with the administration threatening hospitals and healthcare systems with the loss of federal funding unless they stopped providing care. This week, those threats escalated sharply: a new federal rule, now in its public…
“Starting next year, American drug prices will come down fast and furious and will soon be the lowest in the developed world,” President Donald Trump claimed Friday as the White House announced agreements with nine pharmaceutical manufacturers. The administration struck most favored nation (MFN) pricing deals with Amgen, Bristol Myers Squibb, Boehringer Ingelheim, Genentech, Gilead Sciences…
Last week, ProPublica published a five-part series that I wrote with senior research reporter Doris Burke about Albany, Georgia, and its only hospital, Phoebe Putney Memorial. We started working on the story five years ago, when COVID-19 was racing around the globe and Albany — small, remote and barely touched by time — had the world’s fourth-highest case rate.
We initially set out to write a David-vs.-Goliath narrative about the town’s response to the crisis. But, as I write in the series, there came a turning point at which we realized there were more enduring questions and challenges facing Albany than COVID-19. They were about race and power.
In the weeks immediately following the outbreak, when the pandemic made it too risky for me to travel, I monitored the city’s daily press briefings and the hospital’s flood of social media posts on Facebook. That, I thought, was where the first draft of Albany’s COVID-19 story was being written, and the narrative that was being pushed in them felt disturbingly familiar.
Albany is a majority Black city of some 67,000 people. However, while Black residents were dying in disproportionate numbers, the officials leading the response were white: the mayor, the chair of the county government and the senior executives at Phoebe. At every briefing, officials announced the number of people who were sick with COVID-19 and the number of who’d died.
Then, in early April 2020, for the first time, they announced a name, not a number. The one person who merited personal recognition was Judge Nancy Stephenson. She was white.
The chief medical officer at the hospital, Dr. Stephen Kitchen, choked up when he announced her death. Mayor Kermit “Bo” Dorough took to the podium to ask for a moment of silence to mark the moment, saying it “brings many of the people in this community to the next phase of this battle because now we know someone who has been a victim of COVID.”
The chair of the county government at the time, Christopher Cohilas, proclaimed, “We have lost a tremendous jewel of this community. A jewel to the people.” Then he added, “I think that her passing highlights exactly how lethal this disease can be.”
I’m not going to lie. I cringed at what I was hearing. Some 38 people had died by then. The overwhelming majority were Black. There hadn’t been any named mentions or moments of silence at the press briefings for them. How could it be, I thought to myself, that it wasn’t until Stephenson’s death that the city’s leaders understood how lethal the disease could be?
The comments that came pouring into the live chat of the video briefing made clear I wasn’t the only one asking that question.
One read, “Let’s not forget all the others who have passed, and who are known by others in our community.”
Another read, “So you extend condolences to the judge, but not your residents.”
And then there was this: “So now it hits home.”
That moment resonated with me because two decades earlier I’d written a piece as part of a Pulitzer Prize-winning series for The New York Times about how histories written by people in power — most of them white — tend to erase, minimize and misrepresent the experiences and contributions of those who are not.
That story was also set in the South. The series, titled “How Race Is Lived in America,” was meant to show how the systemic divisions that shape our society and each individual’s place in it are driven by day-to-day interactions at work, at school and in hospitals.
What I was seeing play out in Albany and at Phoebe felt like the stuff of a new installment. Not only did it seem that city leaders had failed to recognize the magnitude of the crisis until one of their own had died, they had also made those bearing the brunt of the pandemic feel responsible for their own demise. According to the official narrative, the outbreak started at a Black funeral, and the reason Black people were so vulnerable to the virus was because they didn’t take care of themselves.
On my first visit to Albany, I met Pastor Daniel Simmons, the leader of Mt. Zion Baptist Church. He made clear he was skeptical of the prevailing narrative and encouraged me not to fall for it either.
“If Albany, Georgia, had done things differently over the years, our community wouldn’t have been as vulnerable as it was,” he said. “If the health care system was different, if it had a different relationship with poor people and people of color, the outcome would have been different.”
The main lesson that he hoped I and other people would take from Albany’s COVID-19 crisis was: “It didn’t have to be this way.”
What he and others told me had been left out of that narrative was how hard it had been for African Americans in Albany, particularly those who are poor and uninsured, to get safe and affordable health care in a city whose dominant institution is a hospital. Phoebe Putney Health System is not only the largest provider of health care in southwest Georgia, it is also Albany’s largest employer and property owner. The health system’s CEO, Scott Steiner, said the hospital’s mission is to provide care regardless of race, religion and ability to pay, “but we’re always trying to balance that out with paying the bills.”
Doris and I spent the following four years exploring that part of Albany’s story, interviewing more than 150 sources and poring over thousands of pages of records. We learned that Phoebe was the only hospital in town because it had worked hard — even stealthily — and spent millions of dollars to drive out its old competitor, before finally managing to acquire it. The cost of care went up and quality went down. Meanwhile the more Phoebe grew, the more economically dependent Albany became, and the harder it was for patients to hold the hospital to account.
The CEO that oversaw Phoebe during the period of its most significant growth and the health system’s former attorney did not respond to detailed lists of questions. When we asked Phoebe’s current leaders for responses to our findings, a hospital spokesperson accused us of intentionally excluding positive patient stories. “Most patients have positive experiences at Phoebe,” he said. “Ignoring that fact is wrong.”
As for Doris and me, we were determined to focus on the people who tend to get left out of Albany’s, and the nation’s, stories because we believed they would resonate with anyone who has struggled to get the health care they need. We hope you’ll spend time with the whole series. You can read it here. Or you can listen here to an audio version, produced in collaboration with actors from Theater of War.
Above photo: President William Ruto has tried to reassure Kenyans over the deal. AFP via Getty Images. Kenya is auctioning its sovereignty to foreign powers. The final item on the block is the genetic data of its own people. Nairobi — It is hardly uncommon to hear Kenyans complain that their President, William Ruto, is […]
In late November, a mental health leader at a major VA medical center learned about a directive issued to the 18 Veterans Health Administration (VHA) regional offices, known as VISNs (Veterans Integrated Service Networks). Department of Veterans Affairs’ leaders in Washington were imposing lower caps on employee positions nationwide. Directors of local VA medical centers and clinics had a month to decide which vacant positions to eliminate, and which job offers to rescind. None of these identified positions would be filled because they would be swept from organizational charts entirely.
Wrapped in a flashy fur coat she’d found at a thrift store for the occasion, Hannah Goetz blew out the candles on her favorite red velvet cheesecake. It was her 21st birthday. The celebration with her family that evening in February 2023 was a milestone not just for her age, but because she was alive.
Three and a half years before, her lungs had collapsed from cystic fibrosis. She was saved by a double-lung transplant that had been allowing her to breathe deeply. Hannah had slowly worked her way back to stable health, overcoming infections and, every day, taking a crucial medication to protect her donated lungs from rejection. Her doctors were optimistic.
Hannah had been feeling well enough to sing karaoke, work as a nanny while taking college classes and begin her first adult relationship, with a Navy sailor. Her 21st birthday gift from her mom was a trip to Nashville, Tennessee, where the two of them and their friends could explore the city’s music scene and cavort in its bars.
Just days after her birthday, though, she was back in the hospital. She’d been feeling her chest tighten, and she struggled for air. By March, Hannah felt as if she were breathing through a straw. Tests showed she was taking in less than half the oxygen of a healthy person.
One of the first questions came from her transplant team’s pharmacist, who had overseen her medications since her operation.
“Did the tacrolimus pills you take change?” he asked.
Most people have never heard of tacrolimus. But to anybody who has received a transplant, it’s nothing short of a miracle. The medication prevents organ rejection. Without tacrolimus, a simple capsule taken twice a day, cells in the blood identify the transplanted organ as a foreign invader and treat it like an infection, trying to rid the body of it. That attack can be fatal.
A team of Japanese scientists discovered tacrolimus in the 1980s, in a fungus found in the soil of a lush, purple-hued mountain north of Tokyo.
Along with another similar drug, tacrolimus radically improved the long-term prospects of transplant patients. The chances that a donated organ would still work after a year roughly doubled for those who used the drugs. Recipients of kidney, heart and liver transplants started living years longer. So did lung patients, but the challenges of those transplants meant the increases in lifespan were smaller.
By the numbers, if Hannah made it past her first year, she could expect her new lungs to give her nine more years of life.
