As the anti-transgender panic continues to escalate — and as many of the bills seen over the last four years migrate from statehouses to the national level — states that have led the charge have shown no inclination to slow down. Instead of resting on the discrimination they have already enacted, many are pressing forward with new and increasingly punitive ways to target transgender people.
The Food and Drug Administration rarely uses its authority to pull dangerous medical devices off the market and is so poorly staffed that it’s sometimes unable to make sure companies are taking critical steps to protect patients during health emergencies, according to a new report by the Government Accountability Office.
The inquiry by the congressional watchdog was requested nearly two years ago by top members of the Senate in the wake of an investigation about the 2021 recall of breathing machines that threatened the health of millions of Americans.
ProPublica and the Pittsburgh Post-Gazette revealed that the FDA had received hundreds of complaints over many years about the machines and never ordered a recall. Philips Respironics eventually recalled the devices, which were fitted with an industrial foam that could break down and release toxic material into the lungs of patients, including the elderly, veterans and infants.
Philips had fielded thousands more complaints before initiating a recall and didn’t notify FDA, the news organizations found. Customers who relied on the continuous positive airway pressure, or CPAP, machines and other devices reported respiratory illnesses, kidney and liver conditions, and cancer.
In 2023, U.S. Sens. Dick Durbin, D-Ill., and Richard Blumenthal, D-Conn., urged the GAO to investigate the agency’s practices amid one of the most tumultuous medical device recalls in recent history.
In a statement, Durbin called the GAO report “long overdue,” saying it details “the harms caused by drastic staffing cuts” and “how weakened enforcement authority has made it even more difficult for FDA to carry out critical oversight activities.”
The probe, which began last year, found the FDA doesn’t use its authority to force manufacturers to pull defective devices from the market. The agency has been empowered under federal law for decades to take such action, but it has only done so four times, the last in 1992.
In the vast number of cases, device makers voluntarily initiated recalls — about 900 in each of the past five years, the GAO said.
Even when companies start the process, FDA staff — which has weathered significant cuts under the Trump administration — can’t always properly ensure that there are no delays or missteps in removing defective devices and communicating with consumers, the report said.
The agency currently regulates more than 190,000 medical devices in the United States, an increase of about 15,000 since 2016, according to the GAO.
“FDA needs additional resources and staff to adequately protect Americans from unsafe medical devices,” Blumenthal said in a statement. “Current and future staffing cuts at FDA will only further undermine the agency’s ability to protect people from unnecessary harm.”
The investigation by ProPublica and the Post-Gazette found some patients didn’t learn about the 2021 recall of their breathing machines for months or years and continued to use them even as company tests showed that foam in the machines were releasing dangerous compounds.
Dr. Rita Redberg, a cardiologist and expert on medical device safety, called the FDA’s recall notification system “primitive by today’s standards” and said improvements have been badly needed for years.
“I mean, recall notices are still faxed because the FDA lacks a modern comprehensive data infrastructure for recalls,” she said. “It’s really shocking.”
One former FDA official said he fears the agency’s handling of recalls could become less efficient in the wake of recent staffing cuts. FDA employees told the GAO they often can’t carry out basic tasks, such as reading status reports submitted by companies while recalls are underway. Those reports detail how many people have been notified about defective devices, the number of products fixed and the estimated time frame to complete the recall.
“I would be worried that the circumstances at FDA are now even worse than portrayed in the report,” said Dr. Peter Lurie, a former FDA associate commissioner who left the agency in 2017.
In response to the GAO’s findings, the Department of Health and Human Services, which oversees the FDA, said it would assess the need for additional staff and greater legislative authority to better manage recalls. The FDA previously defended its handling of the Philips recall, saying it acted as soon as it learned of safety concerns.
Philips, which manufactured the devices at two plants outside Pittsburgh, has said the original foam caused “no appreciable harm” to patients. Last year, the company reached an agreement with the Justice Department, promising to hire an independent safety monitor and undergo regular facility inspections.
The company also agreed to pay more than $1 billion to settle lawsuits filed by thousands of people who say they were injured by the devices. Under the terms of the settlement, Philips did not admit fault or liability.
This week, Durbin and Rep. Jan Schakowsky, D-Ill., introduced legislation that would require the FDA to address some of the GAO’s most pressing concerns.
The bill, among other things, would require the FDA to establish an electronic format for recall alerts so that critical information can more easily be shared between companies, the FDA, hospitals and doctors.
“Millions of Americans rely on a medical device to stay healthy,” Durbin said. “But if their medical device is recalled, patients have the right to know as soon as possible so that they can understand the risks.”
A federal court in Philadelphia ruled in favor of Children’s Hospital of Philadelphia blocking the Trump administration’s demand for the renowned hospital’s Gender and Sexuality Development Program to turn over confidential information about clinic patients. CHOP runs one of the largest clinics in the U.S. which provides medical care and mental health support for transgender and gender-nonbinary children and teens and their families. Each year since 2014, hundreds of new families seek care through the program.
For years, Sen. Ron Johnson has been spreading conspiracy theories and misinformation about COVID-19 and the safety of vaccines.
He’s promoted disproven treatments for COVID-19 and claimed, without evidence, that athletes are “dropping dead on the field” after getting the COVID-19 vaccination. Now the Wisconsin politician is endorsing a book by a discredited doctor promoting an unproven and dangerous treatment for autism and a host of ailments: chlorine dioxide, a chemical used for disinfecting and bleaching.
Kory has said there’s a globally coordinated campaign by public health agencies, the drug industry and the media to suppress evidence of the medicinal wonders of chlorine dioxide. His book, according to its website, contends that the “remarkable molecule” works “to treat everything from cancer and malaria to autism and COVID.”
The book jacket features a prominent blurb from Johnson calling the doctor’s treatise: “A gripping tale of corruption and courage that will open eyes and prompt serious questions.”
Chlorine dioxide is a chemical compound that has a range of applications, including as a disinfectant and deodorizer. Food processing plants apply it to sanitize surfaces and equipment. Hospitals use it to sterilize medical devices, and some municipalities use low levels to treat public water supplies. Paper mills rely on it to whiten wood pulp. Safety experts advise those who handle it to work in well-ventilated spaces and to wear protective gloves.
Concentrations in drinking water systems higher than 0.8 milligrams per liter can be harmful, especially to infants, young children and fetuses, according to the Environmental Protection Agency.
Still, for many years people in online discussion groups have been promoting the use of chlorine dioxide in a mixture that they call a “miracle mineral solution,” ingested to rid people of a host of maladies. The Food and Drug Administration has warned that drinking these chlorine dioxide mixtures can cause injury and even death.
It is not medicinal, despite Kory’s contention. “It is all lunacy. Absolutely, it’s 100% nonsense,” said Joe Schwarcz, director of McGill University’s Office for Science and Society in Montreal and an expert on the threat of pseudoscience. Schwarcz has written articles about the so-called miracle mineral solution, calling it “a poison” when it’s in high concentrations.
The cover of the paperback version of “The War on Chlorine Dioxide” features a quote from Sen. Ron Johnson.Bella Luna Press
Kory’s book, set to be released to the public in January, argues that word of chlorine dioxide’s effectiveness has been suppressed by government and medical forces that need people to remain perpetually ill to generate large profits. The use of the word “war” in the title is fitting, Kory said in a recent online video on his co-author’s Substack. “In the book I detail many, many assassination attempts of doctors who try to bring out knowledge around chlorine dioxide,” he said.
Johnson confirmed to ProPublica in an email that he authorized the statement on the cover. “After reading the entire book, yes I provided and approved that blurb,” he said. “Have you read the book?”
ProPublica asked Kory and his co-author, Jenna McCarthy, to provide an advance copy, an interview and responses to written questions. Kory did not respond. McCarthy wrote in an email to ProPublica that she was addressing some of the questions on her Substack. (She did not send a book or agree to an interview.)
The book “is a comprehensive examination of the existing evidence and a plea for open-minded inquiry and rigorous research,” she wrote on Substack. She dismissed warnings about chlorine dioxide’s toxicity in high concentrations, writing: “Everything has a toxic dose — including nutmeg, spinach, and tap water.”
She said that chlorine dioxide is being studied in controlled settings by researchers in the United States and Latin America and that “the real debate is how it should be used, at what dose, and in which clinical contexts.”
Johnson did not agree to an interview and did not answer questions emailed to his office by ProPublica, including whether he views chlorine dioxide as a world-changing medical treatment and whether he believes the FDA warnings are false.
“It’s Called Snake Oil”
Johnson has been an advocate of Kory’s for years, calling the doctor as an expert witness in two 2020 Senate hearings. In one, Kory championed taking the drug ivermectin, an antiparasite medicine, to treat COVID-19.
In 2021, an analysis of data from clinical trials concluded that ivermectin could reduce deaths from COVID-19 and may produce other positive effects. McCarthy cited that analysis in her Substack response.
In 2022, however, the American Journal of Therapeutics, which had published the study, warned that suspicious data “appears to invalidate the findings” regarding ivermectin’s potential to decrease deaths.
Later clinical trials have found no beneficial effect of ivermectin for COVID-19, and the FDA has warned that taking large doses can be dangerous. The drug’s manufacturer has said it hadn’t found any scientific basis for the idea that ivermectin can effectively treat COVID-19. Kory, though, continued advocating for ivermectin.
In 2024 the American Board of Internal Medicine, which credentials physicians in certain specialties, revoked Kory’s certifications in internal medicine, pulmonary disease and critical care for making false and misleading public statements about the ability of ivermectin to treat COVID-19. Hospitals and many insurance networks typically require doctors to be board certified.
Kory vigorously fought the disciplinary action, arguing to the ABIM that he provided substantial medical and scientific evidence to support his recommendations for addressing COVID-19, though not the “consensus-driven” approach. He also sued the board in federal court, citing his free speech rights in a case that is still progressing in the 5th U.S. Circuit Court of Appeals. On Substack, McCarthy excoriated the ABIM, saying it “bullies physicians” and “enforces ideological conformity.”
In 2022, Johnson and Kory penned a Fox News op-ed opposing a California bill that would strip doctors’ licenses for espousing misinformation about COVID-19. The bill became law but was repealed after a court fight. A federal judge found the statute’s definition of misinformation to be too vague, which could infringe on doctors’ right to free speech.
Johnson, who has been in Congress since 2011, has a history of advocating for experimental treatments and viewing the government as an impediment. Dr. Peter Lurie, president and executive director of the Center for Science in the Public Interest, a public health advocacy group, said that among members of Congress, Johnson was “an early adopter of anti-science ideas.”
Lurie said that Johnson is no longer an outlier in Washington, which now has many more elected lawmakers whom he considers anti-science. “What may have started off as the cutting edge of an anti-science movement has now turned into a much more broader-based movement that is supported by millions of people,” he said.
Earlier this year, Johnson held a hearing highlighting a flawed study claiming that vaccinated children had an increased rate of serious chronic diseases when compared to children who were not vaccinated. The conclusion questions the scientific consensus that vaccines are safe. The study’s researchers chose not to publish it because of problems they found in their data and methodology.
HHS did not respond to requests from ProPublica about Kennedy’s views on chlorine dioxide. At his confirmation hearing, Kennedy praised President Donald Trump for his wide search for a COVID-19 remedy in his first term, which Kennedy said included vaccines, various drugs, “even chlorine dioxide.”
Kory’s publisher is listed as Bella Luna Press, which has issued at least two other titles by McCarthy. “Thanks to the Censorship Industrial Complex, you won’t find The War on Chlorine Dioxide on Amazon or at Barnes & Noble. We had to design and build this website, figure out formatting and printing and shipping, and manage every aspect of order processing ourselves,” the book’s website states. (A representative for Bella Luna could not be reached for comment.)
As this new book is released, the autism community is also grappling with another controversy: the unsubstantiated assertion by Kennedy that Tylenol use by pregnant women poses an increased risk of autism. In addition, under Kennedy, the Centers for Disease Control and Prevention revised its website in November to cast doubt on the long-held scientific conclusion that childhood vaccines do not cause autism.
Some parents of children with autism, desperate for a remedy, have long reached for dubious and at times dangerous panaceas, including hyperbaric oxygen chambers and chelation therapy, used for the treatment of heavy metal poisoning. Neither method has been proven effective.
Helen Tager-Flusberg, director of the Center for Autism Research Excellence at Boston University, said Johnson has “acted extremely irresponsibly” in lending his name to a book making claims about chlorine dioxide treating autism.
“Wisconsin is filled with experts — clinical experts, medical experts, scientists — who understand and have studied autism and treatments for autism for many many years,” she said. “He’s chosen to completely ignore the clinical and the scientific community.”
People with autism may take medication to reduce anxiety, address attention problems, or reduce severe irritability. Many benefit from behavioral interventions and special education services to help with learning and functional abilities. But there is no cure, said Tager-Flusberg.
Referring to chlorine dioxide, she said: “We have had examples of this probably throughout the history of medicine. There’s a word for this, it’s called snake oil.”
In her response on Substack to ProPublica, McCarthy wrote that “chlorine dioxide is being used to treat (nobody said ‘cure’) autism with life-changing results.”
The Search for Miracle Cures
The mother of an autistic son, Melissa Eaton of North Carolina, heard Kory reference his book in early November on The HighWire, an internet talk show hosted by Del Bigtree, a prominent vaccine skeptic and former communications director for Kennedy’s 2024 presidential campaign. She then looked up the book online and noticed Johnson’s endorsement.
Eaton for many years has worked to expose people who peddle chlorine dioxide and to report apparent injuries to authorities. She monitors social media forums where parents discuss giving it to their children orally or via enemas. Sometimes the families reveal that their children are sick. “They’re throwing up and vomiting and having diarrhea and rashes,” Eaton said.
Some adherents advise parents that the disturbing effects indicate that the treatment is working, ridding the body of impurities, or that the parents should alter the dosage.
“Most of these kids are nonverbal,” Eaton said. “They’re not able to say what’s hurting them or what’s happening to them. The parents feel they’re doing the right thing. That’s how they view this: They’re helping to cure autism.”
The idea that chlorine dioxide can be a miracle cure began to spread about 20 years ago when a gold prospector, Jim Humble, wrote a book claiming his team in Guyana fell ill with malaria and recovered after drinking safe amounts of chlorine dioxide.
Humble later co-founded a “health and healing” church in Florida with a man named Mark Grenon, who called himself an archbishop and sold a chlorine dioxide solution as a cure for COVID-19. They described it as a “miracle mineral solution,” or MMS.
Grenon went to prison in 2023 for conspiring to defraud the United States by distributing an unapproved and misbranded drug. The scheme took in more than $1 million, according to prosecutors.
An affidavit in the case filed by a special agent with the FDA Office of Criminal Investigations noted: “FDA has received numerous reports of adverse reactions to MMS. These adverse reactions include hospitalizations, life-threatening conditions, and death.”
Grenon, who is now out of prison, told ProPublica that he too is writing a book about chlorine dioxide. “My book will tell the truth.” He declined further comment.
Chlorine dioxide is currently used in many ways that are not harmful. It is found in some consumer products like mouthwashes, but it is not meant to be swallowed in those instances. (One popular mouthwash warns to “keep out of reach of children.”) It’s also available to consumers in do-it-yourself packages where they combine drops from two bottles of different compounds — commonly sodium chlorite and hydrochloric acid — and add it to water. Hikers often carry the drops, or tablets, using small amounts to make quarts of fresh water potable.
But numerous online shoppers post product reviews that go further, referring to it as a tonic. Various online guides, some aimed at parents of autistic children, recommend a shot-glass-size dose, sometimes given multiple times a day and even hourly. That can far exceed the threshold the EPA considers safe.
McCarthy, addressing ProPublica on Substack, wrote: “You point to various online guides that offer what could be considered dangerous dosing instructions. We agree, the internet is a terrifying wasteland of misinformation and disinformation.”
In the Substack video, Kory said he felt compelled to spread the word about chlorine dioxide much as he did about ivermectin, even though it cost him professionally.
He no longer has a valid medical license in Wisconsin or California, where he did not renew them, according to the Substack post. His medical licenses in New York and Michigan are active.
“I like to say I was excommunicated from the church of the medical establishment,” he said in the Substack video. As a result, he said, he turned to telehealth and started a practice.
In the Nov. 6 HighWire episode hosted by Bigtree, the discussion included talk not just of chlorine dioxide’s medicinal potential but also of how cheap and easy it is to obtain.
“On Amazon, it’s literally, you get two bottles, well, it comes in two,” Kory started to explain, before stopping that train of thought.
Senator Elizabeth Warren (D-Mass) is set to reintroduce the Corporate Crimes in Health Care Act — legislation that authorizes criminal and civil penalties for private equity owners of healthcare organizations when their actions cause the injury or death of patients under their care. It is the toughest legislation to date designed to curb the worst excesses of Wall Street owners in healthcare.