Hannah was upbeat during regular two-week hospital stays — she dances here during one visit in 2015 — which were often needed to treat infections after she was diagnosed with cystic fibrosis. Courtesy of Holly Goetz
Hannah was in fourth grade in 2012 when doctors figured out that her regular bouts of bronchitis and her struggle to gain weight were caused by cystic fibrosis, a genetic disease that leads to mucus building up in the lungs and other organs. The disease is ultimately fatal.
Ten-year-old Hannah sat listening for hours as a medical team explained the diagnosis to her and detailed how it was treated. The doctors managed to avoid any discussion of mortality, and it wasn’t until Hannah got home that she found the answer she sought online. At that time, the median lifespan was less than 40 years. Mom, she asked, did you know I won’t live as long as most people?
Holly Goetz, a high school teacher who was newly divorced and shouldered almost all of her daughter’s care, tried to reassure Hannah. Her case wasn’t severe, she told her daughter. And new advancements could improve the outlook.
Hannah didn’t dwell on the diagnosis, and she managed to keep up with peers in her Isle of Wight, Virginia, school, playing soccer and singing in musicals. Like any tween, she documented every moment of her life in a series of selfie videos. In one from fourth grade, she chatted to the camera as if she were a jocular TV host, capturing the twice-a-day event when she wore a device that looked like a life preserver and shook her chest to break up the mucus in her lungs. “Here I am, vibrating, whooo!” she trilled in rhythm with the pink vest. She ended the video, “See you next time on Vest Treatment with Hannah.”
Sometimes, she also needed a feeding tube hooked up to her stomach at night to ensure her body absorbed enough calories. And there were occasional two-week stints at the local children’s hospital for a course of antibiotics.
Still, she graduated high school a year early, as a 17-year-old, in June 2019. That month, sporting purple streaks in her hair, she’d gone with her family to the Caribbean to celebrate her achievement. She was looking forward to attending Longwood University, a couple of hours west from her hometown.
Hannah, whose signature pose was sticking her tongue out, was relatively healthy during her teen years despite having cystic fibrosis — at least, until she was 17.
One afternoon not long after returning from the trip, Hannah told her mom she was feeling sick. Holly packed up, thinking they were headed to the hospital for a standard “tune up.”
This time, though, Hannah quickly went from sitting up in her hospital bed, mouthing along with the “Frozen” song “Do You Want to Build a Snowman?” to a ventilator in the pediatric ICU. She had pneumonia, which was filling her already clogged lungs with even more fluid. Hannah also had an infection from a rare bacteria that had caused sepsis, a type of potentially lethal inflammation. Before Holly could process what was happening, Hannah was in an ambulance, being transferred three hours north to the better equipped Inova Fairfax Medical Campus.
The doctors said the prognosis was dire: Hannah’s lungs were too damaged to recover, and she needed a double-lung transplant. But the infection was proving insurmountable. Hannah was stuck on the wrong side of an agonizingly thin line: A patient needs to be severely compromised to qualify for a replacement organ; but if they’re too gravely ill, they’re ineligible.
The transplant team proposed something bold. The only way to give Hannah a chance, they said, was to remove both of her lungs — without knowing whether they’d find new ones for her — in the hopes that if they went, so too would the infection. That would clear the way for her to be added to the transplant list.
For four days, Hannah lay unconscious in the ICU with no lungs while machines pumped her heart and tubes the size of garden hoses circulated oxygen through her body. Holly curled her lanky frame into a chair by Hannah’s bedside every night. She prayed first that the infection would clear and then, later, that a lung donor would be found.
The risky move was a success. When Hannah awoke in August, fully conscious for the first time in three weeks, she had no memory of what had happened. Her mom told her everything was going to be OK; she had new lungs.
Hannah spent 67 days recuperating in the hospital. At first, she could only take a few tentative steps from her bed with the aid of both a walker and a nurse. She ultimately strode out of the hospital with her arms flung above her head in triumph. Doctors marveled, saying that Hannah had been saved by her youth and surprisingly healthy body.
Hannah posed for a picture with her care team, including transplant pharmacist Adam Cochrane, and her mom, Holly Goetz, the day she was discharged from the hospital in 2019 after her transplant.Courtesy of Holly Goetz
Medications are so central to recovery from a transplant that the federal government requires hospitals to assign a pharmacy expert as part of a patient’s team. For Hannah, that person was Adam Cochrane, a specially trained transplant pharmacist with two decades of experience who worked exclusively with lung- and heart-transplant patients.
Cochrane, who has a calm, measured disposition, tried not to overwhelm Hannah and her mom as he taught them about the lineup of pills Hannah now needed to take. The daily regime was critical. She can’t live without these medications, he told them. Hannah would need to take tacrolimus twice a day at the same time every day — for the rest of her life.
Tacrolimus is part of a special category of drugs that work only if the dose is calibrated within a very narrow range. Any amount outside that window can be dangerous, particularly for lung transplant patients, who face high rates of rejection. To make sure Hannah was getting the correct dose of tacrolimus, Inova would test her blood every other week to start and then once a month after that. (Inova said that it doesn’t comment on individual cases but that it “collaborates closely with transplant recipients to ensure they access appropriate medications to maximize the likelihood of a successful outcome.”)
There’s no formula that tells Cochrane what dosage each patient needs, so he tinkered to find the sweet spot. He thought of it as a teeter-totter. Too much tacrolimus and the immune system would dip too weak to ward off infection. Too little tacrolimus, and the immune system would tip too strong and attack the transplanted organ. Cochrane knew that a steep tip in either direction was potentially catastrophic.
For years, tacrolimus was made by one company, now called Astellas, which had discovered and patented the drug. When generic versions arrived 15 years later, none behaved in the body exactly like the original tacrolimus or like one another. To make a generic, most companies have to reverse engineer the brand drug; there’s no recipe to follow. Each generic is a distinct formula made in a distinct way.
As with all generics, the tacrolimus versions approximated the original within a broad range set by the Food and Drug Administration. In general terms, it’s how much a generic can differ from the original brand in the amount of the key ingredient that reaches the relevant part of the body and when.
As the FDA considered the first generic version of tacrolimus in the mid-2000s, the agency had to decide whether there should be stricter rules for generic versions of the small number of drugs like tacrolimus that require such precision dosing. Canada and the European Union both adopted tighter standards. Those governments essentially halved the range considered to be a match for the brand drug.
But the U.S. continued with a one-size-fits all approach, allowing the looser standards that treated tacrolimus like any other generic drug. The agency said in 2009 that it was confident that its “method for approving generic tacrolimus uses appropriate bioequivalence standards.”
The FDA approved the first generic version of tacrolimus that same year. In May 2010, one made by an Indian generics company called Dr. Reddy’s was approved. The next year, so was one made by another Indian company called Intas, whose U.S. brand is called Accord.
In all, six generics were greenlit before the FDA reversed course and decided in 2012 that tacrolimus should, after all, be made under tighter criteria. But the rule applied only to companies newly approved to sell a generic version of tacrolimus. The agency did not require Dr. Reddy’s, Accord and the others already on the market to meet the new standard. The agency stated later in a public filing that it doesn’t retroactively apply new standards to existing products.
Almost from the beginning, some transplant doctors had raised concerns that patients on Dr. Reddy’s tacrolimus were faring worse than those on other generics. The Cleveland Clinic was so alarmed that it banned Dr. Reddy’s generic for its transplant patients in 2013. Later, at the Tulane Transplant Institute, doctors found that patients taking generic tacrolimus by any drugmaker had a higher chance of organ rejection, and the hospital decided to use only the brand drug.
At Inova, Cochrane had noticed irregular fluctuations in patients taking Dr. Reddy’s as well as early signs of organ rejection. “Omg! … Another [patient], victim of Dr Reddy,” an Inova nurse wrote in a 2019 email obtained by ProPublica.
Holly knew none of this when she picked up her daughter’s tacrolimus at the local Kroger grocery store after Hannah’s discharge in the fall of 2019. (Kroger didn’t respond to requests for comment.) Unlike with Hannah’s medical care, where Holly could research and choose a doctor or hospital, the brand of generic tacrolimus Hannah received was out of her hands. She would get whichever one that pharmacy happened to have in stock.
Inova’s transplant team had typed, in the electronic prescription that it sent to Kroger, “do not dispense Dr. Reddy.” But that’s what Hannah received.
Just months after Hannah was discharged from the hospital with her new lungs, COVID-19 shut down the world. Holly couldn’t believe she had to be on guard against yet another threat, one so dangerous to her immunocompromised daughter. Lungs are among the trickiest organs to protect, in part because they draw in germs in the air with every breath.
Despite those threats, Holly found a kind of appreciation for the moment. The pandemic meant she could keep 18-year-old Hannah, otherwise eager to leap back into life, tucked away at home during her perilous first year after the transplant. When she’d first been discharged, Hannah had shown a streak of teenage rebelliousness. She was quick to drive off in the pumpkin-colored Jeep Holly had given her and get tattoos and piercings, risking infections that transplant patients were supposed to avoid.
Holly Goetz in her bedroom this year
Hannah lived through the COVID-19 quarantine with her mom and younger brother in their modest clapboard house on a neat suburban street. The three of them, and their newly adopted St. Bernard-poodle mix, Miracle, made dance videos together, and at night, Hannah curled up to sleep in her mom’s bed rather than head to her own room.
That year, Hannah’s lung function improved to normal levels as her body grew stronger. When the pandemic began to recede in 2021 and Hannah ventured out more, Holly remained diligent about her daughter’s tacrolimus, making sure she took it every morning and night. Holly insisted Hannah either send a video of her taking the medication or FaceTime while she did so.
Cochrane and the team observed fluctuations in Hannah’s tacrolimus levels. They’d adjust her dosage to try to keep her at the optimal amount. Cochrane concluded that Hannah was perhaps not taking her medication at the same time every day, he told ProPublica. That’s not unusual for young patients. Her adherence to other drugs unrelated to rejection had proved spotty. Hannah wasn’t always diligent about taking the enzymes she needed to aid her pancreas and keep her weight up, and she declined to continue a new cystic fibrosis medication that she didn’t feel was giving her results.
But Cochrane said he didn’t think any sloppiness with her tacrolimus meds fully explained the wild swings he often saw when she was admitted to the hospital to treat an infection. His experience with other patients had convinced him that the generic versions of tacrolimus varied significantly, enough to harm the health of a patient.
During one inpatient stay at Inova in August 2021, Cochrane gave Hannah the same dose of tacrolimus she took at home. But he used a different generic from the hospital’s pharmacy. Cochrane expected to see steady levels of the drug in Hannah’s system. Instead, the amount of tacrolimus was much higher than it had been. He said he couldn’t remember why he didn’t ask Hannah about which brand of generic she was using.
During the COVID-19 quarantine, Peyton, Hannah’s brother, would make dance videos with her and their mom.
Well before Hannah began taking the drug, there had been concerns inside the FDA about whether tacrolimus generics were being made correctly, according to an agency drug official who was there at the time. The manufacturing process for tacrolimus is particularly complex.
The medical community had kept pushing the FDA to do more to verify the effectiveness of tacrolimus generics, and in 2013 the agency acquiesced and commissioned a study. That study, which was completed in 2015 and included Dr. Reddy’s, identified a problem with one generic: the version made by Accord. It didn’t mimic the brand drug as it was supposed to.
But the agency decided those results were not definitive. The FDA didn’t make the findings public, and Accord’s tacrolimus remained on the market.
In 2021, an FDA-commissioned follow-up study showed unequivocally that Accord was not equivalent to the brand drug, potentially delivering too much medication to the patient. But once again, the FDA did not warn the public. Accord continued to be sold as usual.
A few months later, in December 2021, Kroger began filling Hannah’s prescription with Accord’s version of tacrolimus.
At first, the new generic seemed to have no negative effect. Hannah had fewer bouts of infection than the year before. She was feeling the best she had since the operation, faring well enough that Holly thought it was OK to leave her for the first time and go on a cruise.
That year, in July 2022, Hannah marked her three-year transplant anniversary on Instagram with a close-up picture of her “bad ass scars.” They were a sort of tattoo she hadn’t chosen, but, as she wrote, they “will always remind me that I got a second chance.”
Both Hannah and her mom were taken by surprise when Hannah’s breaths became shallow around the time of her 21st birthday in 2023.
“i wish i was out and about with friends and family enjoying the weather but unfortunately my reality has been me cooped up in a hospital room,” she posted to Instagram in March. “I put on a brave face for all my loved ones, but deep down it affects me everyday.”
Hannah celebrated her “lungiversary” one year by taking the roof and doors off her orange Jeep and convincing her cousin to get matching Saturn and moon tattoos.Courtesy of Holly Goetz
The next month, tests confirmed that Hannah’s lung function had declined precipitously. If she’d been breathing through a soda straw before, now it was closer to the thin red ones used to stir coffee.
Cochrane asked what brand of tacrolimus she was taking. He always had to sleuth a bit to figure out what might be going on; perhaps a patient had chronic digestive problems or their diet had changed, affecting the absorption of tacrolimus. He was most concerned that a patient had been on Dr. Reddy’s. Cochrane was not suspicious of Accord at the time; the FDA hadn’t made its study results public.
Holly went home after the conversation with Cochrane and scoured her medicine cabinets. It was the first time she’d ever had a reason to look at the manufacturer. Cochrane had trusted pharmacies to follow Inova’s instructions, and so he hadn’t previously warned Holly to avoid Dr. Reddy’s. Sure enough, Hannah had old bottles labeled Dr. Reddy’s. Cochrane told Holly to throw them away.
For more than three years, Hannah had exclusively taken tacrolimus manufactured by companies that had alarmed either doctors, pharmacists or the FDA. Cochrane would later wonder if there had been a cumulative effect — chronic rejection is “sneaky and slow” — and Hannah had now reached a tipping point. Her donated lungs were failing.
Hannah’s mood darkened as her decline accelerated. In April 2023, back at her local hospital yet again, she snapped at the nurses. Everyone was always telling her how strong she was, she fumed. She wanted out of that room. When she counted the days she’d been home rather than hospitalized since late January, she realized it had been only 20.
“I don’t want to do this again,” Hannah told her longtime respiratory therapist.
Anxiety gripped her at all hours. She couldn’t breathe.
That month, a biopsy had confirmed that her body was rejecting her lungs, precisely what tacrolimus was supposed to prevent. The damage was irreversible.
“Once again, they’ve decided i need new lungs,” Hannah wrote on Instagram. “It’s happening a lot sooner than anyone expected.”
Hannah checked into Inova in June with the expectation that she would have a second lung transplant. But as she got increasingly sick, she spent the next five weeks being moved between the transplant wing and the ICU two floors below. Holly was vigilant by her side. When Hannah lashed out because there was a tear in her pink security blanket, the one she’d had every time she was hospitalized since she was 10, Holly paid someone double to patch it in one hour. She followed doctors into the hallway after they checked on Hannah. Her daughter had done everything they’d asked of her. When was she getting new lungs?
Doctors wanted Hannah to be able to stand up and walk, a sign she was strong enough to survive a second transplant. Holly encouraged Hannah to push through the discomfort, thinking to herself, “You’ve got to show them you want to live.” Hannah lacked the energy to even speak most days. She agreed when the transplant team proposed a tracheostomy, a surgical procedure to place a tube into her windpipe to help her breathe. That way, she could have the benefit of a portable ventilator and still do the required physical therapy. On a sheet of printer paper, she wrote in shaky letters that she needed the vent.
“hurry”
“hurry”
At 3 in the afternoon after Hannah received the tracheostomy, the transplant team called a meeting with Hannah’s family. Standing in a conference room in clothes she’d worn for days, Holly listened in shock as doctors explained that Inova would no longer consider Hannah for a transplant. Hannah was underweight, she had poor kidney function that would likely require dialysis and she had a persistent sinus infection. Hannah was simply too fragile.
How could you deny someone so young? Holly asked again and again. What about the medication, the Dr. Reddy’s? No one had told her to look out for that until Hannah was already in rejection. Didn’t they owe her another chance?
Over the next few days, while Hannah was sedated, Inova searched for other transplant programs. Temple University Hospital in Philadelphia was the only facility willing to evaluate her. She’d have to start over with a new transplant team.
Who’s going to tell Hannah? Holly asked. It wasn’t going to be her.
Hannah lacked the energy to speak most days, so she would communicate by writing on printer paper. She asked for a ventilator to help her breathe.
Hannah lay in the intensive care unit with her blond hair slicked back off her face, puffy from the side effects of aggressive medications. She was gently roused from sedation. Several transplant doctors hovered at her bedside. Hannah looked with confusion at her mom and grasped her hand.
Christopher King, Hannah’s favorite among her transplant doctors, tried to help her understand what was happening. “You’ve been a little bit in the dark for the last day or so. You’ve been sedated,” King said. “Things have changed a little bit over that time.”