Supporters of Mumia Abu-Jamal are on a 103-mile, 12-day march ending Tuesday in Frackville, Pennsylvania, where he is imprisoned at the Mahanoy state prison. The march ends on the same day Abu-Jamal was arrested in 1981 for the murder of Philadelphia police officer Daniel Faulkner, for which he has always maintained his innocence. One of the best-known political prisoners in the world…
This past June, Ashley Voss-Barnes received a court summons in the mail.
PrairieStar Health Center, a nonprofit community health center in south-central Kansas, was suing her for $675 and her wife for $732 in unpaid medical bills. Voss-Barnes knew the clinic received federal funding to make preventive health care accessible in a region where many families, including her own, needed financial help.
She didn’t understand what led to the lawsuit. She and her wife had a blended family of five kids that cost a lot to keep healthy. As a result, years ago, the couple had asked PrairieStar if they could set up an ongoing payment plan to automatically take money from their checking accounts multiple times a month. Voss-Barnes would later state in a court filing that PrairieStar never informed her those payments were not enough to cover her bills and keep her out of collections.
“If I have something due, then I will try to pay it,” she said to ProPublica. “It came out of nowhere.”
Voss-Barnes, a nurse who feels confident navigating the health care system, wanted to push back. She reached out to a local lawyer to see if he could represent them, but he said the debt was too small to be worth it. So she represented herself, filing a letter in court objecting to the lawsuit and asking to continue the existing payment plan.
Eventually, Voss-Barnes and her wife agreed to set up new payment plans with the collections agency for the debt, to avoid having the money taken directly from their paychecks through wage garnishment. To their dismay, they owed hundreds more in interest, court costs and lawyer fees as a result of PrairieStar’s decision to sue.
They worry about PrairieStar suing them again. “I know we’re not the only ones this has happened to,” Voss-Barnes said.
The lawsuits against the two women are among at least 1,000 that PrairieStar has filed against patients since 2020 for unpaid medical bills, according to a ProPublica analysis of state court records over that period. Many patients PrairieStar sued were uninsured and made so little money they qualified for discounted care, a former patient accounts employee told ProPublica.
Community health centers like PrairieStar Health, also known as federally qualified health centers, were created to serve as medical safety nets for people who struggle to afford primary care. They were established during the Civil Rights Movement-era “War on Poverty,” when federal officials realized that low-income Americans, overwhelmed by long drives and crowded hospitals, were forgoing medical attention. The health centers receive federal grants in exchange for serving patients regardless of their ability to pay, increasing access across large swaths of the country.
But ProPublica found that several of these health centers are suing patients and garnishing their paychecks — which experts say contradicts their mission. We identified two other centers in Kansas, plus one in rural Virginia and one in Kalamazoo, Michigan, that consistently filed lawsuits against patients since at least 2020. Our search, which was not exhaustive, focused on states and counties where court records are publicly accessible online. We also reviewed documents from a municipality in Alaska and a county in California that run community health centers, which showed they use outside debt collectors to pursue what patients owe.
Leaders of five community health centers, including PrairieStar, told ProPublica they send patients to collections or file lawsuits against them as a last resort, after sending statements and offering payment plans. Three pointed to the financial instability that community health centers face as a reason to pursue patient debt. All five stressed that they did not turn away patients who could not afford medical care, citing a goal to make health care accessible.
In response to questions from ProPublica, PrairieStar CEO Bryant Anderson said that the health center faces “a perfect storm” caring for patients while also dealing with higher costs and unstable funding. “With all the challenges PrairieStar faces to maintain access to care for the uninsured and the underinsured, having someone imply that we don’t fulfill our mission is certainly rubbing salt in the wounds,” he wrote in an email.
Anderson said PrairieStar generally tries six times to communicate with patients before sending them to collections. He also said every patient is given the option to apply for sliding-scale discounts based on income and about a third choose not to provide that information.
Other health center leaders also explained their decision to pursue patient debt through lawsuits, in response to questions from ProPublica. “We understand that sending accounts to collections can seem at odds with that mission, and it’s not a decision we take lightly,” said Renee Hively, the CEO of CareArc, a community health center in Kansas. CareArc has appeared in local news for pursuing one patient’s medical bill through a lawsuit and wage garnishments for more than 12 years, contributing to her being unable to afford basic utilities. (CareArc did not respond to a request for comment about that particular case.)
A spokesperson for the department that oversees community health centers in Monterey County, California, told ProPublica that most unpaid bills it sends to collections “involve small amounts that do not justify the cost of initiating legal proceedings.” As a result, none of its patients have been sued since 2019. If the health centers ever stopped sending patients to collections, the spokesperson said, the financial effect would be “minimal.”
Most of the public attention on medical debt and related lawsuits has been focused on hospitals, especially nonprofit hospitals that receive tax breaks in order to make care more affordable. Hospitals must provide emergency care regardless of whether the patient can afford it but are not required to provide primary care like checkups or routine screenings. Nonprofit hospitals are required by federal law to check whether patients qualify for financial help before suing them or garnishing their wages.
Community health centers, on the other hand, must make “every reasonable effort” to collect money from patients before writing it off, according to federal law.
Though experts and leaders of other health centers say the centers have ample freedom to decide what “reasonable” means — and whether to pursue debt through collections agencies and the courts — Anderson said the manner in which PrairieStar collects debts is mandated by the law.
He also said that ProPublica may be trying to “induce” other health centers to violate federal law by reporting and writing this story. “Your messaging would therefore be dangerous and intimate that such health centers were not required to make ‘every reasonable effort to secure payments’ for their services,” he wrote.
But experts on community health center finances said that federal law does not require the centers to send patients to collections. “There’s no law that says you have to garnish wages or that you have to go after someone through collections,” said Ray Jorgensen, a health care billing consultant who said he has worked with hundreds of community health centers over about 30 years. “I would say that’s an anomaly. That’s not the norm.”
Anderson did not answer specific questions about PrairieStar’s lawsuits or wage garnishments. He repeatedly said that ProPublica did “not have all the facts” and that the story would be “potentially defamatory,” but he did not clarify what he felt was missing or inaccurate. Nor did he respond directly to questions about Voss-Barnes’ experience, even though she and her wife signed privacy waivers allowing him to do so. Voss-Barnes said that he reached out to her directly, telling her that everyone in their Kansas city would know that she had failed to pay her medical bills if she moved forward with the article. (He did not respond when asked about that outreach.) He did tell ProPublica that he personally contacted both a former employee and another patient who ProPublica had asked him about. The patient stopped responding to ProPublica.
Medical debt experts said they were surprised and horrified to hear that community health centers were using lawsuits and third-party debt collectors to recover money from patients, given their intended purpose of providing care to people who have no other options. Under federal law, community health centers must provide discounted care on a sliding scale for patients who make at or below 200% of the federal poverty guideline, an amount that varies based on family size and household income. A family of four must make under $64,300 to receive a discount. Medical debt disproportionately burdens Black, Hispanic, low-income and uninsured patients — groups more likely to use community health centers for affordable care.
“Patients who have been sued because of medical debt are likely to avoid care in the future,” said Miriam Straus, policy adviser for Community Catalyst, a health advocacy group. “These collection activities seem to violate at least the spirit of the requirement to provide health services available to all.”
On Virginia’s Eastern Shore, a narrow peninsula bordered by the Atlantic and the Chesapeake Bay, getting sued by the community health care center is a regular occurrence. Over the last decade, Eastern Shore Rural Health filed more than 7,000 lawsuits for unpaid medical bills in two counties where 45,000 people live.
It sued one couple for $59 in January 2024, an amount that ballooned by more than 600% within months due to interest, court costs and lawyer fees. Court records show money regularly garnished from people working in the low-wage industries that abound on the Eastern Shore, including poultry processing and retail.
On an August morning in Accomack County’s civil court, Eastern Shore Rural Health accounted for most of the cases on the judge’s docket. One man who showed up to court told ProPublica that the visit potentially cost him hundreds of dollars because he missed out on lucrative hours harvesting oysters and clams. He only spoke Spanish and the court did not make a translator available; the judge told him to return for another hearing in the fall. Most people didn’t show up to court at all, meaning the health center won by default.
ProPublica did not find any other community health centers in Virginia consistently suing patients for unpaid bills in the court records.
Eastern Shore Rural Health began using lawsuits to collect medical debt about 20 years ago after conversations about “maximizing our revenue,” according to Kandy Bruno, the organization’s chief financial officer. A local company called Bay Area Receivables handles its collections and takes 30% to 40% of what it recovers from patients through the court. The minimum amount that Eastern Shore sends to collections is $25, Bruno said.
Bruno said Eastern Shore sends patients to collections when it has exhausted other options, including sending out letters, offering interest-fee payment plans and helping fill out Medicaid applications. “We should never have to send anyone to collections,” she said. “It should be 100% avoidable.” She also said the number of lawsuits the company had filed in a decade was not very high compared to the 32,400 patients seen there last year.
Patients are never refused health care, no matter how much they owe, she said.
Virginia recently passed a law that experts say would stop at least some of Eastern Shore Rural Health’s debt collection practices starting next summer. The law prohibits large medical providers from garnishing wages of patients who qualify for financial assistance.
Bruno said she hasn’t yet looked into how the Virginia law would affect the health center or its patients on the sliding scale. “We will absolutely comply with and make adjustments to comply with the letter of the new law,” she said.
The health center is the main option for preventive care on the peninsula; otherwise, people have to make the long drive up to Maryland or pay tolls, often totaling more than $20, to cross the bridge over the Chesapeake Bay. More than 70% of people who live on the Eastern Shore see doctors at the health center, including higher-income people with private insurance through their jobs, Bruno said.
That means some of the patients, she said, make enough to “take responsibility for their care.” But the health center does not track what percentage of patients sent to collections receive financial assistance or make so little that their checks legally cannot be garnished.
Brittney Shea, a single mom with two teenagers, has been sued three times by Eastern Shore Rural Health since 2021. She and both of her children have chronic health conditions that require them to see doctors and specialists frequently, and the $25 co-payments add up quickly, she said.
Most recently, the health center sued her last October for about $2,000 in medical bills and an additional $760 in lawyer fees and court costs, records show. The money was garnished from multiple paychecks from her Walmart job.
Shea is aware that she ends up paying more through garnishments than she would if she paid her medical bills on time. But she said the money just isn’t there on the front end, especially when she has been out of work due to health emergencies. Sometimes she avoids seeing doctors when she is feeling sick to avoid owing more money.
The cycle of lawsuits and garnishments has made it harder to provide for her children, she said. “You expect this money, but then they’re garnishing you,” she said. “Now you got to figure out how you’re going to feed them, how you’re going to put gas in your car to go back and forth to work, how you’re going to pay your rent.”
Many regions served by community health centers lack primary care options and have
a real need for them. That was the case in Hutchinson, Kansas, a historic salt mining town northwest of Wichita, in the 1990s when the local hospital came up with the idea to start PrairieStar Health.
When Aimee Jones started working at PrairieStar in 2015, she had only ever been on the patient side of debt collection. After a difficult divorce decades earlier, she’d had trouble paying outstanding medical bills and filed for bankruptcy to avoid having her wages garnished.
As a patient accounts representative, Jones was responsible for handing patients’ debt over to an outside collection agency once she had exhausted efforts to get them to pay. PrairieStar would send out three statements and two collections notices and often make an additional phone call reminding patients of their unpaid balances and encouraging them to set up a payment plan. The last notice told them that their bill would be sent to collections. (Anderson, the PrairieStar CEO, told ProPublica the collections agency also sent patients multiple notices before escalating to lawsuits.)
Jones said she convinced her bosses to change some policies in favor of patients. The company was initially sending bills as low as $30 to collections, which Jones felt was pointless because the outside agency took a third of the money. She pushed PrairieStar to raise the threshold to $200 in outstanding debt. In more recent years, that amount increased to $500, she said.
In Kansas, unlike Virginia, lawmakers have not significantly limited how health care providers can recover medical debt. Kansas is also one of 10 states that has chosen not to expand Medicaid, leaving thousands of people unable to get health insurance — and potentially more reliant on community health centers.
Many of the patients who qualified for discounted care based on their income had no insurance, Jones said. And even with lower fees, some struggled to afford medical care at PrairieStar. “You don’t stay on top of it or you come in a lot, it’s going to accumulate quite fast,” Jones said. According to the health center’s financial assistance policy, not all services qualify for discounts.
Jones tried hard to convince patients to pay even a few dollars each month so they could stay out of collections. Often, it worked. She was aware that some people, especially those on fixed incomes, had almost nothing to spare. If they didn’t pay their bills or sign up for a payment plan within about six months, she handed their names over to the collection agency.
Jones could request permission to write off some bills for people who had endured extreme hardship, like a woman whose baby died in a house fire or another whose boyfriend and son died in a car accident. But she couldn’t help everyone.
Once the collection agency referred a case for a lawsuit, it was largely out of Jones’ hands, she said. PrairieStar hired a company that handles collections for hospitals in many Kansas counties — Account Recovery Specialists Inc., which has a documented history of requesting arrest warrants for patients who don’t show up to court. (The collections agency told ProPublica that the warrants were ordered by a judge and that it could not discuss its contract with PrairieStar. It has previously denied using the threat of jail to get people to pay.) Each summer, the agency would send PrairieStar a long list of patient accounts deemed “uncollectible” because they had no income or assets, Jones said.
Jones, who retired last year, looks back on nearly a decade of work with a mixture of pride and sadness. She wonders if PrairieStar could have convinced more people to agree to payment plans if it hadn’t contracted with an outside agency. The health center’s patients would have benefited from a law like Virginia’s, she said, which prevents providers from garnishing wages of patients receiving financial assistance.
“We serve the poorest of the poor. These people don’t have any money,” Jones said.
Pursuing debt in court is a choice, and some community health center leaders have opted out.
Several years before Krista Postai founded the Community Health Center of Southeast Kansas in the state’s poorest region, she worked at a hospital that took extreme measures to collect medical debt. As part of her job, she fielded calls from patients unhappy with the billing process. At times, she said, patients reported receiving warnings that they would be sent to collections, even though they hadn’t received a bill.
When she began applying for grants to start her own clinic in 2002, she knew there had to be another way. “If your goal is really keeping people healthier, it makes more sense to deliver care at the lowest cost possible and not drive them into ERs and hospitals,” she said.
Hospitals do not make much from suing their patients, according to research in several states. (Experts did not know of similar studies on community health centers.) One study of Virginia hospitals found that wage garnishment brought in just a fraction of a percent of their total revenue, on average. But patients can see their finances devastated by these lawsuits, especially with the added interest charges, lawyer fees and court costs.
The National Consumer Law Center, a nonprofit that focuses on consumer protection, urges states to set limits on health care providers collecting medical debt. Their recommendations include capping interest rates for debt at 2% a year — much lower than Kansas’s 10% maximum — and prohibiting lawsuits for patients who qualify for financial help. It recommends banning wage garnishment for all patients.
Community health centers should be held to the same requirements when possible, said Berneta Haynes, policy adviser for the center. “The idea here is that certain types of egregious and aggressive debt collections really should just be banned,” she said.
Community Health Center of Southeast Kansas, based in a county with a poverty rate almost twice that of the state as a whole, provides care to many people who can’t afford to immediately pay their bills. Postai said the health center makes “every reasonable effort” to collect money from patients, as required by federal law. But she is determined to never outsource that work to a collections agency, despite the weekly calls she gets from companies hoping to purchase the health center’s debt.
The center’s internal policy says it will not send patients to collections “to ensure that patient dignity is maintained.” Its peers, she said, should do the same.
“Most people try to pay,” she said. “It makes no sense to take an already stressed population and stress them further.”
Instead, the health center finds creative ways to pull in more patients — using federal grants to open discount pharmacies, serving patients at jails and prisons, partnering with other local nonprofits. It has branched out to neighboring counties with no other sources of affordable medical care. Last year, it wrote off about $5.3 million of bad debt from patients who didn’t pay their bills, about 5% of its total revenue, federal reports show.
Postai said the clinic is willing and able to sustain the loss, and she cringes thinking about patients at PrairieStar and similar health centers who may avoid returning there for medical help.
New polling published on Monday shows that the Affordable Care Act (ACA), oftentimes called Obamacare, is more popular than it’s ever been before. The Gallup poll, which was conducted in early November, asked voters to rate how they feel about the ACA. Nearly 6 in 10 voters (57 percent) said they approved of the 2010-passed law, while only a third of voters (35 percent) said they disapproved.
South African billionaire Johann Rupert has enjoyed a sudden surge in wealth. His expanding fortune, like those of billionaires around the world, is not a sign of brilliance or achievement. It is a symptom of a system built to funnel wealth upward into the hands of the 1%.
Rupert’s net worth jumps from $13.7 billion to $19.1 billion in under a year, powered by sales of high-end jewelry through Richemont, the luxury goods holding company he founded. With his exploding profits he invests in hospital networks, viewing them simply as financial assets, not the essential services the rest of us — the 99% — need and have the right to. The headlines call it “performance,” but anyone living outside the 1% knows it is extraction.