He told her he wasn’t sure she’d survive a second transplant. He didn’t want to put her through more suffering if, in the end, it wouldn’t help. “We don’t think we should offer you a transplant here,” he said.
Hannah, unable to speak because of the tracheostomy tube, reached her pale hand for a marker and wrote on a small dry erase board: “I don’t wanna die. I’m only 21.”
King told her she could go to Temple, but she would need to be off the ventilator during the day and be able to walk a lap around the ICU to be eligible for a transplant. Even if she could do that, a transplant was not guaranteed.
“Do you want me to give you some time?” King asked.
Holly watched her daughter fade back into sedation, and she knew: Hannah was done fighting. Holly had begged the surgeon to do everything to keep Hannah alive. She had begged the director of the transplant program. She had begged other hospitals. She would not beg her daughter.
“I’m sorry,” Hannah wrote after waking a short time later. She didn’t want to try for a second transplant. She was ready to let go.
Hannah took her brother’s hand and made him promise he wouldn’t forget her. She FaceTimed with friends, mouthing that she loved them. She pushed to stay awake for goodbyes with her father, grandparents and other family.
As nighttime fell, Holly sat by Hannah’s side, in the glow of two lava lamps. Holly told her how proud she was and that she understood that she couldn’t do it any more. “You’ve made me so happy,” she said. Holly was sorry she hadn’t done something more to save her.
Hannah was gasping for air. She needed more Dilaudid, an opioid that is about five times stronger than morphine.
Holly knew it was time. She walked out into the harsh light of the nurses’ station and requested the drugs that would slip her daughter into unconsciousness for good. “Is this really happening?” she thought to herself. “Did I just talk to her for the last time?”
At 10:48 p.m., the doctors removed Hannah’s ventilator.
Holly found a note in Hannah’s phone: “dear mom, i think eventually you will find this, and when you do i don’t want you to get sad.” She assured her mom she’d had a great life, “and you truly are my best friend.”
“i fought so hard and this time luck just wasn’t on my side.”
Holly and Peyton, who is now 19
When Hannah died at 8:19 in the morning on July 16, 2023, eight years had gone by since the FDA’s first study raised questions about Accord. Two years had passed since the FDA had definitive results that Accord didn’t match the brand-name medication.
Two months after her death, in September 2023, the FDA finally took public action. The agency announced that Accord’s tacrolimus doesn’t “provide the same therapeutic effect” as the original brand-name medication. That step would stop many prescriptions, since some states bar pharmacists from automatically dispensing a generic flagged in that manner. Still, in the very next sentence, the FDA added, the pills remain “FDA-approved and can be prescribed.” The agency told ProPublica that it needed two years to review and release the study results in order to “evaluate the potential public health impact” and determine what to do about the drug. (The FDA answered questions about its handling of tacrolimus generics but didn’t respond to questions about Hannah’s specific case.)
The problem, the agency stated, was that Accord’s drug could provide a toxic dose to a patient. But the FDA said that did not cause an increased risk for organ rejection, because the amount of drug in the body when measured at its lowest concentration was not significantly different than the brand drug.
The FDA should have moved quicker, Janet Woodcock, the longtime head of drug safety for the agency, told ProPublica. “This obviously is a quality problem with Accord,” Woodcock, who retired in 2024, said. Scientists had gotten caught up in debate about how significant the results were, she said. “That doesn’t excuse the fact that the agency should immediately jump on these things and try to sort them out,” she said, adding that tacrolimus for transplant patients is “crucial to health and should be right.”
An Accord spokesperson said in a statement that the company can not comment on individual cases but that it is “dedicated to patient safety, product quality and regulatory compliance.” Accord maintains that its tacrolimus is safe and effective. The FDA recommended in 2023 that the company do new studies to prove its bioequivalence, but shortly after, the FDA banned two of Accord’s factories in India from selling drugs in the United States, citing a “cascade of failure” in the company’s manufacturing. The work on tacrolimus is on hold while the import ban remains in place.
ProPublica hired Valisure, an independent lab, to test both Accord’s and Dr. Reddy’s tacrolimus. Valisure used peer-reviewed methods designed to compare the quality of generics, a method adopted by the Department of Defense. The tests concluded that Accord dissolved too quickly, raising the possibility of too much active ingredient at the outset and then too little after the surge. In tests that focused on dosage, three out of seven sample batches didn’t provide enough of the medication, including pills that were supposed to be 0.5 milligram, 1 milligram and 5 milligram doses.
Dr. Reddy’s tacrolimus, which is still sold in the U.S., also fared poorly. The lab found that it dissolved up to twice as fast as the brand-name drug. A 2021 study by Cleveland Clinic doctors found similar results.
A Dr. Reddy’s spokesperson said in a statement that the company’s version of tacrolimus was approved based on rigorous studies; the statement added that all batches sold in the United States have met FDA specifications and FDA studies didn’t reveal any problems with its tacrolimus. The company said the independent lab did not use the FDA-approved testing method, so the results “cannot be considered an accurate representation of Dr. Reddy’s dissolution performance.” Dr. Reddy’s did not receive a complaint about Hannah’s case nor any other complaints that “indicated any concerns in patient safety,” according to the statement. “Patient safety and consistent product performance remain our highest priorities.”
Hospitals like Inova and the Cleveland Clinic today advise patients not to take Dr. Reddy’s and Accord’s tacrolimus. Cochrane had another lung transplant patient die this year after experiencing rejection that he ties to Dr. Reddy’s tacrolimus. Like Hannah, the patient received that brand despite Inova’s instructions on the prescription, and it’s impossible to say with certainty what caused the organ rejection. Since 2019, Cochrane has reported to the FDA database that tracks “adverse events” related to drugs four episodes in which he suspected that Dr. Reddy’s tacrolimus contributed to organ failure or the death of a patient.
Cochrane understands that patients could use brand-name tacrolimus and still suffer organ rejection. And no one knows what exactly caused it in Hannah’s case.
But Cochrane told ProPublica, “I believe her medicine contributed to her rejection.”
Holly wants to hold someone accountable, but it’s extremely difficult to sue the FDA and lawyers told her it was impossible to draw a straight line from Hannah’s death to a generic manufacturer.
Holly is tortured by the question of whether Hannah would still be alive if she had been on a different brand of tacrolimus: “I just wish I had known.”
These days, with Hannah’s younger brother at college, Holly’s house feels too quiet. Each night, she falls asleep holding Hannah’s worn pink blanket.
The Samaritan Clinic is a small, free clinic serving people without health insurance in Albany, Georgia. It was created in 2008 to provide care for people who couldn’t afford medical treatment. More than 15 years later, the need has changed little. Today, Albany has one of the highest poverty rates in the state. About 16% of residents are uninsured, nearly double the national average. And people here pay some of the highest commercial health insurance rates in the country.
Not far from the Samaritan Clinic is Phoebe Putney Memorial Hospital, Southwest Georgia’s largest hospital — a nonprofit founded on the principle that patients should be treated regardless of their ability to pay.
So why do some residents turn to a free clinic for care?
Trump administration officials on Thursday announced new proposed regulations targeting gender-affirming care for youth, part of a larger push from the Department of Health and Human Services (HHS) to restrict such care. One of the new proposed rules would ban hospitals that provide gender affirming care to youth under 18 from receiving Medicaid and Medicare funds.
The U.S. has the highest medical and health care costs in the world — a reality that is driving 1.2 million medical tourists from there to Mexico each year, where up-front costs are lower. Yet for Mexicans whose wages or incomes are many times lower, living in the country with the most expensive medicine in Latin America presents an obstacle to treatment. Mexico faces serious…
It quickly became clear through our reporting that patients and doctors don’t reliably have the information they need to make informed decisions about the medicines they take or prescribe.
ProPublica has created Rx Inspector, a tool that aims to help.
You can look up your generic prescription drugs, and we’ll guide you to the specific facility that made them. We were able to link more than 80% of generic prescription drug products in our database to a factory that made them using databases of label information, manufacturing facilities and location data that we sued the FDA for. Additionally, we included the history of FDA actions at those facilities based on a trove of inspection records we assembled.
Keep in mind that if you turn up a troubling inspection report, it doesn’t necessarily mean that your drug is compromised. Doctors and pharmacists advise that you not stop taking your medications. Instead, you should talk to your health care provider about any concerns.
Our ongoing reporting has focused on the safety of generic drugs, which represent the vast majority of all prescriptions filled in the United States. Thus, Rx Inspector does not include brand-name or over-the-counter drugs, at least for now. We excluded gases (like oxygen tanks) and intradermal route drugs (many of these were allergy tests for things like feline hair).
ProPublica described the app and the methodology used to build it to the FDA, which did not comment. The agency previously told ProPublica that it doesn’t reveal where drugs are made on inspection reports to protect what it deemed confidential commercial information.
Here’s how we did it:
Getting Lists of Drugs and Facilities
First, we needed to get a list of prescription drugs. We downloaded the National Drug Code product list from the FDA. A company that wants to make a generic must file an Abbreviated New Drug Application for approval. We used those ANDA numbers to filter our list to generic drugs only.
We included biological drug products, such as insulin. We opted to include authorized generics, which are brand-name drugs that are marketed without the brand-name label, because we thought consumers may not know their “generic” is actually a brand-name drug.
We then joined that list of drugs to the Structured Product Labeling database from DailyMed, a National Institutes of Health resource that contains information on more than 155,000 drug labels submitted to the FDA by companies. We used that data to get basic information about the drugs, like the form (pill, injectable, etc.), dose, color, imprints and more. In some, but not all, cases, it also contained identifiers or addresses that we could use to link to the agency’s official list of manufacturing locations.
We then matched the drugs to three different facility lists:
The first and primary list comes from the FDA’s Electronic Drug Registration and Listing System. That database contains the addresses of drugmakers’ factories. It also has two numeric identifiers: the FDA Establishment Identifier and a Dun & Bradstreet, or DUNS, number.
The second facility list comes from a federal lawsuit we filed against the FDA for a list of manufacturer addresses connected to their ANDA numbers among other information. We received a partial list, which we used when we only had ANDA numbers for a drug.
And finally, we have a list of historical facilities, which allows us to identify production sites and link to them via FEI number if other routes don’t work.
Joining Them Together
In October, we detailed our unsuccessful search for the original manufacturer of a popular cholesterol generic through a labyrinth of company names and complex databases that few consumers would even know exist. We decided we had to do something similar for nearly 47,000 drug products.
Different datasets had varying identifiers, and we had to link multiple together to find the correct facilities. For example, if all we had was an ANDA number, we used the facility list we obtained from our lawsuit, which also was listed by ANDA. If we had an FEI, we could link it to the FDA’s official list of facilities.
Sometimes, we had neither. In cases where we did not have any useful identifiers, we searched the product labeling data for any manufacturing addresses and attempted to match them to our facility lists. We used both fuzzy text matching and geocoding to do this and then manually reviewed our matches.
For repackaged or relabeled drugs, we traced back to the original label using the source NDC code.
In total, we were able to match more than 39,250 products to a manufacturing facility.
Getting the Inspection Data
Linking up individual drugs was only half the battle. The next thing we did was acquire the FDA’s inspection outcomes for facilities and join them back to our facility lists.
We acquired data on FDA inspections from a variety of sources. First, we turned to the FDA’s public inspections dashboard for inspections since 2008. We used only information related to drugs or biologics, excluding inspections related to food, cosmetics, tobacco, medical devices and veterinary products. This dashboard contained the dates and outcomes of inspections, as well as citations detailing any violations of federal code. We linked these reports back to a facility with a matching FEI number.
That still only gave us limited information for inspections. For documents with more details, we needed what’s known as a Form 483, which is where inspectors document problems they observe at a facility. Unfortunately, the FDA does not make all 483s public. We began by exporting those that have been published in the inspections dashboard, though we know this is incomplete.
We also went directly to the FDA and asked for all the 483s that had already been released publicly. They delivered a trove of almost 40,000 documents.
We linked the 483s to an inspection by extracting text from the documents using optical character recognition, connecting them to a facility using the FEI number and finding inspections of that facility within 10 days of the date of the letter. We were unable to link every 483 to an inspection because the FDA’s public inspections data does not include every inspection the agency conducts.
The FDA publishes warning letters that detail “significant violation(s) of federal requirement(s).” We obtained these from the FDA’s website going back to 2020, filtered out the ones not related to drugs and connected the rest to a facility using the FEI number.
Some facilities are outright banned from sending drugs to the U.S. market for a time, with exceptions for certain drugs as ProPublica detailed in reporting this year. The FDA calls this an import alert.
We used the Internet Archive’s Wayback Machine to find hundreds of import alert lists published by the FDA over more than 15 years. The lists identified factories banned from shipping drugs to the United States because the FDA found manufacturing violations.
We focused on 66-40 alerts, which call out drug manufacturing facilities that do not meet “good manufacturing practice” standards. We considered the published date on the alert as the start date. We are unable to tell when an alert was lifted and instead approximate it using the date we last see the facility on the list. Import alerts do not include FEI numbers to easily identify the facility in question, so we used the entity name and address to tie them back to a facility.
We attempted to identify exemptions to import alerts by looking for strings like “excluded from DWPE” (“detention without physical examination”), then parse it manually to get a clean list of drugs.
To support our research, we paid for access to Redica Systems, a quality and regulatory intelligence company with a vast collection of FDA inspection documents. We used Redica’s database to spot-check our own work.
We know that much of the data represented here is likely an undercount. Clerical errors could have resulted in missed connections. The FDA sometimes removes inspection outcomes from its dashboard, and our method of scraping through the Internet Archive is subject to availability. We were also limited in how completely we could obtain 483s, warning letters and import alerts. There may be additional communications between the company and the FDA that are not reflected in our database because they have not been made public.
Still, this is the most comprehensive public list of FDA actions tied to drugs that has ever been assembled.
With every bottle of prescription medication comes an implied promise: The drugs are safe and effective and meet strict standards set by the Food and Drug Administration.
But the agency known as one of the world’s toughest regulators provides only intermittent oversight of the foreign factories where generic drugs are made. And when investigators turn up mold, filthy equipment and contaminants in those facilities, the FDA keeps the names of the drugs they make secret.
Consumers often have no way of knowing if the medications they are taking came from factories that used dirty water, were infested by insects or birds, or were outright banned from shipping drugs to the U.S., but then granted special exemptions to do so anyway.
Today, ProPublica is launching Rx Inspector, a first-of-its-kind database that provides answers to what the FDA won’t tell us: where our generics are coming from and the track records of the factories that made them. The information is harder to find than you may think.
Labels on pill bottles often list a distributor or repackager rather than the actual manufacturer — and some have no information at all. When ProPublica asked our readers to send in photos of their pill bottles, they flooded our inbox with pictures proving just how difficult that information is to come by.
Even though generic drugs make up 90% of prescriptions dispensed in the U.S., the FDA only provides piecemeal information about them. It’s scattered across different websites with no easy way to link drugs to their manufacturers, factory locations and regulatory track records. Over many months, our journalists connected that data. In one case, ProPublica had to sue the FDA in federal court and received a partial list of factory locations.
You can use this app to connect your own medication to the manufacturer that made it, to the specific factory where it was made and to any FDA inspection reports and serious compliance violations linked to that facility that ProPublica has obtained.
For example, you can enter your drug name and any information on the label of your pill bottle about the company that may have made it. If you don’t have a company name, you can enter the color of your pills, or any markings on them, details that can lead you to information for your specific drug. From there, you can learn the name of the actual manufacturer (not the company that simply repackaged or distributed it). And you can also see the address for the factory that produced it.
If the factory has been inspected by the FDA, we’ll show you the inspection reports and any subsequent warning letters. We didn’t have access to every inspection report, so you may only see summary information that includes the dates of the inspections and any findings.
For pharmacists and others particularly knowledgeable about drugs, we’ve added an advanced search option so that you can enter key information, such as the National Drug Code, and quickly pull up manufacturing and regulatory details.
Finally, this app will allow you to learn more about individual drugmakers overall by providing a way to search for their factories. By entering a company name, you can see when those factories were last inspected and whether the FDA took any action in recent years.
Keep in mind that if you turn up a troubling inspection report, it doesn’t necessarily mean that your drug is compromised. Doctors and pharmacists advise that you not stop taking your medications. Instead, you should talk to your health care provider about any concerns.
ProPublica described the app and the methodology used to build it to the FDA, which did not comment. The agency previously told ProPublica that it doesn’t reveal where drugs are made on inspection reports to protect what it deemed confidential commercial information.
Our data is incomplete in places. The FDA, for example, hasn’t released all of its inspection reports. And though the agency provided ProPublica with a list of medications and the factories that made them, some locations were missing. We’ll add more details as they become available.
But this app provides the most detailed look yet at the makers of America’s generic drugs and whether they’ve met manufacturing standards meant to keep us safe.