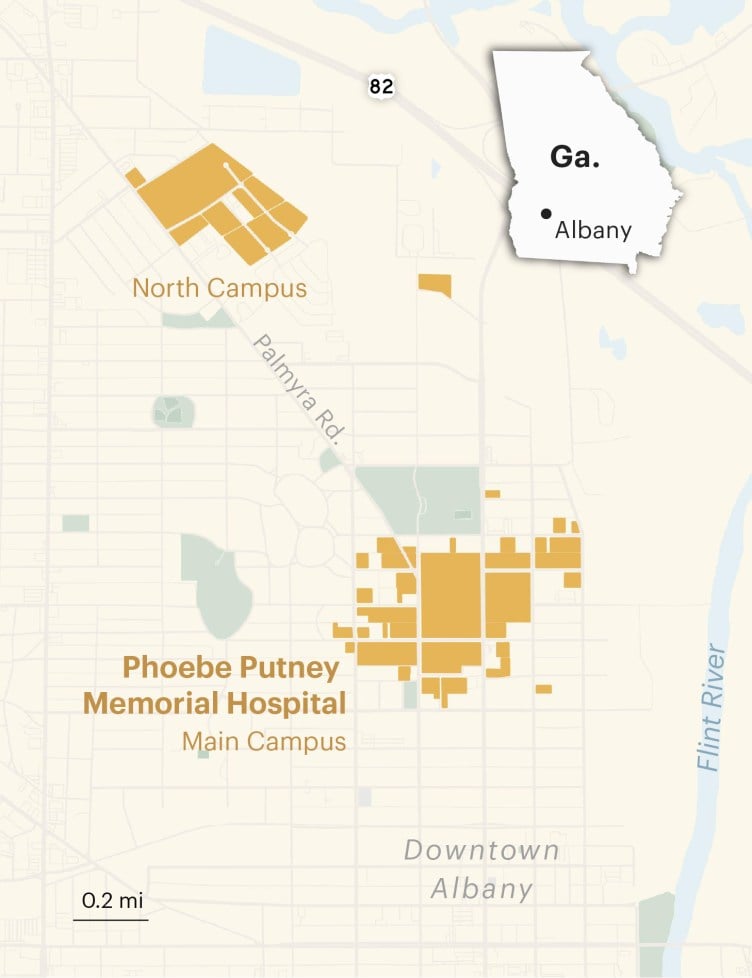
Phoebe Putney Memorial Hospital Katie Campbell/ProPublica
Early morning, May 26, 2022
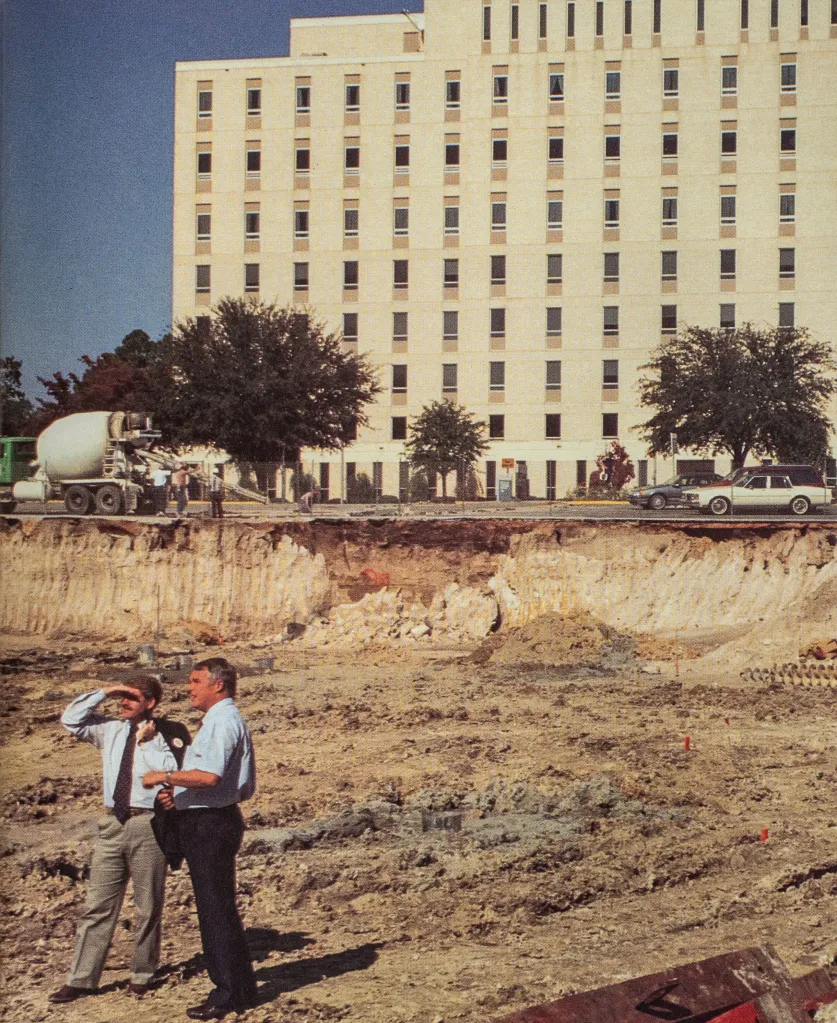
Anthony Parker was tired of feeling tired. He was approaching his 70th birthday and his third decade as president of Albany Technical College in southwest Georgia. He was close to accomplishing the professional project of his dreams, a brand-new center for training nurses, when his heart began to give him trouble. He’d found that it was hard to walk short stretches across campus without getting winded. He’d stopped using the pedestrian bridge that connected the east and west sides of the college because it had become too difficult to climb the stairs. His wife and three adult children were struck by his sudden urge to take afternoon naps, something he’d once ribbed them about, saying they were sleeping their lives away.
But perhaps what most bothered Dr. Parker — which is what everyone called him because he’d earned a Ph.D. and because honorifics are considered good manners in the South — was that his severely irregular heartbeat had begun to affect his golf game. So, on the day before he checked into Phoebe Putney Memorial, Albany’s only hospital, Dr. Parker was anxious to get his stamina back.
His cardiologist, Dr. José Ernesto Betancourt, recommended a procedure called an ablation. It involved running a catheter through a blood vessel from his groin to his heart and applying extreme heat or cold to create tiny patches of scar tissue on the outer walls of the organ, blocking the electrical signals that were causing his arrhythmia. Betancourt told Dr. Parker the procedure was minimally invasive and had a high success rate in men his age. In most cases, patients were sent home the day after the procedure and able to return to normal activities in a day or two.
Because Betancourt was relatively new to Phoebe, the Parkers sought a second opinion from a close friend, a cardiologist who was godfather to their second child. After he heard what other measures had been taken to try to address Dr. Parker’s condition, he agreed that an ablation was an appropriate next step.
Next came the decision about whether to have the procedure at Phoebe. The Parkers had heard horror stories about the hospital from friends and colleagues over the years. But every hospital had stories like that — as far as they were concerned, those were isolated incidents. Dr. Parker was confident that what might have happened to other people would never happen to him. If there’d been anything serious to worry about, some systemic problem, he would have heard about it. For much of the time the Parkers had lived in Albany, he’d served on Phoebe’s board of directors, one of the few African Americans invited to do so. He was a member of what the hospital called the “Phoebe Family.”
He scheduled the ablation for the Thursday before Memorial Day in 2022. He assured his staff he’d be back at work by the following Tuesday and even half-joked about getting out to hit a few golf balls during the break.
When the day arrived, Sandra, Dr. Parker’s wife of nearly 50 years, drove him the 15 minutes to Phoebe. By 7:30 a.m., he had checked into the surgery center. A nurse arrived to wheel him to the catheter lab, where the procedure would take place. Mrs. Parker walked alongside them as far as the entrance. Before saying goodbye, Dr. Parker pulled off his wedding ring and handed it to her for safekeeping. She slipped it on top of her own ring. Then she kissed her husband and told him she loved him as the nurse rolled him away.
One of her younger daughter’s best friends from high school called to check on Mrs. Parker.
“Phoebe better not mess up,” she said.
Anthony Parker with his family in 1990 after he earned his Ph.D. at the University of South Carolina and with his wife, Sandra, in 2008
CHAPTER 1
Albany, Georgia, is a sleepy, majority African American city of some 67,000 that sits along the banks of the Flint River, more than a three-hour drive south from Atlanta. It’s not on any major interstate. Getting there isn’t easy, though there’s not much reason to go without family ties. It’s one of the state’s poorest cities in one of its poorest counties, Dougherty. It’s so isolated and so untouched by time that its own residents like to joke that when the world ends, Albany is the place to be because it will take another 20 years for the end to arrive there.
COVID-19 upended that way of thinking. In early March 2020, Albany became one of the country’s first hot spots. It had the fourth-highest per capita case rate in the world (after Wuhan, China, the Lombardy region of Italy and New York), and the virus was taking a disproportionate toll on neighborhoods with the highest concentrations of poor, Black residents. Suddenly a city that most Americans couldn’t place on a map had become a harbinger of doom: If the virus could strike Albany, nowhere was safe. Phoebe Putney Memorial, the primary command center for the regional COVID-19 response, was inundated with calls from journalists seeking to make sense of how the virus was being transmitted, who was most affected and whether our health care system could save us.
The storylines that were drawn tended to cast American hospitals as national heroes, and Phoebe, like its counterparts elsewhere, embraced the role. Its doctors, nurses and chaplains appeared on magazine covers and morning news shows. They testified at congressional hearings, hosted delegations of state and federal elected officials, were honored at area military ceremonies and virtually presided at the opening bell of the New York Stock Exchange. Phoebe’s executives used daily livestreamed press briefings to appeal for calm and answer questions about whatever new federal guidelines were being issued for preventing the virus from spreading.
Sometimes the executives tripped over the color line, like when the hospital’s chief medical officer, Dr. Steven Kitchen, who is white, announced that thanks to “prudent medical history-taking,” Phoebe had discovered that the outbreak was touched off by an infected visitor from Atlanta who came to attend a service with more than 100 other mourners at a Black funeral home. Many of them went to a second funeral the following weekend. The assertion was so clearly loaded in a town once considered a bulwark of the Confederacy that the chair of the Dougherty County government, who was also white, quickly chimed in, saying, “This is not to besmirch anyone’s reputation,” adding, “No one did anything wrong by going to any of these funerals.”
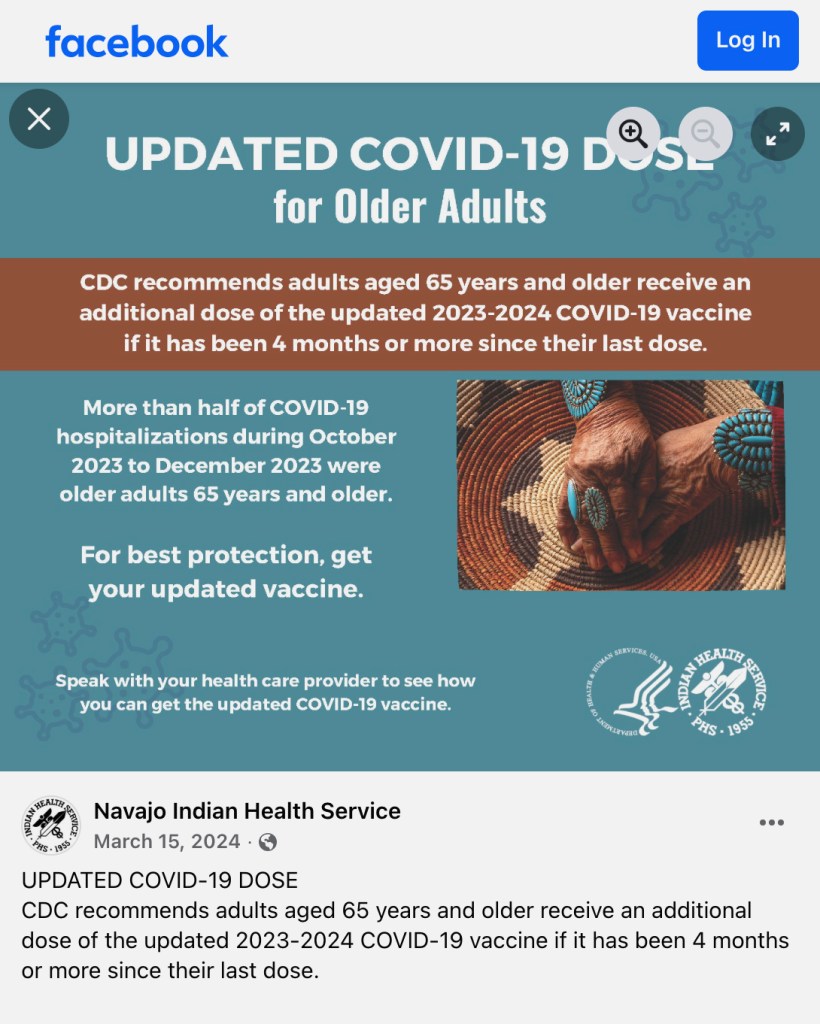
Most of the messaging, though, celebrated the miracles happening inside the hospital’s COVID-19 wards. One video that the press office circulated featured a 99-year-old patient named Maude Burke, who Phoebe had determined was well enough to be discharged from the hospital. In her honor, nurses and doctors had staged their own version of a ticker-tape parade. Burke, peeking out from beneath a poofy hair bonnet, was propped up on a gurney that orderlies pushed through hallways thronged with staff who cheered and waved balloons as it, and she, glided by.
“We continue to celebrate with our COVID-19 patients when they get well enough to go home,” Phoebe wrote in a statement that was released along with the video. The statement noted that Burke was a few months shy of her 100th birthday, which made her the oldest COVID-19 patient it had been able to discharge. “Her strength and determination are amazing,” the statement read, adding, “Thank you for being an inspiration Ms. Maude!”
The Harlem neighborhood, once the center of African American culture and commerce in Albany, GeorgiaKatie Campbell/ProPublica
I was among the throng of journalists who rushed to report about what was happening in Albany. I thought, at first, that it was a compelling place to tell a story about a small town facing a mammoth crisis: David versus Goliath. I interviewed intensive care doctors and emergency room nurses who would call to update me on conditions at the hospital at the end of their shifts. I monitored livestreams of city council meetings and church services. I gathered data about the identities and comorbidities of people who were dying of COVID-19. As I watched the pandemic unfold, I realized I was chasing the wrong story.
COVID-19 was just the latest in a long list of health crises to hit the city. Since the 1990s, its residents had suffered some of Georgia’s highest death rates from heart and kidney disease, according to the state’s Department of Public Health. Data from the Centers for Disease Control and Prevention showed that they’d also suffered some of the highest rates of diabetes in the country. Life expectancy rates in the census tracts immediately adjacent to the hospital were lower than the state average. Teen pregnancy rates were higher. And the indicators that affect a community’s well-being, known as the social determinants of health — such as poverty, unemployment, educational attainment, violent crime and food insecurity — had been going in negative directions for the previous two decades.
Albany’s Poverty Rate Was More Than Double the National Rate in 2023
Source: American Community Survey 2023 Five-Year Estimates
Perhaps the most important determinant of a community’s health, however, is access to care. In this, Albany seemed more fortunate than other cities its size because it has Phoebe, a self-described world-class health system that is so intimately woven into residents’ lives that they call it by its first name. Its main hospital in Albany is licensed to operate 691 beds, and it owns two other area hospitals, a cancer center, a hospice, as well as numerous outpatient clinics, urgent care facilities and medical practices covering specialties, including bariatrics, cardiology, anesthesiology, gastroenterology, neurology, urology and sports medicine. It has long run training programs for specialists in family medicine and pharmacists. Over the past three decades, the system has not only grown into the largest provider of health care in southwest Georgia, but it has also become the region’s largest employer with more than 5,500 employees and a footprint that covers a large swath of the center of town.
I began to focus on the relationship between Phoebe’s breakneck growth and the rates of chronic illnesses among Albany’s residents and wondered whether the city was more of a microcosm than a hot spot. It wasn’t the only place where the poorest among us are also the sickest. The United States is blessed with one of the most scientifically and technologically advanced health care systems in the world, a sprawling industry so vast and lucrative that it is now one of the largest drivers of the economy, accounting for more jobs and revenue than manufacturing. But for all the money flowing in and out, Americans have more chronic illnesses and shorter lifespans than people in other wealthy nations. When it comes to health outcomes among those countries, the United States ranks last.
I set out to answer a question I hoped would resonate with anyone who’s ever struggled to get the health care they need. Why are people in Albany — and, for that matter, the city of Albany itself — so sick when its most powerful institution is a hospital?
I started by speaking to dozens of people whose loved ones had died at Phoebe during COVID-19. It didn’t surprise me to learn that not all the miracles posted on Phoebe’s Facebook page were true. Maude Burke’s relatives told me she hadn’t fully recovered from COVID-19. She’d been readmitted to the hospital a couple days after she was discharged and died shortly thereafter. Nor did it surprise me that relatives like hers were bitter about their loss and that some blamed Phoebe for mishandling their loved ones’ cases. (A Phoebe spokesperson said, “We are confident that Ms. Burke received quality, compassionate care during her stay at Phoebe and that she was appropriately discharged.”)