Four Republican lawmakers have signed onto a Democratic-led discharge petition, which aims to force a vote on a bill that would restore tax credits for millions of Americans who receive health insurance through the Affordable Care Act (ACA). Those tax credits, initially instituted during the COVID-19 pandemic, allow for more people to access the program, insuring more Americans as a result.
As major anti-transgender bills loom and Congress prepares to vote on sweeping restrictions on transgender healthcare over the next two days, Representative Sarah McBride gathered with reporters outside the Capitol to denounce what she called the Republican Party’s “obsession” with transgender people. McBride was joined by Representatives Ocasio-Cortez and Johnson for the press scrum…
Dr. Kirk Moore had been on trial for five days, accused of falsifying COVID-19 vaccination cards and throwing away the government-supplied doses.
The Utah plastic surgeon faced up to 35 years in prison if the jury found him guilty on charges that included conspiracy to defraud the United States. Testimony had paused for the weekend when Moore’s lawyer called him early one Saturday this July with what felt to him like unbelievable news.
U.S. Attorney General Pam Bondi had ordered Utah prosecutors to drop all charges, abruptly ending his two-and-a-half year court battle.
“I just literally collapsed to the floor, and tears rolling down my face,” Moore recalled in a recent interview.
Bondi’s announcement marked a striking reversal of how the federal government handled the prosecution of COVID-19-related fraud under President Joe Biden. It has since emboldened other medical professionals who were similarly charged to consider seeking reexaminations of their cases. And it signaled the increasing clout of doctors and politicians who champion what they call “medical freedom,” which rejects modern public health interventions such as vaccine requirements in favor of individual choice.
Dismissed by the medical establishment, this movement has nevertheless built momentum as distrust in government and medical systems grew after the coronavirus pandemic. It has also gained new influence in Washington, where longtime vaccine critic Robert F. Kennedy Jr. oversees the nation’s health agencies. As President Donald Trump’s Health and Human Services secretary, Kennedy has replaced members of a federal vaccine advisory panel with his own picks and pushed the Centers for Disease Control and Prevention to restrict access to some vaccines, including the coronavirus shot. The Trump administration’s evisceration of long-standing federal vaccine guidelines and rejection of scientific evidence have alarmed the American Medical Association and other professional medical groups.
Just days before Bondi’s decision, a federal prosecutor from her department had stood before the jury in Moore’s case and accused him of enrolling in the federal government’s COVID-19 vaccine distribution program in order to “sabotage” it, according to a court transcript. She had asked jurors to convict him and to “find that no one is above the law, not even a plastic surgeon.”
Moore said he’d signed up for the program in May 2021 to receive more than 2,000 free vaccine doses and accompanying proof-of-vaccination cards after some businesses, nursing homes and the military began requiring such proof for visitors and employees. He said his plan was always to give vaccine cards without providing the shots because he wanted to offer patients a choice to circumvent vaccine mandates.
Bondi explained her decision to dismiss the charges on X later that morning, writing that “Dr. Moore gave his patients a choice when the federal government refused to do so. He did not deserve the years in prison he was facing. It ends today.”
A spokesperson for Bondi declined to comment beyond what the attorney general posted on social media. The Utah federal attorney’s office did not respond to requests for comment.
Moore was one of at least 12 health care professionals charged after giving or selling fraudulent COVID-19 vaccine cards since 2021, according to cases identified by The Salt Lake Tribune and ProPublica through government news releases and media clips. Those charged include midwives, nurses, pharmacists and another surgeon. Eight were charged in federal court by the Biden administration; prosecutors from California, New York and New Jersey brought state charges against four others.
Other than Moore, only one of these health care workers went to trial: a Chicago pharmacist whom a jury found guilty of selling on eBay blank vaccine cards that he had stolen from the Walgreens where he worked. The rest pleaded guilty and were sentenced to a mix of probation, home arrest and, in a few cases, prison. Many also were professionally disciplined with fines or suspension of their medical licenses.
Of those 11, the Chicago pharmacist appealed his conviction but the U.S. Supreme Court in November declined to hear his petition; his attorney told The Tribune and ProPublica that they are exploring a presidential pardon. One other health care worker said she, too, would like to be pardoned by Trump.
Some of these health care workers, along with those in other professions who were also convicted of vaccine card fraud, started a group called Covicted Patriot following the dismissal of Moore’s case.
“There are more of us than Dr. Moore,” they declared in July through an X account that bills itself as representing “Justified Felons & Persecuted Patriots who were victimized by a politically weaponized justice system for providing covid cards.”
“We celebrate his vindication as we pray for our own,” they wrote.
Moore said he supports their efforts: “I think anybody who took the same stance that I did, in large measures, should be pardoned.”
Brian Dean Abramson, an immunization law expert in Virginia who serves on the board of directors for the National Vaccine Law Conference, said that medical workers falsifying vaccination cards is “absolutely horrifying” from a public health perspective. Their actions, he said, fuel distrust of the medical profession and create blind spots in disease surveillance and response, increasing the likelihood and severity of outbreaks. (A simulation model published in JAMA in April predicts a reemergence of diseases that had been eliminated in the United States, such as measles, and accompanying deaths as a result of declining childhood vaccination.)
“This undermines every layer of the system that protects us from infectious disease,” Abramson said. “Vaccination policy relies on accurate records and honest medical participation.”
“Everybody Got What They Wanted”
Moore met with The Tribune and ProPublica in his clinic in the Salt Lake City suburb of Midvale. A neat row of clogs, his preferred footwear, lined one wall of his cluttered office. The 60-year-old physician wore black scrubs and a “Trump 2024” rubber bracelet stacked atop a gold chain.
Moore, a licensed physician in Utah since 2005, doesn’t deny the government’s claims: that he gave falsified vaccine cards to patients, that his staff threw away doses, and that, in some cases, he gave children saline shots instead of the COVID-19 vaccine at their parents’ request.
“All of that stuff is true,” he said.
Moore repeatedly referred to COVID-19 vaccines as “bioweapons” in an interview in his clinic in Midvale, a Salt Lake City suburb.Francisco Kjolseth/The Salt Lake Tribune
In an interview that lasted nearly two hours, Moore said choosing whether to get vaccinated is deeply personal and the decision should be made between patients and their doctors — not mandated by government or businesses. The Trump administration has similarly framed vaccination as a personal choice in its dismissal of established public health guidance.
Moore referred to COVID-19 vaccines as “bioweapons” a dozen times and said he distrusts how quickly the government facilitated the vaccines’ rapid development and distribution. He said he concluded the vaccines were unsafe after conducting his own online research that he said cast doubt on the medical technology used in their development and the amount of testing before the first doses became available under emergency use authorization in December 2020.
The COVID-19 vaccine was developed in record time during Trump’s first term, less than a year after federal authorities declared a public health emergency — a feat Trump touted at the time as a “monumental national achievement.” This was made possible by a federal effort known as Operation Warp Speed that reduced bureaucracy and invested in clinical trials and manufacturing, according to a 2021 report by the Government Accountability Office — not due to any shortcuts in testing. The technological backbone of the vaccines, known as mRNA, has been in development for decades by scientists who won the 2023 Nobel Prize in medicine.
Moore said that the vaccines “failed in every animal test.” “All the animals died, and now all of a sudden, we’re going to use the human population as our guinea pigs,” he said. The Food and Drug Administration has previously told reporters that such claims, widely promoted among vaccine skeptics during the pandemic, are false.
The plastic surgeon said that he believes all vaccines are “poison” and that they have not been adequately tested — a view he says he has held for more than two decades.
Vaccines approved by the FDA and recommended by the CDC have been proven to protect public health by preventing disease, serious illness or death. Major health authorities like the World Health Organization have affirmed the safety and efficacy of the COVID-19 vaccines, which researchers estimate prevented more than 14 million deaths worldwide in their first year.
Prior to signing up for the CDC’s vaccine distribution program, Moore did not provide vaccines in his business, the Plastic Surgery Institute of Utah. The “bread and butter” of his practice, he said, is a method of “rapid recovery” breast augmentations that he says he developed, which allows patients to return to their routines with little downtime.
“They were looking for anybody and everybody to get these bioweapons out,” he said about joining the government program, which was open to all health care providers who agreed to comply with the CDC processes, such as storing the vaccines at a certain temperature and recording who had been vaccinated. “And so, it was a pretty simple process.”