What I didn’t expect was how fearful people were to criticize Phoebe on the record and how powerless they were to hold the hospital to account. The same was true of many of the current and former employees of the hospital.
Phoebe Putney Memorial Hospital at sunriseAlmudena Toral/ProPublica
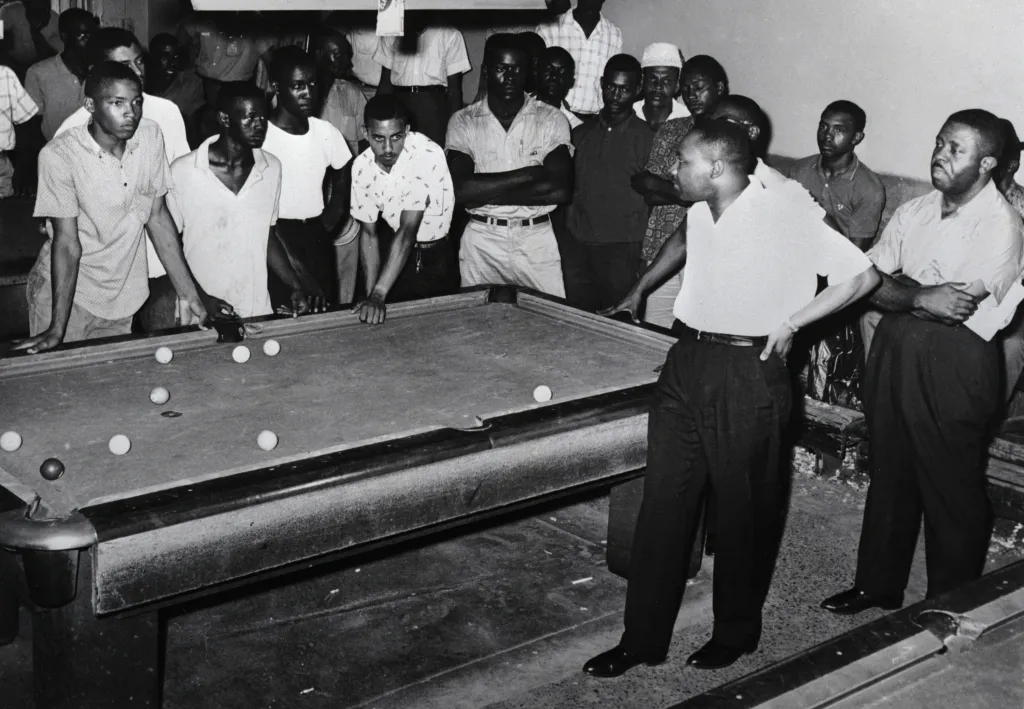
Still, people encouraged me to keep digging. Among them was Pastor Daniel Simmons at Mt. Zion Baptist Church, home to one of the Rev. Martin Luther King Jr.’s earliest and least successful civil rights campaigns. He told me that he had serious doubts about Phoebe’s account of the outbreak’s origins and that rather than bringing the community together it had cast African Americans as culprits. Even Georgia’s governor, Brian Kemp, picked up the explanation, telling the press, “We had an infected person do the wrong thing and go to a funeral service.” The funerals, Simmons said, were not the only potential superspreader events to have occurred in the weeks leading up to the outbreak. The city had also hosted a marathon to raise money for Phoebe that drew runners from across the country.
I later learned that Simmons was on to something when I met an epidemiologist named Daniel Pollock, who’d retired from the CDC and was researching a paper that examined the origins of Albany’s outbreak. He told me that Phoebe’s assertions were, at best, “highly speculative” and, at worst, “deliberately misleading.” Phoebe’s COVID-19 narrative, he told me, was “deeply flawed from an epidemiological perspective, stigmatizing from a health communications perspective and unjust from an ethical perspective.”
There was no conclusive scientific evidence linking the virus’s introduction in Albany to a single person, Pollock said. Yes, he told me, Patient Zero, as he came to be called, could have carried the virus to the city. But there’s compelling evidence that the virus was circulating widely and undetected in Georgia, including in Albany, weeks before the patient arrived at Phoebe. Doctors there mistakenly thought his rapidly deteriorating condition was connected to a previous and long-standing respiratory illness, not a new one. They never tested him for COVID-19, which Pollock said went against the CDC’s recommendations at the time.
That patient spent seven days at Phoebe before he was transferred to a hospital back in the Atlanta area, where he could be closer to home. That hospital notified Phoebe that the patient was COVID-19 positive.
Because Phoebe failed to test the patient, it’s impossible, Pollock told me, to know for sure whether he carried the virus into the hospital or contracted it there. What’s certain, though, is that the phone call from Atlanta was the first time Phoebe understood that dozens of its staff had been exposed to the virus. At the minimum, the hospital was as much a superspreader location for Albany’s outbreak, Pollock said, as the two Black funerals that Phoebe officials had called out in that March 2020 press briefing.
“It was an abject failure on Phoebe’s part not to test him and isolate him as soon as he entered the hospital,” Pollock said. He pointed out that although tests were hard to come by at the time, the Atlanta-area hospital tested the patient as soon as he arrived. Phoebe’s failure to do so, he said, “made it difficult to pinpoint when and where the first case occurred. Instead of admitting as much, Phoebe wanted to find an explanation that omitted their medical mishaps. It amounted to a cover up.”
Kitchen agreed that without having tested Patient Zero for COVID-19, it was “impossible to definitively say” that he was the source of the outbreak. However, he added, “I think it’s very likely that he was.” His conclusions, he said, were based on the best information he had at an extraordinarily chaotic time. Pollock has had the luxury of investigating the matter long after the crisis ended.
A Phoebe spokesperson echoed Kitchen’s views. He said: “It is a fact that the first confirmed COVID patient treated at Phoebe was visiting Albany for a funeral. It is also true that most of the sickest patients who filled our critical care units in the first days of our COVID battle were connected to several gatherings in the community.”
When I asked Kitchen about the stigmatizing effect of Phoebe’s initial assertions about the origins of the outbreak, he seemed taken aback. How could telling the public what he knew as soon as he knew it be stigmatizing? He hadn’t said anything in any way that had blamed anyone. Why would Black people feel that he had?
“There was no suggestion or tone of judgment or blame,” he said. “I was simply conveying information factually and with great sensitivity and compassion for everyone who was affected.”
Simmons didn’t know about Pollock’s paper. His skepticism about Phoebe’s funeral explanation came from what he’d learned during his years living in Albany about how power works there. It was part of a familiar pattern, he said, and with time, I would see it, too.
“If Albany, Georgia, had done things differently over the years, our community wouldn’t have been as vulnerable as it was,” he told me. “If the health care system was different, if it had a different relationship with poor people and people of color, the outcome would have been different.”
The main lesson he said that he hoped I and other people would take from Albany’s COVID-19 crisis was, “It didn’t have to be this way.”
Anthony Parker and his son, Richard, in 1986
Late afternoon, May 26, 2022
Mrs. Parker felt her eyes well up as she arrived at the waiting room. Sixty-seven years old, compact, with a dark complexion and close-cropped hair, she had been a high school assistant principal for many years and had a lot of practice projecting confidence under pressure. But her wide, expressive eyes gave her away. The clerk took Mrs. Parker by the hand and promised to pass on any and every update she received about her husband.
Mrs. Parker took a seat in a less-crowded corner of the waiting room and pulled a bag of peppermints and her iPad from her purse, hoping she’d find enough reading to distract her. On the wall above her, she caught sight of a portrait of the late Dr. Carl Gordon, a towering figure in the hospital’s history and a friend of the Parkers.
Gordon had left Albany after high school in the mid-1940s to attend college. Afterward he joined the military, served in Korea and Vietnam, then returned to Albany in 1968 because there were no Black surgeons in the city. He told people that conditions at Phoebe had “improved 100%” since he’d left — by which he meant they were still bad, but less bad. Federal law had forced Phoebe to integrate its staff and patient wings. Dr. Gordon became the second Black physician granted privileges at Phoebe and, in 1993, its first Black chief of staff.
The Parkers moved to Albany two years later when Dr. Parker took over running Albany Tech. The two families became close, partly because they were among the handful of African Americans in high positions at major institutions, who’d bought homes in neighborhoods next to country clubs, and moved easily — or knew how to make it look like they moved easily — across the color line.
Looking up at the portrait, Mrs. Parker tapped out a text to Dr. Gordon’s son. “Your Dad,” she wrote, “is keeping me company and giving me comfort.”
Relationships like that made Phoebe feel like more than a hospital to the Parkers. In the weeks leading up to the procedure, they’d received well wishes from the hospital’s president and the health system’s CEO and chief medical officer, along with nurses who’d been students of hers and her husband. Phoebe had recently hired the Parkers’ elder daughter, Kim, who has a Ph.D. in public health, and had agreed to a $40 million deal with Albany Tech to significantly expand its nursing program. It was a project that Dr. Parker for years had pressed Phoebe to support. He believed it would create good jobs for a community badly in need of them, revitalize the school and address critical staffing shortages at the hospital.
The morning and afternoon passed with no word, except that the procedure was still underway. Around 4 p.m., Mrs. Parker asked for the umpteenth time about her husband. A nurse arrived from the catheter lab to tell her that there was nothing to worry about. It was not unusual for an ablation to take longer than expected because of the time required to map the arteries of a patient’s heart. The receptionist told Mrs. Parker that the waiting room would close soon, but that she could stay there as long as she needed.
Around 4:30, Betancourt arrived. He seemed a bit out of breath, but he was smiling. The procedure had gone well, he told Mrs. Parker. Her husband’s blood pressure was running low, but they were giving him some medication to stabilize it, and they were going to have him spend a night in the ICU so that he could be closely monitored.
He told her that her husband might be out of it for the next six to 12 hours but that he believed they had accomplished what they wanted. He asked Mrs. Parker to give him an hour to get her husband ready for transfer and then he’d take her back to see him. She could stay with him for a while, if she liked, but he said she should go home and get a good night’s sleep since Dr. Parker was unlikely to be awake before morning.
Relieved, Mrs. Parker dashed off texts to her three kids and eight siblings. She packed her iPad and sat back down to wait for Betancourt to return. When Betancourt reappeared, she thought he looked pale and panicked.
He pulled up a chair and told her there had been some complications. Her husband had gone into cardiac arrest.
Mrs. Parker felt the room spin and blinked hard to try to keep herself focused. Maybe she misunderstood the doctor. He was Cuban-born and -trained and spoke with a thick accent.
She thought to herself, “Did he just say Anthony had a heart attack?”
Before she could open her mouth to ask, Betancourt told her that he’d responded to the arrest as soon as it happened. As for how long her husband’s heart had stopped beating, it couldn’t have been more than five or six minutes.
“That’s not a lot of time,” she thought. “Is it?”
CHAPTER 2
In May 2020, after the first wave of the pandemic had subsided, Albany’s mayor, Kermit “Bo” Dorough, discussed the city’s response to the crisis in an interview with a monthly current affairs program called “The Buzz” on Queen Bee radio station.
Video of the show was livestreamed, so I was able to watch it. Queen Bee’s studios were inside a downtown brewpub. Like the mayor, the two hosts were white and had long been fixtures on the local political scene: Carlton Fletcher, the longtime editor of the Albany Herald, the area’s one daily newspaper, and B.J. Fletcher, no relation, a rare Republican member of the City Commission, what Albany calls its city council.
The mayor, a workers’ compensation lawyer in his early 60s, had only been in office for four months, a tenure that had been consumed entirely by COVID-19. He’d long been an opponent of the city’s establishment, especially Phoebe. His election had been attributed more to abysmally low turnout among Black voters rather than a surge among whites.
After opening the conversation on a congratulatory note, the hosts turned quickly to the crisis at hand, and Carlton Fletcher asked his co-host and guest to share their thoughts about Phoebe’s performance.
B.J. Fletcher answered first. Just as she’d been raised to show respect to military officers and preachers by standing up when they walked into a room, she said, she now felt compelled to do the same for health care workers. “I can’t see Albany without Phoebe,” she said, and called the hospital’s response to the pandemic “top of the line.”
When she finished speaking, Dorough pounced like a dog on a rib eye. “That’s a juvenile statement,” he said. Then he cleaved his hands to his chest and reminded those listeners living in Albany, or anywhere else in Dougherty County, that the hospital belonged to them.
“We own Phoebe Putney,” he huffed.
Rainbow Records in HarlemKatie Campbell/ProPublicaA car hobbyist meetup in North AlbanyRoss Landenberger for ProPublica
Dorough wasn’t just spouting a political talking point. Founded in 1911, Phoebe Putney Memorial was operated by the county government from 1941 until the early 1990s. But then, in a move that allowed the hospital to expand its services beyond the county limits, Dougherty officials agreed to lease the facility to a private nonprofit entity with the same name. That’s when Phoebe Putney Health System was born. Under the new arrangement, the county kept ownership of the building in which the main hospital operated, but it lost control of the day-to-day management of the hospital, including, to Dorough’s chagrin, how much it charges its patients.
Dorough told Queen Bee listeners that he was convinced Phoebe’s patients paid way too much. “Just because Phoebe Putney has made such valiant contributions to our community in the last few months,” he said, “doesn’t change the fact that health care costs are higher here than anywhere else in the southeast United States.”
Cost is one of the great mysteries of American health care, and few communities have fought over the issue more vigorously than Albany. Phoebe hasn’t always been Albany’s only hospital. It became so after a long and highly contentious fight that was the subject of countless newspaper articles, a feature-length documentary and a lawsuit by the Federal Trade Commission that went all the way to the Supreme Court. Throughout that fight, Phoebe had denied that its prices were out of line, but, like most hospitals, it refused to divulge them for competitive reasons.
Dorough reminded listeners that on the night he became mayor he pledged to find a way to get an independent study of health care costs across the region to determine how Phoebe’s fees compared with those of other hospitals, something he’d been demanding for years. Now that he was mayor he felt confident he was in a position to get it done, and he challenged his colleagues on the city and county commissions to join him, saying that Albany’s future was at stake.
“I don’t think it’s a community hospital that first and foremost benefits the community,” he said of Phoebe. “I think it is a business model where you’re driven by profits.”
A few weeks later, I met a young Black man named Clifford Alexander Thomas. We met at a sandwich shop downtown. He’d lost his 61-year-old mother, Beverly “Kay” Thomas, to COVID-19 not long after the outbreak and was still grieving. It was hard enough, he told me, to make peace with the fact that a virus from China had made its way to “Small-bany,” as he called his hometown, and took away his favorite person in the world. But he doubted he’d ever be able to make peace with Phoebe, not because it didn’t know how to save her but because of the way it had treated her, and him, after she died.
Thomas, tall and thick through the middle, pulled out his cellphone and showed the last photo he’d taken of his mother. She was lying on her bed at the hospital, her mouth caked in mucus, her torso half-exposed and tangled in tubes and tape. Judging from the way his mother looked and by the gowns and sheets that littered the floor, Thomas guessed that his mother’s final moments had caused some commotion. But what he couldn’t understand was why the hospital staff hadn’t taken the time to clean her and her room, even though he’d told them that he and his sister were on their way to the hospital to say their goodbyes.
“Why would they leave her like that?” Thomas asked. “Is that what they call taking care of someone? Did they really do everything they could to save her life? Did they think about how it would feel if that was their momma left like a lab rat?”
I suggested there might be an explanation. Hospital staffers were probably so busy handling the crush of COVID-19 cases that they couldn’t clean his mother up as quickly as they should have. Perhaps they’d had to rush away to try to save other lives?
Thomas didn’t budge. He told me that while he and his sister were standing over their mother’s body, a white nurse walked into the room and, without saying a word, began disconnecting the IV. He said he broke the awkward silence by asking her whether he could retrieve his mother’s belongings. The nurse, he told me, looked over at him and said, “This one didn’t have any belongings.”
He said he struggled to keep his composure because that’s what his mother would have wanted. She’d been born at Phoebe, delivered by an obstetrician who used forceps to pull her into the world, leaving her with a permanently disfigured right limb. Her parents sent her to Atlanta for surgeries to try to repair the damage. But they never filed a complaint against Phoebe or its obstetrician because Black people didn’t sue white doctors in those times, and no one, particularly poor African Americans, dared get on the wrong side of the only hospital in town.
Watching that nurse removing tubes from his mother without acknowledging his and his sister’s loss, Thomas said, his anguish got the best of him. He told the nurse, “Be mindful of the next words that come out of your mouth.” Then he asked her to get out of his mother’s room altogether.
He said the nurse left and came back with a security guard who ordered him to leave.
“That definitely tore me with Phoebe,” he said.
Remembering Beverly “Kay” Thomas 1958-2020
Beverly “Kay” Thomas Courtesy of the Thomas familyThomas with her son, Clifford Alexander Thomas, top; his wife, Diamond Thomas, left; their son, Ca’Marion Alexander Thomas; and Clifford’s sister, Zandria Thomas, right
Courtesy of the Thomas family
A Phoebe spokesperson said that while the hospital could not confirm Thomas’ encounter with the nurse, “his perception indicates that she — and we as an organization — could have done better.”
All across Albany, I found evidence of tattered relations between the hospital and the city. Those with insurance — many of them white or well-off — were critical of the hospital in the same ways as Dorough. They described Phoebe as a behemoth that had unfairly driven off its competition, jacked up its prices and pumped more money into executive salaries than into improving its services. They complained that the hospital’s nonprofit status created a drain on the county’s tax base, and they blamed the hospital’s high fees for their exorbitant health insurance rates.
Those without insurance or on Medicaid — many of them Black and employed in low-wage jobs — complained about the quality of care. They described everything from long waits in the emergency room and dismissive attitudes among nurses and doctors to lapses that cost them or their relatives life and limb. They almost never claimed ownership of the hospital but instead described its leadership and their own stubbornly high rates of disease as vestiges of the institution’s history, throughout which whites set the hospital’s priorities and expected African Americans to go along or go elsewhere, knowing there wasn’t anywhere else.
Both critiques were not only commentaries on Phoebe’s economic and political power but echo American sentiments about our health care system as a whole. That’s largely because most people don’t think of hospitals the way they think of themselves. Although the United States is the only industrialized country without universal health insurance, we cling to the notion of our health care system as a public service because that’s often how hospitals portray themselves.
The reality, however, is that hospitals are businesses, first and foremost. The decisions they make about the kinds of services they provide, the staffing they need to provide them and even the amount of financial assistance they offer to the poor are not driven first by the health needs of a community but by what the hospital needs to maintain its bottom line. That’s even true at the nearly 60% of hospitals that are nonprofits, which enjoy tax exemptions worth $37.4 billion a year.
Nearly 1,600 mergers over the past two decades have made hospitals some of the biggest companies in the country. They have played leading roles in the redevelopment of old industrial capitals like Cleveland, Buffalo, Baltimore and Pittsburgh and turned their downtrodden centers into gleaming, glass-encased landscapes. All this consolidation, however, has its pernicious effects. It’s not the pharmaceutical industry that is most responsible for driving up the nation’s health care costs; it’s the hospital industry. The Centers for Medicare & Medicaid Services recently reported that hospitals account for nearly one-third of the $4.9 trillion the nation spends on health care. Retail and prescription drugs, according to the report, account for only 9% of spending.
Just like any other industry, the more concentrated the money becomes, the fewer incentives there are to lower costs or improve quality and the less communities can do about either. The imbalance is most acute in small cities like Bryan, Ohio; Beatrice, Nebraska; St. Joseph, Missouri; Owensboro, Kentucky — and Albany, Georgia. Their survival is hitched to the fates of oligopoly health systems the way towns in West Virginia and Kentucky once were to coal. They’ve become hospital towns.
Doretha Moultrie, bottom row, second from left, with her nursing school classmates and instructor in 1963. She went on to work at Phoebe.Courtesy of Doretha Moultrie
Early evening, May 26, 2022
Kim, the Parkers’ elder daughter, was the first to show up at the hospital after her mother alerted the family about Dr. Parker’s cardiac arrest. The two of them had barely stepped off the elevator on their way to one of Phoebe’s intensive care units when his cardiologist, Dr. José Ernesto Betancourt, and three other physicians rounded the corner. For Mrs. Parker, the sight of them, shoulder to shoulder, all in white coats, conjured the image of the Four Horsemen of the Apocalypse. “This isn’t good,” she whispered to Kim.
Dr. Jyotir Mehta, the chief of Phoebe’s critical care team, stepped ahead of the pack to take Mrs. Parker’s hand and asked whether she knew who he was. Of course she did, Mrs. Parker thought to herself. She’d known Dr. Mehta for years. He’d served on the health system’s board with her husband. What he was really asking, Mrs. Parker thought, was whether she had her wits about her; whether she was mentally capable of understanding what he was about to tell her; that if she wanted to fall apart, now was not the time.
“Yes, Dr. Mehta,” she nodded, thanking him for being there.
Dr. Dianna Grant, the health system’s chief medical officer and a friend — she’d been the one who’d hired Kim — arrived shortly after. She told Mrs. Parker that the health system’s entire executive team had been notified about what had happened. Your Phoebe family is here, she said, and we love you.
This was the embrace Mrs. Parker had hoped for — the one Phoebe reserved for its inner circle. Whether Grant intended it, her words felt to Mrs. Parker like a secret handshake, an invitation to let down her guard and cry, and she did, falling into Grant’s arms sobbing.
Friends and colleagues from Albany Tech began arriving. Betancourt pulled Mrs. Parker and her daughter aside and began going over what he’d said before: how he’d been right there when the cardiac arrest occurred and how quickly he’d gotten Dr. Parker’s heart beating again. It couldn’t have been more than five minutes. It appeared the cardiac arrest hadn’t caused any significant harm to Dr. Parker’s heart. It was functioning well. What worried Betancourt and the rest of the critical care team was the extent of damage to their patient’s brain, which had been starved of oxygen when his heart had stopped beating.
He told her that Dr. Parker had not awakened. Another doctor, whom Mrs. Parker didn’t recognize, joined the conversation and told her that the medical team wanted to try a treatment that would involve cooling her husband’s body below normal to slow his metabolism and reduce his brain’s need for oxygen, giving it time to rest and restore. The cure is a little R&R, she thought to herself.
The doctor explained that therapeutic hypothermia had been developed by doctors who’d found that they could revive skiers who’d fallen unconscious below sheets of snow and ice for long periods. Betancourt assured Mrs. Parker that her husband would be kept comfortable throughout the treatment, which he estimated would last 72 hours. In the final phase, he told her, they’d slowly return Dr. Parker’s temperature to normal and wake him.
Mrs. Parker took the doctor’s plans to wake him as a promise. The sooner the doctors got started, the sooner she’d have her husband back. “That’s no time at all,” she said to Kim. “Hell, we can stand on our heads for 72 hours if we need to.”
Anthony Parker with his elder daughter, Kim, in 1999, celebrating her masters degree from the University of South Carolina
CHAPTER 3
More than a century ago, the great sociologist and civil rights activist W.E.B. Du Bois wrote about Albany in his landmark “The Souls of Black Folk,” and the city still looks and feels a lot like the place he described: “wide-streeted” and “placid.” The Flint River, which once separated Black neighborhoods from white ones, still serves as an economic dividing line, with wealth concentrated on its far west side and poverty on the east. The town, Du Bois wrote, “takes frequent and prolonged naps.” There were many afternoons when I drove through Albany and felt as if I were the only one there — except for Phoebe.
Phoebe’s everywhere. Its logo and advertising can be found on the sides of high school sports stadiums and on billboards rising above the fast-food restaurants, Dollar Generals, discount strip malls and liquor stores that line commercial thoroughfares. There are Phoebe golf tees. Phoebe pens find their way into glove compartments and purses. I went to the beach with Clifford Thomas’ family, and he offered me a Phoebe beach chair. At almost every community event I attended, at least one person wore a Phoebe T-shirt, cap or jacket.
The hospital itself isn’t much to look at. It’s a blond brick-and-concrete structure with a spearmint-colored roof, made up of a main building with nine patient floors and two adjoining wings for outpatient services and a new trauma tower. Those facilities occupy more than five square blocks at the center of the city.. The hospital towers over the properties that surround it, including nearly 100 that Phoebe had acquired over the years. It has turned a bit more than half of those properties into facilities for its own use — an energy plant, parking lots, housing for cancer patients, a day care center for its employees. It has left many vacant and unattended.
A block from Phoebe, on one of my solitary drives through town, I spotted an elderly man watering a rose bush with deep fuschia blooms outside a red brick Craftsman-style home. His name was Nathaniel Smith. He and his wife, Mary, seemed happy to have some company, and they invited me up to their porch to talk.
“Are you the only people living on this block?” I asked.
He smiled, and nodded yes, as if he’d heard that question before. Then he asked whether I worked for Phoebe and was interested in buying his place. The hospital began acquiring the other houses on his block in 1986. It now owned all but one, he told me. I looked around — roofs had fallen in, lawns were littered with empty liquor bottles and fast-food wrappers, there were holes in walls where windows used to be.
The Smiths asked me if I had any idea whether the hospital had a plan for the houses. I told them that I did not. Then Mr. Smith shook his head and scowled, “It don’t make sense for a nonprofit hospital to buy up all these houses and let them go to waste like that.”
Nathaniel and Mary Smith were in their 80s. When they moved into their home in 1987, he worked as a peanut sorter at the M&M Mars plant. They paid $46,000 for the house. They told me they put down all the money they had, but they saw it as a smart investment in a home where they could comfortably live out their days and then pass on to their daughter. When they arrived in the neighborhood, it was filled with working families like theirs. Their daughter was able to walk to school. Mary, a seamstress, converted the shed out back into her sewing studio. Nathaniel doted on his flowers. “It was a real nice place to live,” he told me.
By the time I showed up, Phoebe and Mr. Smith’s rosebush seemed about the only thing flourishing in his neighborhood. The Smiths had stayed put all those years because they couldn’t afford to leave. Phoebe, they said, had been the only buyer to express interest in their property, but the hospital had only offered a little more than what they’d paid for it, which wasn’t enough to cover their mortgage and the cost of settling elsewhere.
When I first told Mr. Smith that I was a reporter, his eyes lit up and he asked whether I’d ever met Oprah. I shook my head and told him that I’d spent the bulk of my career reporting from Latin America. Then he said something that made me think he was reading my mind.
“I bet you ain’t never seen a place like Albany.”
Nathaniel and Mary Smith’s home in Albany, Georgia, a block from Phoebe
Katie Campbell/ProPublica
One of the many ironies about Albany, a city where Confederate flags still fly, is that its most important institution was founded with money from a man who fought for the North. Francis Flagg Putney, a New Hampshire native and a veteran of the Union Army, arrived in Albany shortly after the Civil War. A supporter of Black civil rights, he was shot in the shoulder in 1868 in what became known as the Camilla Massacre when whites opened fire on a political rally he helped lead in a nearby town, leaving 12 dead and dozens injured.
Putney abandoned politics soon after; instead, he devoted his energy to building the region’s largest and most profitable cotton farm. In 1909, a women’s association asked his support for the construction of the city’s first hospital. He agreed to donate $25,000 on three conditions: that the hospital be made of bricks, so that it was fire resistant; that it bear his mother’s name; and that it serve both Blacks and whites.
The women agreed, which set the hospital apart from most others in the country. But just because Phoebe admitted Blacks, it didn’t mean they received the same treatment as whites. There were only a small number of Black nurses until the mid-1950s, and they were almost exclusively assigned to Black patients or to night shifts. White nurses were addressed by their last names; Black nurses were just called “nurse.” The cafeteria had white-only counters. Until at least 1960, Black patients were housed in the basement, alongside the furnace, steam pipes and laundry machines. Black doctors were denied privileges until 1965.
Phoebe acknowledges its segregated past in a 230-page book it published called “A History from the Heart,” but it makes few mentions of how Black patients and doctors were treated, and even those minimize the nature and effects of the indignities Blacks endured. Here’s one passage:
“Queen Jenkins, R.N., Phoebe’s only African American registered nurse in 1960, remembers some difficulties with patients, black and white, and co-workers. White patients often asked for a white nurse, and so did some black patients. LPNs and nurses aides sometimes did not want to take orders from her. Remembering her mother’s advice, ‘let your work speak for you,’ Mrs. Jenkins tried to ignore the racial prejudice.”
Before World War II, Albany was an impoverished agricultural town, its majority black population working mostly in the surrounding cotton and pecan fields. After the war, thanks largely to the opening of a nearby B-52 bomber base and, later, a Marine logistics base, it experienced an economic boom. In 1952, Merck opened a pharmaceutical factory on a 640-acre lot, drawing hundreds of chemists and their families.
The influx of money and educated workers contributed to changing Albany to a majority white town but also to making race relations there different from the poorer, rural counties around it. Although the Ku Klux Klan openly held meetings around the city, Albany did not experience the lynchings and other forms of terrorism that raged elsewhere. Amid the relative calm grew a small, but notable Black elite, made up of doctors, lawyers, business owners, ministers and educators, who held onto their gains, as nurse Jenkins did, by not openly challenging the racial status quo — mostly because they knew things could be much worse.
The quiescence was disrupted in 1961, when the city’s Black high school and college students, emboldened by the sit-ins and Freedom Rides challenging segregation throughout the South, launched a series of protests at the Trailways bus station. Administrators at the historically Black Albany State University attempted to quell the demonstrations by suspending protesters. There were discussions among ministers about driving the organizers out of Albany, though no one acted on them. When the students pressed on, and the police chief began sending them en masse to jail, the elders rushed to take control of the movement, hoping to stop the tensions from turning violent.
They turned for leadership to the 32-year-old Rev. Martin Luther King Jr., who had gained renown five years earlier for organizing the Montgomery bus boycott in Alabama. Albany became his second major civil rights campaign and is widely considered the only one that failed. The city was seized by demonstrations and arrests, with at least 1,000 people following King to jail. But the resentments between the older and younger factions of the movement never mended. They were unable to agree on the goals of their campaign, much less the tactics for winning them. In the end, the movement ran out of money and foot soldiers before the police chief ran out of jail cells.
Demonstrators in front of Albany City Hall in January 1962Donald Uhrbrock/Getty ImagesAlbany taxicabs with the words “White Only” in August 1962Warren K Leffler/PhotoQuest/Getty ImagesThe Rev. Martin Luther King Jr. and the Rev. Ralph Abernathy, far right, talking with a group in an Albany pool room in July 1962
Bettmann Archive/Getty ImagesA Ku Klux Klan gathering of approximately 3,000 outside of Albany in September 1962
Bettmann Archive/Getty Images
King left Albany defeated. Managers at the public library closed its doors when Blacks attempted to check out books. Public transit administrators shut down service rather than allow Blacks to occupy any seats on buses that they wanted. Park supervisors took down nets at an African American tennis court when integrated doubles attempted to play there. After Congress passed the Civil Rights Act in 1964, whites established private schools or moved to surrounding counties to keep their kids out of integrated classrooms. And in 1970, a group of white neurosurgeons opened a new medical center, less than 2 miles from Phoebe, called Palmyra Park.
The neurosurgeons had joined forces with what would become the largest for-profit hospital chain in the country — the Hospital Corporation of America. Its founders patterned the company after fast-food franchises, seizing on the fact that the newly enacted Medicare bill essentially allowed hospitals and doctors to charge the federal government what they wanted. With its manicured gardens, high-end meals and private rooms, the 223-bed Palmyra quickly became the hospital for people with means.
The Phoebe swag that blankets the region today? No one went near it back then, according to Duncan Moore, who ran Phoebe in the mid-1980s. Throughout his time in Albany, Moore told me, white people referred to Phoebe as “the nigger hospital.” He said he had a hard time getting doctors to stop sending all their well-insured patients to Palmyra and all their underinsured patients to Phoebe. He would wander the hospital floors, scanning daily admissions sheets and engaging in hallway shouting matches with offending doctors. “It got to be like hand-to-hand combat,” he said.
Late evening, May 26, 2022
After giving Phoebe’s doctors permission to begin the hypothermia, Mrs. Parker asked to go see her husband. When she got to his room, she barely recognized him. He looked nothing like the person she’d kissed that morning. That man was vibrant, upbeat and indomitable. This one — prone, pale, cold to the touch — was at the mercy of others.
“That’s so not Anthony,” she thought, not the man who in most crises during their 50 years of marriage had taken charge.
She started talking to him with all the confidence she could gather, hoping that he was able to hear her. “I love you. I’m here. I’m not going anywhere. I know you’re going to pull through this. You always do. This will be one more thing we’ll have to talk about.”
From the moment he escorted her to the junior prom in Orangeburg, South Carolina, she and Anthony talked about everything. Like so many teenage love affairs, their attraction was primarily physical at first. He was tall and had a mustache. She had curves and a blinding smile. His parents were friends with her grandparents. She’d been raised in a big, raucous family by a father who was a truck driver and a mother who was a cosmetologist. He’d been the sheltered only child of an elementary school teacher and the principal at a nearby high school that was segregated like hers. But their different temperaments complemented each other. “She’s the nicest girl I’ve ever met,” he wrote in his senior memory book. “And somehow I’m going to get it through her thick head that I love her.”
Two years later, when she was a freshman and Anthony a sophomore at the historically Black South Carolina State University, he asked her to marry him. She skipped gym class and he took the night off from his job as an orderly at the campus hospital to elope. His mother swore she’d never forgive her new daughter-in-law for denying her the joy of a big wedding, but then Kim was born and any hard feelings were forgotten.
Mrs. Parker wasn’t worried that Anthony lacked a clear plan when he earned his business degree. They would figure it out. After getting laid off from an administrative job in a nearby factory, he went back to South Carolina State for a master’s in rehabilitation counseling and landed a job in the marketing department of Augusta Technical Institute, which was part of Georgia’s system of technical colleges. It was there that he found his calling. He’d run a school, like his father.