In December 2021, a husband-and-wife couple who Moore had met through a mutual acquaintance came to his home for dinner, according to a prosecution trial brief. “While they were there, Dr. Moore personally handed them both pre-completed CDC COVID-19 vaccination record cards with their names and birth dates on them, falsely purporting to show that the couple had received COVID-19 vaccines from the Plastic Surgery Institute,” the brief said. “Dr. Moore did so knowing that neither of them had been vaccinated for COVID-19, and without administering a COVID-19 vaccine to either of them.”
Within weeks, prosecutors said, Moore had started handing out fake vaccine cards in his medical office to anyone who was referred to his business by people who had already received a falsified card.
As word spread, Moore’s employees suggested patients who wanted a card could donate $50 via Venmo to a local health freedom advocacy group called the Health Independence Alliance, according to Moore. The husband of the couple to whom Moore first gave the fake vaccine cards testified at the Utah Legislature in January on behalf of the Health Independence Alliance on a vaccine-related bill. Moore says that he supports the group but does not run it; the Health Independence Alliance declined to comment in response to a request sent to the email listed on its website. The couple, who were not charged, declined to comment.
When sending their donation, patients were told to include an emoji of an orange in the Venmo subject line, according to federal prosecutors, and they were also instructed to bring an orange with them to the waiting room of the clinic. “At one point, there was a large basket full of oranges” at Moore’s clinic, prosecutors said in their trial brief.
In a trial brief, prosecutors included text messages showing the instructions patients were given to get a falsified vaccine card.Obtained by The Salt Lake Tribune and ProPublica
Moore confirmed this system in his interview with The Tribune and ProPublica, saying the piece of fruit was a quiet signal to his busy staff that the patient was there for a falsified vaccine card.
He said during this time he maintained his plastic surgery practice while distributing fake vaccine cards and treating COVID-19 patients with ivermectin and other methods. Ivermectin has not been authorized by the FDA or recommended by the CDC to treat COVID-19.
An undercover state licensor called Moore’s office in March 2022 and asked to make a vaccine appointment during the criminal investigation after someone complained to the state health department, according to the prosecutors. At his clinic, the licensor, posing as a patient, received a vaccine card attesting to her vaccination without ever being offered a shot, prosecutors said.
Federal prosecutors alleged in their trial brief that a portion of the donations for the advocacy group paid a part-time worker at the plastic surgery clinic $18 an hour to give out falsified vaccine cards and administer saline shots to children. The worker, who could not be reached for comment, testified against Moore as part of an agreement with prosecutors to dismiss her charges after the trial, according to prosecutors’ trial brief.
Moore said during an interview that he didn’t make any money himself and never directly charged patients for these cards. He added that every adult patient who got a fake card had wanted one.
“Nobody in my practice was ever tricked. Nobody came to me expecting a vaccine and didn’t get it,” he said. “Everybody got what they wanted.”
But some children who received saline shots at their parents’ request falsely believed they were being vaccinated against COVID-19, according to court filings and Moore. This was a breach of medical ethics because doctors have a duty to build trust between their community and the health care system, said Wendy Parmet, director of Northeastern University’s Center for Health Policy and Law.
Moore said he gave kids the saline shots so they wouldn’t be bullied if their peers found out they got a vaccine card without getting a shot. “I did have some parents that didn’t want their kid to know that they were getting something fake,” he said.
He didn’t question the parents’ deception, Moore said, because he didn’t want to “intervene in their family dynamic.”
“You have to stand up for what you feel is right,” he said. “That’s the reason why I did what I did. I had no intention of defrauding the federal government.”
Emboldening a Movement
On the first day of Moore’s trial in July, about 60 supporters — including state lawmakers like House Speaker Mike Schultz — gathered on the stairs outside the federal courthouse in Salt Lake City. They waved American flags and held signs protesting Moore’s charges at a busy intersection. The doctor tearfully thanked the crowd before walking into the courthouse where a jury would soon be selected.
Moore passed through a group of supporters on the steps of the federal courthouse in Salt Lake City during his trial in July.Rick Egan/The Salt Lake Tribune
The rally increased public and social media attention on Moore’s case, eventually reaching Georgia Rep. Marjorie Taylor Greene. She sent a letter to Bondi, urging the U.S. attorney general to drop Moore’s charges.
“Dr. Michael Kirk Moore deserves to be celebrated, not prosecuted, for his bravery in standing up to a system that prioritized control over public health,” Greene wrote in her July 12 letter. Her office did not respond to requests for comment. (Greene, an early supporter of Trump’s, recently announced her resignation from Congress after falling out of the president’s favor.)
That same day, Bondi ordered the charges be dropped and thanked Greene and Utah Sen. Mike Lee in posts on X for bringing the case to her attention. Lee’s office did not respond to questions about his role in the dismissal of Moore’s case.
Utah prosecutors then dismissed the charges against Moore, his business and a neighbor who prosecutors alleged had organized the donations to the health freedom advocacy group. Prosecutors also dropped charges against his office manager — who had pleaded guilty — and the part-time worker. Both of these employees testified against Moore and his neighbor the day before Bondi’s announcement. Neither the neighbor nor the office manager responded to requests for comment.
Less than a week after his charges were dropped, Moore and his fiancée flew to Washington, D.C., at Bondi’s invitation to meet with her and Greene; Moore said he asked if Lee could join them. Moore said the America First Policy Institute, a conservative think tank founded by former Trump administration officials, paid for his travel. (The group did not respond to a request for comment.)
Moore described the meeting as low-key and genuine: “It was a handshake and a hug to both M.T.G. and Attorney General Bondi.”
Moore, second from right, met with Utah Sen. Mike Lee, left, Georgia Rep. Marjorie Taylor Greene, center, and Attorney General Pam Bondi in Washington, D.C., after Bondi directed Utah prosecutors to drop federal charges against Moore.Courtesy of Kirk Moore
Moore estimates that he lost about two-thirds of his plastic surgery business after his 2023 indictment because he had used his marketing budget to cover his legal expenses. As he’s tried rebuilding his practice in recent months, he rebranded as Freedom Surgical & Aesthetics. He said he started thinking about a new name during the 22 days he spent in jail in November 2024 after a judge determined he had violated pretrial rules by communicating with other co-defendants.
The new name “stands for freedom and for people’s ability to choose,” he said. Images of the American flag and bald eagles appear on his clinic’s new website among photos of svelte women.
Moore’s medical license is in good standing. A state licensing division spokesperson would not say whether the agency is considering taking action against his license.
The lack of consequences for medical workers who falsify records could encourage others to undermine public health guidance, said Paul Offit, a pediatrician and vaccine expert at the University of Pennsylvania and Children’s Hospital of Philadelphia. Offit, who served on the CDC’s vaccine advisory panel from 1998 to 2003 and has clashed with Kennedy over vaccine policy, was kicked off a vaccine advisory committee for the FDA in August.
“The first two years of the pandemic turbocharged the medical freedom movement, which is a euphemism for basically saying that I don’t need experts. I will do my own Google searches and decide what’s right and what’s not,” Offit said. “Even if it goes against what is standard medical practice or medical wisdom, I’m going to decide for myself — and my neighbor be damned, in the case of vaccines.”
As Moore vows to “do everything I can to get COVID shots off the market,” others who faced similar legal battles say his turn of fortune has inspired them to fight their convictions.
Julie DeVuono, a former nurse in Long Island who also distributed fake vaccine cards to her patients, said she and two others created the CovictedPatriot X account after others who gave out fake cards reached out to her in response to her social media post celebrating Moore’s vindication.
New York state prosecutors had charged DeVuono with forgery and money laundering for using the proceeds from the fake vaccine cards to pay her mortgage. She pleaded guilty in 2023 and was sentenced to community service and probation. Her home was also seized as part of a $1.2 million forfeiture, and she lost her nursing license.
Kathleen Breault in her home in Cambridge, New York. The recently retired nurse says she expects to lose her professional licenses after issuing fake vaccine cards and is considering asking Trump for a pardon.Kate Warren for ProPublica
“Is there any chance for us to get some kind of restored justice?” she said in an interview.
DeVuono, 53, said she feels she and others who were convicted of similar crimes were treated unfairly, but she can’t ask for a presidential pardon because her charges were filed in state court. Instead, she’s advocating on behalf of others who can beseech Trump, such as Kathleen Breault, a recently retired midwife and nurse in New York.
Breault faced a possible five-year prison sentence after she and a co-defendant were indicted in federal court in 2023 for destroying thousands of vaccines and issuing falsified vaccine cards.
“I was terrified,” Breault, 68, told The Tribune and ProPublica. “But I also felt defiant, because I felt like what I did was right.”
She said if she had gone to trial, her defense would have been civil disobedience. But Breault has health issues and cares for her grandchildren. She said her children urged her to do whatever she needed to in order to avoid a prison sentence.