He received a Ph.D. in education administration at the University of South Carolina. Few of the white administrators at Georgia’s technical colleges had doctorates. They also didn’t have to get over the same hurdles he did. Still, that awareness didn’t prevent him from being deeply wounded when he was passed over for president of the technical college in Statesboro in favor of a white man. He declared himself done with Georgia and took a job at a trade school in South Carolina. Then in 1995, one of his former colleagues called to tell him that the president’s position was open at Albany Tech and that the commissioner of the state’s trade schools wanted him to apply.
A nurse tapped on the door of Dr. Parker’s room. She gently mentioned to Mrs. Parker that it was getting late and offered to take her to a place where she and her children could make themselves comfortable during the 72-hour cooling period. It wasn’t going to be necessary for them to contort themselves into rigid chairs. Phoebe had set them up in what it called its “hospit-el” — hotel rooms in a hospital — that it offered to VIPs. The nurse said that Mrs. Parker’s family had been assigned one of the nicest rooms.
It had two double beds, a flat-screen television and a desk. Not at all plush, Mrs. Parker thought, but it was comfortable, and she was grateful for it. Her water aerobics bag with a change of clothes was in the trunk of her car, and after she’d unpacked, the nurse returned with a goodie basket, filled with snacks and soft drinks, wrapped in colored cellophane.
Anthony Parker with Sandra on prom night in 1971 and with their first child, Kim, in 1973
CHAPTER 4
Moore didn’t stay long in Albany. He knew the fight to overcome the competition from Palmyra would always be ugly. Closer to the end of his career than the beginning, he didn’t have the energy for it. But he knew someone who did, his 34-year-old protégé, Joel Wernick. The two men had met when Wernick was a star right guard on his high school football team in Fort Smith, Arkansas, and worked as a groundskeeper at the hospital that Moore ran. Wernick was brash and competitive, Moore told me, and he encouraged him to go to business school and pursue a job like his.
Wernick took Moore’s advice and became part of a growing number of hospital administrators who’d been trained in business, not medicine. “They were the kind of men — and the vast majority of them were men — who would walk into a room with a pregnant woman and immediately know how much her care was going to cost, rather than the kind of person who could walk into that same room and know immediately what care that woman would need for a safe delivery,” said Richard Ray, a former Phoebe vice president. “They’re both important, but they have different priorities.”
In 1988, Moore recommended Wernick to the Hospital Authority of Albany-Dougherty County, whose nine members approved Phoebe’s spending and operations. From the moment Wernick arrived in Albany, his No. 1 priority was to get rid of Palmyra. He had a powerful ally in the chair of the authority, William Harry Willson, who would hold the position for 31 years. A Harvard Business School graduate, Willson had converted his family’s pecan farm into a successful mail-order business, helped found a local bank and became the city’s leading philanthropist.
Albany’s economy had shifted from agriculture to industry. In 1968, Firestone had opened a factory that employed some 1,600 workers. Procter & Gamble had built a paper products plant in 1973. Within the city’s white establishment, old and new money were vying for influence. Willson and Phoebe represented the old, Palmyra the new. To hear Phoebe’s supporters explain it, Palmyra was driven by racism and greed. Not only did it provide scant care to the poor, but it had no obligations to invest any of the money it was making off of Albany into Albany. Meanwhile, as a public hospital, Phoebe was legally obligated to serve the poor, and in the years when the hospital ran a deficit, the county’s taxpayers were on the hook to make up the difference.
Willson moved to make Phoebe a business, too. Among his first instructions to Wernick was to reach out to Palmyra’s parent company and offer to buy it out. When the Hospital Corporation of America turned him down, they decided that the only way Phoebe could compete was to expand, and the only way it could expand was to change its governance.
The two persuaded Dougherty County to relinquish oversight of Phoebe and transfer it to a private management company that would also finance its operations. Under the new structure, the county would retain ownership of the actual building but lease it to the new entity for $1 a year.
That lease still stands as the county’s only leverage over how the hospital is run. County officials can revoke it without warning, although the conditions of the lease leave a lot to Phoebe’s discretion. It broadly requires that Phoebe provide quality care to the community at a reasonable cost — without defining what that means — that it spend 3% of its revenue on free and subsidized care for the poor and that it uphold Phoebe’s founding promise to treat all people, no matter their ability to pay.
Hospital authority chair William Harry Willson, left, and Phoebe CEO Joel Wernick in 1988. Courtesy of Phoebe Putney Memorial Hospital The construction site for Phoebe’s medical tower two years later.
Courtesy of Phoebe Putney Memorial Hospital
With that move, Phoebe Putney Memorial Hospital became the centerpiece of the Phoebe Putney Health System. Controlled by Wernick, the health system was now free to pursue business ventures in the wealthier suburbs outside the county limits with the same tax-free status as before but without the same burden of public scrutiny.
Under Wernick and Willson’s leadership, the hospital authority approved hundreds of millions of dollars in bonds for the construction of new clinics, office towers and medical wings, including some that weren’t in Dougherty County. Rather than staging hallway tirades to get doctors to refer their paying patients to Phoebe, Wernick bought their practices. He lobbied to prevent Palmyra from obtaining a state license to deliver babies by using Georgia’s strict certificate-of-need provisions, which put limits on the kinds of health care services that can be provided in any one market.
The laws are meant to prevent massive chains from squeezing out smaller hospitals, but in practice they often stifle the competition. Wernick refused to negotiate rates with managers of factories who complained that the costs to insure their workers in Albany were higher than in other cities. When Blue Cross, Georgia’s largest health insurer, moved to include Palmyra in its health care plans, Wernick threatened to withdraw from the network if it went ahead with the deal. It did not.
In 10 years, Wernick dramatically reshaped Phoebe from a small community hospital in a small city to a behemoth hospital system spread across the state. In 1998, a decade after Wernick arrived, The Wall Street Journal reported that the hospital’s profit margins were double the national industry average. Along the way, though, he had made enemies. In 2003, Phoebe’s chief of surgery and a local health care accountant started sending a series of anonymous faxes to businesses, accusing Phoebe and Wernick of an array of excessive and predatory behavior. The faxes, called Phoebe Factoids, were drawn from public records and leaks. A lot of the allegations they made were true — that Phoebe paid its executives high six-figure salaries; that it treated the members of its board of directors to all-expenses-paid trips to Europe and the Caribbean; and that it employed aggressive measures to collect medical debts from the poor. But the information was couched in so much spin and crude innuendo that it wasn’t easy to tell what was accurate and what wasn’t.
A Phoebe Factoid critical of Wernick and the hospitalObtained by ProPublica
For months, the Factoids held Albany in thrall. Wernick used his connections in the district attorney’s office — led by a Putney descendant — and a former FBI agent to help him investigate who was behind them. Once he knew who the authors were, Phoebe sued one of them for defamation. They brought their own suits against Wernick and Phoebe, accusing them of retaliation. Each side denied the allegations.
Eventually the faxes stopped, and the lawsuits were dismissed or dropped, but not before attracting attention from state and national media, which, in turn, got the attention of Iowa Republican Sen. Charles E. Grassley. The chair of the Senate Finance Committee, he was launching an investigation into whether nonprofit hospitals like Phoebe were giving enough back to their communities to justify what they were receiving in tax breaks.
The committee released its findings in 2006, and they were devastating. Among the 10 hospitals that answered the senator’s questions, eight of them submitted information about the amount of free and discounted care they provide to the poor. According to the committee, Phoebe’s terms were the least generous. It offered free services only to people whose income was under 125% of the poverty line and discounted care to those below 200%. Under those terms, a single mother with two dependent children who earned more than $21,000 a year would not qualify for free care. The other seven hospitals covered patients whose income was at least one and a half times that much.
Even more damning was how aggressively Phoebe pursued patients with medical debt. The hospital told the committee that it had filed lawsuits against more than 1,000 people during the previous five years and that nearly 40% of those suits involved people who owed less than $500.
Decades later, when I spoke with Dean Zerbe, who led the Grassley investigation, he got worked up again about Phoebe’s debt collection practices. “They weren’t doing that because they genuinely expected to collect $500,” he said. “When hospitals go after people like that, it’s because they don’t want them to come back.”
One of the many Phoebe billboards in AlbanyKatie Campbell/ProPublica
Three former executives at Phoebe told me that the Grassley report rattled Wernick, because he couldn’t disparage the findings as a “terrorist conspiracy” the way he had done with the Factoids. It wasn’t the only public relations hit. The Albany Herald published an accounting of the properties the hospital was acquiring in the downtown historic district, raising questions about the drain on the county’s property tax base. In 2006, The Associated Press reported that Phoebe had used its relationship with the county government, which has the power of eminent domain, to force a 93-year-old retired domestic worker named Julia Lemon out of her home. The hospital wanted to raze the house so that it could expand a day care center for its employees. A jury ruled in Lemon’s favor.
That same year, the Albany Herald obtained a deposition in which the hospital’s chief financial officer revealed that Wernick’s compensation came with a long list of perks, including a country club membership, six-figure bonuses, an automobile of his choice every three years and a termination agreement guaranteeing that if he was fired for cause, he’d receive three years pay unless he was convicted of a felony. This was on top of a $650,000 salary.
If all that wasn’t enough, in 2009, the battle between Wernick and the authors of the Factoids became the subject of a feature-length documentary. The timing of all the coverage couldn’t have been worse. Plants in Albany had begun to shut down, and thousands of people were being thrown out of work: Bob’s Candies (236 employees); Merck (273 employees); MacGregor Golf (200 employees); Flint River Textiles (230 employees); and, the biggest hit, Cooper Tire, which had replaced Firestone (1,268 employees). On their way out of town, plant managers complained that one of the reasons for the closures was the high cost of health care.
Sandra Morris was a human resources manager at the Procter & Gamble plant, which didn’t close but whose workforce has shrunk over the years. “I was trying to do everything I could to lower our costs,” she told me. But, she added, “I was fighting a monstrosity of a hospital.”
Men playing checkers across the street from the checker club in downtown Albany
Katie Campbell/ProPublica
The battle with Palmyra ended when Phoebe least expected it — when it looked like it had lost. Palmyra applied in 2008 for a license to deliver babies. Phoebe spent millions of dollars, including $8.8 million to the firm of its lead attorney, Robert Baudino, to challenge the request. Palmyra took its case to court, charging Phoebe with a host of antitrust violations, and it won. In April 2010, the 11th U.S. Circuit Court of Appeals ruled against Phoebe and, in remanding the case, recommended that the health system could be held liable for damages amounting to three times the value of any provable harm.
Those who worked with Wernick told me that he saw the ruling as a matter of life and death. The damages Phoebe might have to pay would gut its finances. Just as troubling was that Palmyra’s ability to begin delivering babies would have dealt a significant blow to Phoebe’s ability to compete for patients. I’ve spoken to numerous people about Wernick, and the one quality that both his allies and detractors agree on is that his determination to win was extreme. Where they disagree is about his motives. His supporters say that he operated on the belief that what was good for Phoebe was good for Albany and that it was his commitment to doing right by the community that compelled him to fight as hard as he did. To his critics, he was only interested in building a health care empire, whether that was what Albany needed or not. Lynda Hammond, a former Phoebe vice president, told me that for Wernick “it was all about being the only hospital, not the better hospital.”
Three months after the 11th Circuit’s ruling, Wernick dispatched Baudino to Hospital Corporation of America’s headquarters to discuss, again, Phoebe’s interest in buying Palmyra. The only public records of how the deal was consummated come from the filings made by the Federal Trade Commission, which mounted a legal battle to undo it.
According to those records, HCA seized on Phoebe’s vulnerability and asked for $195 million in cash, which was more than twice Palmyra’s net revenue for the previous 12 months and which the FTC said “far exceeded” other recent hospital deals. HCA demanded that the agreement be kept confidential until it was signed. Also, if the acquisition failed to go through, either because of antitrust challenges or opposition from the hospital authority, Phoebe would have to pay the chain a breakup fee of some $52.5 million.
Wernick presented the terms to the hospital authority a week before Christmas. Baudino, Phoebe’s lawyer, was assigned to represent the authority. As the FTC would later point out in a legal complaint, this put him in the position of both pitching the merger and weighing its merits. He recommended that the authority approve the deal. Seven of its nine members attended the meeting, and they voted unanimously in favor.
Feelings among the residents of Albany, who didn’t learn about the purchase until after it was signed, ranged from confusion to outrage. The Albany Herald quoted opponents to the deal saying that it was “mind-boggling” that the hospital authority would agree to a merger of this magnitude without taking time to do an independent assessment of its potential impact on the cost and quality of care. They accused the members of the authority of conducting themselves as “agents of the hospital” rather than representatives of the public good.
Within months, the FTC sued Phoebe, describing the hospital authority as a “rubber stamp” and the deal as a “merger to monopoly” that would “cause consumers and employers in the Albany region to pay dramatically higher rates for vital health care services.” The agency pointed out that many people in the city were “already struggling to keep up with rising medical expenses.” It added that the merger was also likely to “reduce the quality and choice of services available.”
Over the years Phoebe had done many things to lose the confidence of the community it was supposed to serve, but the purchase of Palmyra — at a huge cost, revealed only at the last minute, without public input or any assessment of its repercussions — was a turning point for many residents.
The hospital authority didn’t call a public hearing on the merger until May 2012, some 17 months after the deal was announced. It attracted an overflow crowd and lasted more than three hours, as one impassioned speaker after another shared their views. “Why did it take the FTC to recognize what you did not — the need to protect our citizens from an overreaching hospital,” asked a resident named Hope Campbell, speaking for many in the room.
In response, Wernick promised that, in order to keep the merger from draining revenue from the county, Phoebe would voluntarily continue to pay what had been Palmyra’s property taxes. Not only would there be no increases in the cost of care, Wernick said, but ending the rivalry between two hospitals would allow Phoebe to streamline services in a way that would reduce costs and broaden its ability to provide the region with “high-quality, affordable and accessible health care.”
He explained that Phoebe Putney Health System had grown to cover 35 counties. As a result, it had to expand to keep up with the demand, and buying a facility was much cheaper and much less disruptive than building one. Phoebe would finally have the space and resources, he said, to address some of the region’s most pressing needs, including establishing a trauma center. And he pledged to convert Palmyra into a medical facility that focused on care for women and children.
The matter of the merger was not settled for five years, and although Phoebe lost the legal battle, it ultimately won. The Supreme Court ruled against the merger, but by then Phoebe had taken control of Palmyra, combining its services and staff and even giving the facility a new name, Phoebe North. The FTC fought another couple of years to find a way to separate the two entities, but it eventually decided that Georgia’s strict certificate-of-need provisions would make it almost impossible for an outside health system to sustainably take over Phoebe North.
Richard Ray, the former Phoebe vice president, recalled being summoned to an executive meeting shortly after the settlement with the FTC was announced. He said that the mood at the meeting was anything but celebratory. The purchase had thrust Phoebe deep into debt. Nobody was sure how the hospital was going to keep its doors open.
Wasn’t the plan to turn Phoebe North into a women and children’s facility? I asked.
“It was clear that no real due diligence on the idea had ever been done,” he said. “We had bought this facility that we couldn’t use.”
How did Phoebe explain that to the public? I asked.
“We knew we couldn’t say that to the public,” he said, “so we really didn’t say anything.”
Rosalynn Almond holding the urn containing the ashes of her sister LaTosha
Almudena Toral/ProPublica
May 27-29, 2022
Just a little more than 24 hours had passed when Mrs. Parker realized that word about her husband’s condition had gotten out. She received a text from someone she and Anthony barely knew, a middle manager in Phoebe’s human resources department. But somehow the woman had heard he was in critical condition and messaged to say that she was praying for him.
“How does she know?” Mrs. Parker wondered. “Had news about Anthony gotten out?
If that wasn’t intrusive enough, the woman stopped by the room. You don’t want to move him to Emory or somewhere? she whispered. Shouldn’t you get him out of here?
It seemed an inappropriate question on so many levels, not the least of which was how little they knew each other. Still, Mrs. Parker was polite. “We’re good,” she responded. “I appreciate your concern, but we’re good.”
Other people might not have a high opinion of Phoebe, but Mrs. Parker did. She was confident its staff was going to save Anthony. She compared it in her mind to when President Donald Trump came down with COVID-19 and had to be rushed to Walter Reed National Military Medical Center. That was an all-hands-on-deck emergency, and the staff at Phoebe, whose senior executives milled in and out of Anthony’s room, had made it clear that this was an all-hands-on-deck emergency, too.
Andrea, the Parkers’ middle child, who was 43 and served as a commander in the Coast Guard, had arrived from suburban Washington, D.C., late the previous evening. So had Richard, a UPS long-haul driver, based in Atlanta, who was 39 and the youngest sibling. None of them doubted that their father was in good hands. They supported their mother, and their mother was going to stick with Phoebe.
That’s what Anthony had always done when others raised questions about the hospital. When doctors shared concerns about staffing issues that were leading to poor patient outcomes, Anthony questioned the propriety of their actions, not Phoebe’s. When friends complained about loved ones dying in Phoebe’s care, he didn’t use his position on the board to press the hospital for an inquiry. He would say he was confident Phoebe had acted appropriately. When he asked Phoebe to invest in Albany Tech’s nursing program and instead it gave money to the predominantly white community college, he stewed privately, but he didn’t raise a ruckus. “They just don’t know they need us yet,” he’d say to his staff. “We’ll be here when they do.”
Mrs. Parker’s loyalties also ran deep. When the spouse of a co-worker had nearly died from an infection she’d gotten after a hysterectomy at Phoebe, she asked Mrs. Parker to help get a letter to CEO Joel Wernick. Mrs. Parker didn’t do it. Who knew whether Phoebe was responsible? she reasoned. It didn’t feel like something she should take to Anthony, much less for Anthony to take to Wernick.
Yes, there was the time years earlier when he was being treated for lymphoma and had been admitted for what was supposed to be a laparoscopic biopsy of a spot that had been detected on one of his lungs. The doctor emerged from the biopsy saying he’d ended up performing major surgery. “Did he just tell me he opened Anthony’s chest?” she said to herself, feeling a lot like she would when Dr. José Ernesto Betancourt told her that her husband had gone into cardiac arrest. The surgeon back then explained that he’d changed plans because he’d had a hard time reaching the section of the lung that he’d wanted to check for cancer and that fortunately he’d found no signs of disease. But afterward, Dr. Parker’s radiation oncologist complained that the biopsy hadn’t been necessary.
Why hadn’t her husband’s doctors communicated with one another? Mrs. Parker wondered. A lawsuit certainly crossed her mind but not her husband’s. He would have never considered such a thing. Not when it came to Phoebe. He’d have a longer recovery, but he’d be fine. His thinking was, “Let’s move on.”
She was praying that her husband would be fine this time, too, that his faith in Phoebe would be vindicated. On Sunday, three days after the ablation, it seemed that might be the case. The cooling period had ended. Dr. Parker’s body was being returned to normal temperature. His three children were in his room, singing along with a recording of the South Carolina State fight song — “Get up for the Bulldogs. Everybody, get up!” — hoping their father could hear them, when suddenly he opened his eyes.
Anthony Parker pinning a corsage on his younger daughter, Andrea, in 1997 and with Andrea during parents weekend at the Coast Guard Academy the following year
CHAPTER 5
Phoebe spending nearly $200 million to buy and then mothball most of Palmyra while so many Albany residents were struggling to pay their medical bills was disastrous for its reputation and its finances. The hospital had paid cash for Palmyra, cobbling together the financing afterward, including arranging for the hospital authority to issue yet another bond — this one for $108 million. The additional debt helped send Phoebe’s expenses soaring from $508 million in 2012 to $576 million the next year.
I spoke with several former Phoebe executives about what things were like during that time. They told me that conditions were bleak. One recalled Joel Wernick, who’d now run the health system for 25 years, spending millions of dollars on a communications expert to come up with a branding campaign. “We had soiled beds, waiting rooms with holes in the chairs, mounting sepsis issues and had just laid off 200 qualified nurses,” he recalled, “but we had a new logo.”
A former vice president at Phoebe showed me an email chain that she’d saved from around that time. It had been written under the subject line “ICU Morale.” The emails captured a conversation among a group of intensive care nurses who were encouraging one another to try to make the best of the conditions because there wasn’t much else they could do.
“Money problems in the hospital (despite all of our opinions) have dictated that cutbacks are necessary,” one of the nurses wrote. “People and family are going to die, our patients are going to die, sometimes quick… sometimes not … sometimes despite everything we do.” The nurse went on. “People are going to be treated wrong, people will suffer, work will not be the best at times,” he wrote. “We will continue to feel underpaid no matter what job, company or title we attain.”
One of the nurse’s colleagues thanked him for speaking up. A supervisor encouraged everyone on the email chain to try to make the best of a bad situation. However, there was a long response from a nurse whose positivity was spent.
She wrote that during a typical shift in the ICU, it wasn’t unusual for a single nurse to manage three critically ill patients at a time, while guidelines advise only being responsible for one to two. She described how doctors ignored late-night calls, leaving her and her colleagues scurrying on their own to figure out how to save patients whose vital signs were crashing. She recalled running out of essential supplies and having to spend hours on the phone — and away from her patients — to get them restocked.
She despaired about having to answer questions from patients and families about “why something wasn’t done or checked, when you’ve been doing your best just to stay afloat.”
It’s easy to talk about keeping a positive attitude, she wrote. “But when you’re hit with tidal wave after tidal wave, night after night, even the most faithful, positive person will start to waver.”
A Phoebe spokesperson said the emails “represent the opinions of a few individuals, not facts.” At the time, he said, Phoebe “was not under undue financial strain and never prioritized financial considerations over quality and safety.”
The conversation in those emails resonated because I’d pored over hundreds of pages of Phoebe’s financial records. Revenue from patient stays was flat. The former Phoebe vice president told me that Palmyra’s patients were so upset by the merger that those who could afford to travel for health care, which often included people with decent insurance, went out of their way not to go to Phoebe. Providing care for the poor and uninsured became an even bigger burden. The amount of bad debt that Phoebe accumulated because patients weren’t paying their bills increased from $16.5 million in 2012 to more than $121.7 million in 2018.
Despite Wernick’s promises, the cost of care at Phoebe increased immediately after the merger, and, a year later, so did the cost of health insurance. An Atlanta Journal-Constitution examination in 2013 of the online market that had been established by the Affordable Care Act found that a middle-tier insurance plan for a typical 30-year-old consumer in Albany was the highest in the state.
The following year, The Washington Post published a national study of the online marketplace. It found that southwest Georgia was one of the most expensive health insurance regions in the country. The only places with higher premiums were in the areas around the Colorado resort towns of Vail and Aspen.
“If Lee Mullins lived in Pittsburgh, he could buy mid-level health coverage for his family for $940 a month,” the Post story opened. “If he lived in Beverly Hills, he would pay $1,405. But Mullins, who builds custom swimming pools, lives in southwest Georgia. Here, a similar health plan for his family of four costs $2,654 a month.”
What that meant, I was told over and over again in Albany, was that the poor and uninsured stopped seeking routine care, and the rates of treatable illnesses began to climb.
I sought out Wesley James, a sociologist at the University of Memphis, whose research focuses on health, mortality and life expectancy in rural parts of the country, and asked him to analyze mortality rates for Dougherty County over the past 50 years. Drawing on Centers for Disease Control and Prevention data, he found that for most of that time, the county’s diabetes mortality rate had tracked closely with the rates for the state and nation. In the decade after the merger, however, it leaps off the charts like rocket trails, going from 36 to 76 per 100,000 people.
James told me that it wasn’t unusual to see modest upticks in poor, rural communities that have experienced steep population decreases and been hit by economic turmoil but that he’d rarely seen spikes as high as the ones he’d recorded in Dougherty County.
The Rate of Deaths from Diabetes Was Far Higher in Dougherty County than in Georgia or the United States
Source: Centers for Disease Control and Prevention WONDER Database
None of this affected Wernick’s compensation. In 2017, the year he turned 63, the health system provided him with a $6 million retirement package, in addition to his more than $1.1 million in salary and deferred pay. In 2018, Wernick’s last full year as CEO, his earnings per bed were more than twice as much as that of the CEO at the Mayo Clinic, one of the top-rated health systems in the country. In the two years following his departure, Wernick was paid almost $2.8 million, because the board had extended his contract in case it wasn’t able to find a replacement.
If Wernick had made peace with his opponents by the time he left, he gave no sign of it in the exit profile that the Albany Herald published. “The kind of unwarranted criticism I was subjected to never really hurt my pride, as it was intended to do,” he told the paper. Nor, he said, did it diminish his commitment to Albany. “This is a place where thousands live, and millions wish they could,” he said. “I intend to continue contributing to it.”
Eight months later, he moved to the other side of the state.
May 29, 2022
When Dr. Parker opened his eyes, his pupils rolled upward. He didn’t say anything. His body was clenched and trembling as if he’d felt a jolt of electricity. The entire episode only lasted a few seconds, but that was the signal Mrs. Parker and her family had been praying for — the “‘Grey’s Anatomy’ moment” she had told everyone was going to happen. Anthony was coming back. He would wake up. He might not remember who they were right away, but he’d wake up.
There were so many big things ahead for him. His and Mrs. Parker’s 50th wedding anniversary. Andrea’s retirement from the Coast Guard. His newly elected position on the Rotary Club board. And the launch of Albany Tech’s partnership with Phoebe that would double the college’s nursing enrollment. The project marked the culmination of Dr. Parker’s effort to transform the image of his school from one that gave students manual skills to one that turned them into professionals.
Mrs. Parker remembered the naysayers — people who never believed it would happen or believed it shouldn’t. At lunch one day, William Harry Willson’s wife, like her husband, a major benefactor of the hospital and community, took Dr. Parker playfully by the hand and cautioned him against trying to turn the school into something for which it was not intended. Willson didn’t say it in so many words, but the message Dr. Parker took from her was: “Don’t forget what your school is there for. Teach those kids to use their hands, not their brains.”
She remembered her husband repeatedly asking the hospital to support Albany Tech’s nursing program and Wernick regularly turning him down. The one time Phoebe did give a large donation, Wernick insisted that Dr. Parker keep it anonymous. It ticked Dr. Parker off. It felt to him like the same kind of hush money that Strom Thurmond, the segregationist senator from South Carolina, had secretly sent to the Black child he’d fathered but never publicly acknowledged.
Dr. Parker never let on publicly how he really felt about Wernick’s request, and he told his wife not to do so either. He did what he’d always done: accepted the gift, privately thanked the hospital and made the most of the money without saying where it came from.
Anthony Parker with his children in 1986
CHAPTER 6
Before coming down with COVID-19, LaTosha Almond earned about $9 an hour working for a company that laundered the hospital’s linens. Her health habits were typical of the poor and uninsured. She couldn’t afford regular checkups. She sought medical help — usually by going to the emergency room — only when she was sick, which was a lot. She was raised in the tiny town of Cotton, where her mother, grandmother and great-grandmother had worked on a farm, both in the fields and in the kitchen.
Almond was the youngest of six children, raised by a mother who struggled with mental health and a father with a violent temper. She spent her childhood bouncing between a troubled home and foster care and her adulthood bouncing between dead-end jobs.
By the time she was about to turn 42, she was morbidly obese, diabetic and in the early stages of congestive heart failure. If that wasn’t enough to make her a perfect target for COVID-19, she’d been hospitalized with the flu just months before the start of the pandemic.
But it wasn’t COVID-19 that killed Almond. Her medical records show that she died from cardiac arrest and severe brain damage, which her family believes was caused by a series of alarming and inexplicable lapses by medical staff at Phoebe. Three nurses, who were either involved in Almond’s care or had detailed knowledge of it, agreed.
According to her medical records, Almond was admitted to Phoebe with COVID-19 in early April 2020 and was hospitalized there until June 1. She announced that she was being discharged on Facebook. Her voice was weak and raspy, but her mood was upbeat. She’d not only beaten COVID-19, she’d shed 100 pounds. “I’m getting fine, girl,” she said to one friend who typed a comment congratulating her. “Fine, fine, fine.”
That wasn’t all. “My life has changed,” she went on. “I feel better about myself. No matter what nobody say, you can’t bring me down.”
The day after Almond arrived home, her mother, Tersas Laster, detected an awful stench coming from her daughter’s bedroom.
“I went in and asked Tosha, ‘What’s that smell, baby?’” Laster said. “She told me, ‘Ma, it’s that wound.’” Almond had a severe bedsore on her lower back. Laster described it as big as a dinner plate and so deep that she could see her daughter’s bone. “It was pouring out yellow and gray pus,” she said. “Smelling like a dead carcass on the side of the road — that’s how they sent my baby home.”
A home health nurse whom Phoebe had assigned to follow up with Almond instructed Laster to get Almond back to the hospital. “The nurse told me they should have never discharged my baby with that wound,” Laster said. Almond’s medical records indicate that she underwent emergency surgery to debride the wound. The surgeons also performed a tracheotomy because her airway had narrowed, making it hard for her to breathe.
Almond spent an additional three weeks at Phoebe and was discharged on June 25 with a tracheostomy tube that required regular cleaning to keep her airway open. Laster only attended school until the eighth grade and acknowledged to me that she doesn’t read or write well. She said that Phoebe did not teach her or her daughter how to manage the trach, as required for discharge. According to Almond’s medical records, she was rushed back to the emergency room three times after the trach became clogged.
The first time was on June 27. Records indicate that doctors in Phoebe’s emergency room removed “a large mucus plug” and sent her home. She was back in the ER again on July 12, with another plug, which doctors removed. A few minutes before noon the next day Almond was back at Phoebe for the third and final time.
“Patient arrived in cardiac arrest, which seemed secondary to respiratory arrest,” her medical records said. Her heart had stopped beating for nearly 15 minutes before doctors were able to revive her, according to the records. They removed her trach and put her on a ventilator and tried treating her with hypothermia — cooling her body to give her brain time to recover. However, the records said, the heart attack had caused too much damage. Almond was not exhibiting “any purposeful activity or signs of brain activity.”
She was pronounced dead shortly before 10 a.m. on July 15. Her sister Rosalynn Almond said the way Phoebe had treated Almond was “inhumane,” adding, “What kind of doctor sends a person home with an open wound like that?”
Citing privacy protections, a Phoebe spokesperson said he could not comment on the specifics of Almond’s case but added “we believe Phoebe provided appropriate care.”
She and her mother attempted to find a lawyer who would represent them against Phoebe, but no one would take their case. Georgia, like many other states, enacted an emergency immunity law that shielded health care providers from civil liability in COVID-19 cases, except when plaintiffs could meet the nearly unattainable standard of proving gross negligence or willful misconduct. Almond was classified as a COVID-19 death, even though that wasn’t what killed her.
“I feel like if they’d have done what they were supposed to, my child would be here now,” Laster said. “I wouldn’t have had to bury my baby.”
Two of Almond’s home health nurses told me that in the chaos of COVID-19 families were not always getting the supplies and the training they needed to properly manage trach patients, because Phoebe either didn’t have the resources or didn’t provide them. Another nurse, who knew of Almond’s case but was not assigned to it, said she scoured Amazon every day looking to buy inner cannulas, the tubes that are placed inside the trach, that were the right sizes for her patients’ needs. She said that cannulas were so hard to find that she asked patients to reuse them more times than standards advised, and she reluctantly asked for them back from patients who had recovered.
A Phoebe spokesperson said the hospital had “no recollection of anyone ever reaching out to complain about a lack of home health supplies or to indicate they were scouring Amazon in search of proper supplies.”
Cases like Almond’s had me wondering how well Phoebe had tended to its patients before the pandemic. In 2012, the year after it acquired Palmyra, Phoebe was rated one of the worst hospitals in the country by a coalition of large health insurers and leading patient safety experts known as the Leapfrog Group. The group’s members had been alarmed by reports that across the country 200,000 people were being killed or injured each year by medical mistakes and wanted to provide patients a way to evaluate their health care options.
The Leapfrog Group began giving letter grades to hospitals based on information it gathered from the institutions themselves and on an analysis of public data from the Centers for Medicare & Medicaid Services. The Albany Herald reported that part of the reason for Phoebe’s poor first grade — it got an F — was that Leapfrog gave the hospital only 5 points out of 100 for ICU physician staffing. The hospital’s senior vice president of medical affairs told Georgia Health News that he was “troubled” by Leapfrog’s methodology, which he described as “inaccurate and misleading.” The score resonated with me because it tracked with what I’d read in the email exchange I’d obtained and with what I’d been told by several nurses who worked at Phoebe during that time. They said that the ICUs back then were not staffed 24 hours and that getting critical care physicians to respond to emergencies was hit or miss.
In 2015, CMS developed a star system to rate the quality of care at the nation’s hospitals, based on reports of hospital-acquired illnesses, readmissions, emergency room wait times and overall patient satisfaction. The ratings, while imperfect, are widely cited among industry analysts because of the agency’s regulatory authority.
According to the system, one star indicates poor performance, and five indicates excellence. Phoebe received one star when the first reports were published in 2016. CMS rated Phoebe below national averages in the most crucial categories, including hospital mortality rates, the rigor of the safety measures practiced by its staff, the numbers of preventable readmissions and general patient satisfaction. The hospital’s Medicare reimbursements were docked because of high rates of hospital-acquired infections and rates of readmission.
Phoebe responded by pointing to one of the glaring weaknesses in the CMS rating system, which is that it puts hospitals that serve predominantly poor and uninsured populations on equal footing with hospitals in wealthier communities. Dr. Steven Kitchen, the chief medical officer, said, “The ratings given to hospitals like Phoebe show that this simple star system does not accurately represent the quality or complexity of care provided by teaching hospitals.” However, to put Phoebe’s score in context, 96% of the nation’s hospitals rated by the agency scored higher. All the other hospitals within a 100-mile radius of Albany received three or four stars. Only four other hospitals in Georgia received one star, including Grady Memorial Hospital, a publicly run, 634-bed safety-net hospital in Atlanta.