So she pleaded guilty to conspiring to defraud the United States — a felony — and was sentenced last December to three years probation. (Her co-defendant, who died in March, had also pleaded guilty.)
Breault said she was buoyed by news over the summer that similar charges against Moore were dropped at the behest of the Trump administration. The outcome of Moore’s case has motivated her to begin the process of asking for a presidential pardon.
A White House spokesperson did not respond to a request for comment about whether Trump has received any pardon requests from health care workers indicted in connection with the pandemic or if he would pardon them. He has not pardoned anyone in that situation, according to a review of the clemency grants in his second term listed on the Department of Justice’s website.
Breault said she’d like to have her conviction erased so she’s not limited by her felon status. She’d like to own a gun again, but those with felony convictions are prohibited from possessing firearms in New York. She’d also like more freedom, including not having to report to her probation officer when she travels or how much is in her bank account.
“After seeing what happened with Kirk,” she said about Moore, “maybe if I didn’t take the plea, I wouldn’t have a felony conviction now.”
New polling finds that a comfortable majority of Republicans say they would rather the U.S. fund health care programs at home than continue to send billions to Israel, in the latest show of the increasing divide between the public and U.S. political leaders on Israel policy. Polling conducted last month asked whether or not Republican voters believe that the U.S. should give Israel funding…
This story originally appeared in Common Dreams on Dec. 16, 2025.It is shared here under a Creative Commons (CC BY-NC-ND 3.0) license.
During his first term, after repeatedly promising the country a terrific healthcare plan, Donald Trump famously commented, “Nobody knew that healthcare could be so complicated.” In fact, everyone who spent even a few minutes looking at the issue knew that healthcare was complicated. That is why Obamacare ended up being a hodgepodge that was pasted together to extend healthcare coverage as widely as possible. It is also the reason Trump and the Republicans never produced a healthcare plan in Trump’s first term.
The basic problem is that healthcare costs are hugely skewed. Ten percent of the population accounts for more than 60% of total spending, and just 1% accounts for 20% of spending. Most people have relatively low healthcare costs. The trick with healthcare is paying for small number of people who do have high costs.
Individual Choice, Cherry-Picking the Pool, and Screwing Cancer Survivors
The Republicans in Congress, along with Trump on alternate days, are pushing plans that are supposed to give choice to individuals and somehow take it away from insurers. It’s not clear what they think they are saying. They seem to still envision that people will buy insurance, as they do now in the Obamacare exchanges, but somehow that they will have more control in the Republican option.
There is one story they could envision, which would make it much easier for insurers to skew their pool. The Affordable Care Act (ACA) restricted what sort of plans could be offered in the exchanges in order to limit the ability for insurers to avoid high-cost individuals.
It would be possible to relax these restrictions to allow insurers to cherry pick their enrollees. For example, they could offer high-deductible plans, say $15,000 in payments, before any coverage kicked in.
The Republican healthcare plan is a rerun of the bluff and lie strategy they have been doing for more than 15 years.
No person with a serious health condition would buy this sort of plan since they know they would be paying at least $15,000 a year in medical expenses, and then a substantial fraction of everything above this amount, in addition to the premium itself. On the other hand, a low-cost plan with $15,000 deductible might look pretty good to someone in good health, whose medical expenses usually don’t run beyond the cost of annual checkup.
The Republicans can look like the great promoters of individual choice by allowing insurers to market these high-deductible plans. The problem is that healthy people will all gravitate to high-deductible plans, leaving only the people with serious health issues—the 10%—to buy plans with more modest deductibles.
These plans will then be ridiculously expensive since insurers are not going to insure people at a loss. If they have a pool with four or five times the average per person healthcare costs, they will charge a premium that is four five times the average cost, plus a margin for administrative costs and profits. This means that cancer survivors, people with heart disease, and other serious health conditions will be screwed, given the option of ridiculously expensive insurance or none at all.
Been There, Done That
The most painful part of this story is that we have all been around the block many times on this story. Unless Trump and the Republicans are extremely ignorant, which can never be ruled out, they are simply lying and hope that the media will let them get away with it. They have no brilliant plan to lower healthcare costs. They are simply proposing a scheme that will lower premiums for healthy people by screwing the ones who need healthcare most.
It amounts to lowering costs by not providing care. It’s like reducing the cost of food by not letting people eat. But if the point of a healthcare system is to provide people with the healthcare they need, the Republican proposals are nonstarters.
As a practical matter, contrary to what the Republicans and the media say, healthcare cost growth did slow sharply after Obamacare passed. That may not have been entirely due to Obamacare, but that is the reality. Too bad the Democratic consultants tell Democratic politicians not to talk about it.
The Real Source of High Costs
We do pay way too much for healthcare in the United States, but it is not because of Obamacare. We pay twice as much for our drugs, medical equipment, and doctors as people in other wealthy countries. These high payments persist because they are supported by powerful lobbies.
Some of us had hope that the Trump administration might take some steps to reduce these prices, especially in the case of drugs, since RFK, Jr. had railed against corruption in the pharmaceutical industry. Unfortunately, his tirades were limited to an evidence-free crusade against long-proven vaccines, which are not even a major source of profit for the industry.
Donald Trump talked about reducing drug prices 1,500% (really), but this mostly amounted to getting his name on a drug discount website for a small group of patients. We were spending 6.4% more on drugs in September of this year than in the same month in 2024. (September is the most recent month for which data are available.)
Trump has shown no interest in doing anything to lower the cost of medical equipment. And he has said nothing about lowering doctors’ fees, although some reshuffling of the Medicare reimbursement schedules may reduce overpayments to specialists and better pay for family practitioners. His immigration policies are going the wrong way here, making it even more difficult for foreign-trained medical students and doctors to practice here.
And there are the insurers themselves, which gobble up close to 25% of the money they pay out to providers in the form of administrative costs and profits. A recent study found that If we add in the cost imposed by insurers on hospitals, doctors’ offices, and other providers, they take up close to a third of healthcare expenses.
Trump has shown no interest in reining in the insurance industry apart from his silly talking point about giving people money directly to… wait, wait, buy their own unregulated insurance. That will do nothing to reduce the money flowing into the industry’s pockets.
The Republican healthcare plan is a rerun of the bluff and lie strategy they have been doing for more than 15 years. Given the right-wing control of much of the media, it could work for them politically. The tragic part of the story is that millions could end up without the healthcare they need.
When Dr. Ed Paul visits Nogales, Arizona, he sees well-trained, hardworking doctors and nurses. Yet as in many smaller towns and rural communities, its health care staffing, infrastructure, and funding doesn’t meet the needs of residents.
People who need health care have a tough time accessing it — and the people delivering it feel overburdened. With limited providers, Dr. Paul notes, it’s hard to get an appointment, so patients either wait, travel long distances, or simply go without.
As the Policy Director for the Rural Democracy Initiative, I support groups across the country who are working to ensure rural Americans have access to quality, affordable health care.
Sarah Monroe once had a relatively comfortable middle-class life. She and her family lived in a neatly landscaped neighborhood near Cleveland. They had a six-figure income and health insurance. Then, four years ago, when Monroe was pregnant with twin girls, something started to feel off. “I kept having to come into the emergency room for fainting and other symptoms,” recalled Monroe, 43…
Around 150 participants filled both sides of the entrance road to State Correctional Institution (SCI) Mahanoy for a rally on Dec. 9 – the final day of the historic March for Mumia. The march demanded “Justice for Mumia Abu-Jamal, End Medical Neglect [in Pennsylvania prisons] and End Elder Abuse.”
The 12-day, 103-mile march started in Philadelphia on Nov. 28 and ended in Frackville, Pennsylvania, with over 65 people walking the last three miles. A long-time supporter of Mumia, Pam Africa, with International Concerned Family and Friends of Mumia Abu-Jamal, reminded people that Mumia was a journalist, a teacher, and a family man, who was railroaded and never had a fair trial. She urged people to keep on fighting for justice for Mumia.
This fall, Americans got to see what it’s like to go without a safety net for the hungry. With the U.S. government shut down for multiple weeks and President Donald Trump refusing to fund SNAP, the federal food stamp program, a panic set in among the more than 40 million people who rely on it. Families skipped meals, and babies went unfed. Food banks ran out of food, and some people turned to dumpster diving.
It was just a glimpse of what’s to come. Starting next October, Trump’s so-called One Big Beautiful Bill Act will shift billions in SNAP costs from the federal government onto states.