A banner in the lobby of Phoebe Putney Memorial Hospital announcing it received an A rating in 2022 from a patient safety group. Its rating has since dropped to a C.Almudena Toral/ProPublica
The Georgia Department of Community Health examined Phoebe’s surgical records. It found two separate incidents of surgeons who operated on the wrong section of a patient’s spine and another where doctors operated on the wrong hip. Home health nurses, according to the inspection reports, were not keeping adequate service records, making it hard to scrutinize whether patients were receiving the medications and therapy they needed. Inspectors obtained audio recordings that showed Phoebe’s physicians refusing to accept critically ill and injured patients who had been referred by emergency rooms at smaller facilities. One case involved a patient with a serious head injury, whom Phoebe’s neurosurgeon dismissed as a serial drunk.
CMS gave the hospital a two-star rating in 2017. Then in 2018, under enormous pressure from the American Hospital Association, one of the most powerful lobbies in Washington, CMS paused its rating system to adjust its metrics. That year, state officials inspected the death of a Phoebe patient who’d arrived at the emergency room complaining of weakness and persistent diarrhea. The hospital had initially reported the death as a freak incident. However, the state’s investigation revealed that staff either ignored or silenced alarms that indicated the patient was in distress 19 times until relatives discovered the patient unresponsive. Inspectors found that the patient was “down for possibly thirty (30) minutes before CPR was initiated.”
A Phoebe spokesperson said any health system of its size “will sometimes have patient outcomes that are not optimal. It is the responsibility of every hospital to learn from those cases and do everything in their power to do better the next time.”
When the results of the new CMS system were back online in 2019, Phoebe received one star again. It had a one-star rating in 2020, when Albany was hit by COVID-19 and patients like Almond flooded in for care. Phoebe is still struggling to address the issues raised by Almond’s case. In 2023, it was penalized for a high readmission rate, which tracks patients who return to a hospital within 30 days after their discharge. That metric can serve as an indication that they may have been released too early or without proper instructions. According to that data, Phoebe also continued to have a problem with bedsores in 2023. The hospital has two stars today, which places it among the bottom 30% of all CMS-rated hospitals in the country.
An email sent this year from an ICU nurse to hospital leaders suggests that some of the same staffing issues nurses complained about more than a decade ago persist.
The nurse described staffing levels at Phoebe’s ICUs as a “crisis.” She wrote that charge nurses, who supervise their units and therefore are not supposed to participate directly in patient care, routinely manage two patients. Nurses who should be handling no more than two patients were often assigned three. “This is not only unsafe for patient care, but also unsustainable for staff morale and retention,” the nurse wrote.
“If immediate action is not taken to correct the staffing crisis, the hospital will not only see a decline in patient outcomes,” she continued, “but also a significant loss of experienced ICU nurses who cannot continue to work under these unsafe conditions.”
A Phoebe spokesperson disputed the nurse’s charge, saying, “We have not had a staffing crisis in our ICUs.” He added, “We staff for the volume and acuity of our patients and currently do not have any issues with staffing in our critical care unit.”
Downtown AlbanyKatie Campbell/ProPublica
June 1, 2022
On Wednesday, Mrs. Parker’s sixth day sitting vigil, Dr. James Palazzolo introduced himself, explaining that he was now the critical care specialist on call. Mrs. Parker had seen Palazzolo around the hospital over the years. She’d been put off a bit by his formal bearing until a close friend who had been Palazzolo’s patient told her how much she liked him. Palazzolo, in fact, was warm, but he hadn’t come to bring Mrs. Parker good news. He wanted to know whether Dr. Parker had signed a living will that explained how he wanted her and his doctors to manage the end of his life, in the event that he was unable to tell them himself.
Mrs. Parker froze for a second and then asked Palazzolo what he meant. She hadn’t been preparing for the end of her husband’s life. She’d been preparing for a “Grey’s Anatomy” moment. He seemed so close. He’d already opened his eyes.
Palazzolo asked her if she had spoken with a neurologist.
Mrs. Parker shook her head. Should she have? she wondered to herself. How was she supposed to know that? Palazzolo said that her husband was being seen by a neurologist and that he’d arrange for her to meet with him. She didn’t even know a neurologist had been involved in her husband’s care. Palazzolo explained that he wanted her to get a specialist’s opinion of her husband’s condition, but his reading of the medical records suggested that Dr. Parker’s brain damage was extensive. He wasn’t getting progressively better, and it seemed unlikely that he would.
Mrs. Parker suddenly didn’t know whom to believe. The previous doctors had told her that they were going to give her husband’s brain time to rest and recover and then would wake him. No one had raised the possibility that he wouldn’t recover. “Anthony opened his eyes,” she reminded Palazzolo.
That was a reflex, a spasm, the doctor said. It wasn’t a sign of brain activity. There hadn’t been any meaningful sign of brain activity since the surgery, he told her.
Mrs. Parker stood in stunned silence. Why hadn’t anyone told her that? She didn’t want to think the worst of Phoebe, that the hospital had been deliberately keeping the truth from her, but she couldn’t help herself.
Palazzolo asked her whether she and her husband had ever discussed what they would want the other to do under these kinds of circumstances. He encouraged her to summon her children to discuss next steps, and he repeated that he would make sure to have a neurologist meet with her before the end of the day.
Andrea, the Parkers’ middle child, arrived at the hospital soon after. They were sitting in a waiting area outside of Dr. Parker’s room when Dr. William Garrett, the neurologist on call, appeared in a white lab coat and bow tie. He invited the Parkers to talk in his office. The space, little bigger than a closet, was cramped and cluttered. Garrett sat behind a desk and turned his computer monitor toward them, calling up different models of the brain, and proceeded to show images and charts that explained the various kinds of damage that could have been caused during the four to 14 minutes Dr. Parker’s heart had stopped beating.
Andrea, taking notes, wrote, “4-14,” and then looked up. “We thought it had only been a few minutes, five at the most,” she said. “Now you’re saying it could have been 14?”
The neurologist told her that the records he’d seen from the day of the procedure weren’t clear, so he couldn’t be sure, but it looked to him like it might have taken much longer than five minutes to restore her dad’s heartbeat. Then he turned back to his models, describing something about inconclusive clinical trials, which made it hard to assess certain kinds of damage to the brain and the chances for recovery.
Mrs. Parker’s face went blank again. She was unable to absorb most of what Garrett was saying. What did those images on his computer have to do with Anthony? she thought to herself. Why is this man speaking to me like I’m one of his med students?
Andrea was also losing patience. She was scribbling the doctor’s words — “extensive posturing in all extremities,” “flexor response at day six,” “reminiscent of diffuse expression” — but she had no idea what they meant. When he told her that there was no single data point that he could use to provide a conclusive prognosis, she stopped him. “I know neurology isn’t an exact science,” she said, “but I don’t want to talk about models.”
Pointing at herself and then at her mother, she went on, “I want to talk about this case — about my dad, her husband.”
The doctor said he wished he knew more about the extent and severity of the brain damage, but he hadn’t been able to perform a scan because Phoebe didn’t have a mobile MRI machine and her dad was too unstable to be moved.
Based on the little he knew, Andrea asked, what would he do if this was his loved one?
Garrett turned away from his computer and toward Mrs. Parker. He told her that he was married to a sweet, beautiful woman whom he loved dearly, but that he didn’t think it would be useful to speculate on what he’d do in Mrs. Parker’s shoes. He told her that his clinical assessment of her husband’s condition was the same as Palazzolo’s. It wasn’t getting progressively better. As for what she should do, he said perhaps she wouldn’t have to do anything. Sometimes, he told her, God makes the decision for us.
The room went silent. Mrs. Parker could feel her daughter about to explode. Why was this doctor talking in circles? Was he hiding something? Was Phoebe hiding something? Suddenly its embrace seemed more like a trap.
Anthony Parker soon after he became president of Albany Technical College in 1995
CHAPTER 7
Scott Steiner, who succeeded Joel Wernick as the CEO at Phoebe, was happy to cooperate with my reporting when I was focused on the hospital’s response to COVID-19. But he was less enthusiastic when I told him that my focus had shifted to the health system’s relationship with Albany. He explained why when I met with him in his office, and he told me about the first time he sat with Wernick.
It was 2018, and the office looked different back then. Wernick, he said, kept it like a bunker — dimly lit with a dark carpet, hunter-green furniture and thick velvet drapes that were drawn shut. Steiner had been told that Wernick barely left the office during work hours anymore and that he never opened the drapes. According to Steiner, when he asked Wernick why not, the CEO looked at him with a “little wily smile” and said, “For fear of being shot.”
Leading Phoebe during COVID-19 hadn’t been easy, Steiner said, but distancing himself from his predecessor was even more challenging. In his first year, he’d held 570 meetings with community groups, churches and medical practices, many of them taken up with decades-old grievances — what Steiner described as the “ghosts that will outlast me.”
Steiner, who is 57, grew up in St. Louis. His mother was an intensive care unit nurse, his father an executive at a printing company. He received his MBA from nearby Webster University. Before joining Phoebe he had been the CEO for a group of Detroit hospitals, owned by Tenet Healthcare, the second-largest for-profit health system in the country. It was a miserable experience, he told me. He oversaw five layoffs in his first two and a half years. Then he had to manage the fallout from a series of newspaper stories that revealed how some of the hospitals had nearly lost their licenses after doctors filed complaints about dirty and broken surgical instruments.
Three prominent cardiologists claimed that the health system fired them for making those complaints public, and two filed a wrongful termination suit against Tenet and Steiner. The cardiologists eventually won a $10.6 million award. (Officials at Tenet did not respond to multiple requests for comment.) Steiner didn’t want to talk about his role in the matter when we met, except to say that the turmoil made him open to calls from a headhunter who told him about the opportunity at Phoebe.
“I didn’t think places like this existed anymore,” he told me. Compared to the “shit show” in Detroit, he said, Phoebe Factoids, the anonymous fax campaign against the hospital that consumed Albany in the early 2000s, seemed like “a lot of external nonsense.” Phoebe’s future direction would ultimately rest with him, not distant corporate overlords. All he had to do was get people in Albany to trust him, to put the past behind them. “What I’ve tried to say to people is, it’s a new chapter.” he told me. My reporting, he said, threatened to stir up old tensions.
The Westgate neighborhood of AlbanyRoss Landenberger for ProPublicaNorthwest Albany
Ross Landenberger for ProPublica
He knew such tensions were already stirring well before I came along. He’d heard them firsthand during his numerous meetings with the community. Mayor Kermit “Bo” Dorough, who’d been a critic of the hospital since the Factoid days, was threatening to commission a study of health care costs. And in early 2020, nearly a year after Steiner’s arrival and weeks before COVID-19 hit the city, The Albany Southwest Georgian, a weekly Black newspaper, published the official portraits of Phoebe’s executive team across its front page. Most were people Steiner had inherited. None was Black.
The racial composition of Albany’s political hierarchy had shifted in the previous 20 years. The city’s manager and police chief were both Black, and so was the county district attorney and chief judge of the county court. Until Dorough’s election as mayor in 2019, African Americans had held the office for four straight terms. The majority of the members of the hospital authority was Black. Among them was a retired civil rights lawyer named Nyota Tucker, who was alarmed by the Southwest Georgian’s front page. Why were there no Blacks on the health system’s executive team, she asked Steiner during one authority meeting.
A front page of The Albany Southwest Georgian from February 2020 showing Phoebe’s executive team
The Albany Southwest Georgian
Bespectacled and silver-haired, Tucker, 76, carries herself with quiet reserve. As a teenager, she was one of six students — all girls — to integrate her hometown’s high school. She went on to become the first African American woman to graduate from the University of Georgia School of Law. Afterward, she moved to Albany to work for Georgia Legal Aid, where judges in her first cases demanded she provide proof that she was a member of the bar. She left Albany for a few years to join the NAACP Legal Defense Fund in San Francisco and then returned, eventually becoming a member of the faculty at the historically Black Albany State University and later its chief counsel.
She didn’t know much about the health care system or how it worked when she agreed to serve on the hospital authority in 2017. She saw volunteering as a way to stay active after she retired and to serve the community. “The authority was not known to cross Phoebe,” Tucker told me. Quickly, she established herself, according to one board member, as the “contrarian in the room” — the person who said what “nobody else wanted to say.”
In late 2020, Steiner added Dr. Dianna Grant, a Black physician, to his executive team. The next year, the hospital authority elected its first African American chair, a businessman named Glenn Singfield. When I interviewed Singfield, he made clear he was also aware of the authority’s history as a rubber stamp. He told me he wanted to break from the days when the authority consisted of people who’d been “handpicked” by Phoebe to “do the hospital’s bidding.” He said, “I can assure you those days are over.”
There were reasons to be skeptical. The authority relied on Phoebe for its funding as well as for its administrator and lawyer. The hospital managed the authority’s website and routinely hosted its meetings in the Phoebe board room. And five out of its nine members were doctors or had other financial ties to Phoebe, including a former mayor who had received numerous campaign contributions from Phoebe executives and Singfield, who owned a construction company that had contracts with the health system.
Still, Tucker wanted to believe Singfield and wanted to believe that Steiner would lead Phoebe in a new direction. But she soon found herself at odds with him. As the pandemic loosened its grip on Albany, she resurfaced a proposal she had made the year before to have the authority hire a consultant to assess whether the hospital was meeting its lease obligations to provide safe and affordable care to the community.
The previous review had been done in 2012, before the advent of Obamacare and Georgia’s decision not to expand Medicaid. The assessment would allow the authority to get a better sense of those policies’ effects. Besides, she was new to the authority, and Steiner was new to the health system, and it seemed like a good way to get a baseline understanding of where things at the hospital stood so they could see where things could be improved.
Steiner told the authority he was not opposed to a review but wondered whether hiring an outside consultant was a good use of precious resources. He said that Phoebe would provide any information the authority requested to assess how well the health system was managing the hospital.
Tucker argued that hiring an outside firm was the only way to get an assessment that was “free of any hidden agendas,” even though the money for the review would ultimately come from Phoebe. Since several members of the authority, including herself, had little to no experience in health care, they might not know what questions to ask, she said.
Retired lawyer Nyota Tucker sat on the hospital authority board from 2017 to 2022.
Alyssa Pointer for ProPublica
The authority voted in favor of hiring outside consultants. They presented their findings at a meeting in May 2021. Marvin Laster, president of the city’s Boys and Girls Club and a member of the hospital’s board of directors, attended. Tucker was surprised. Laster hadn’t ever come to an authority meeting that Tucker could remember, but she knew him — she was on the club’s board — and she was happy to have a friend in the room.
The analysis read like an exercise in damning with faint praise. Phoebe, the consultants wrote, was “committed to providing quality care” and was “delivering comparable or better quality than its peers in many areas.” However, when they zeroed in on the seven metrics that make up the Centers for Medicare & Medicaid Services’ star rating system, they found that Phoebe “currently ranks below the national average in five of the areas, including mortality, readmission, patient experience, effectiveness of care and timeliness of care.”
While Phoebe had spent hundreds of millions of dollars in building, buying and equipping new facilities, the consultants pointed out, its investments in the maintenance and modernization of the old buildings — which the consultants emphasized were among the health system’s core obligations to the county — were “consistently on the lower end” of its peers.
The hospital’s financial margins were comparable if not better than its peers, the report concluded, but it relied more heavily on long-term debt to fund its operations — an indication that Phoebe still hadn’t fully absorbed the cost of the Palmyra merger 10 years earlier.
As for the percentage of gross revenues that Phoebe spent to help the poor, the report found it had a “lower charity/indigent care percentage than its local, regional and national peers, in all years except 2015.” And finally, the report found that Phoebe’s cost of services “are, on average, higher than local, regional and national peers.” In short, the issues that had bedeviled the hospital’s relations with its community — the quality of care, cost of care and its outreach to the poor — hadn’t changed.
When the consultants concluded their presentation, the first questions to arise were less about the findings and more about what to do with them, according to two authority members attending the meeting.
Singfield was emphatic, Tucker said. He declared the report was “not for public consumption.” (Singfield did not respond to questions about the meeting.) Another member of the authority told me that everyone saw the finding regarding cost of care as “the big elephant in the room.” The member said, “There wasn’t any way to sugarcoat it.”
Steiner did not offer an opinion, but Laster weighed in. It was understood that he was speaking on Phoebe’s behalf, according to two members of the authority. Laster said that even though most of the assessment was upbeat, the information about the high costs of care could hurt the hospital’s image. He compared the potential effect to “rat poison.” Ninety percent of it’s not toxic, Tucker and the other member recalled him saying, but it’s the 10% that’ll kill you. (Laster later denied that he was proposing keeping the report secret.)
The consultants reminded the authority that because it was subject to open records laws, the report was going to get out. However if the authority released it, members would have better control of how it was perceived: It would demonstrate the body’s independence and its fidelity to its oversight responsibilities.
Tucker spoke vigorously in support of this view and suggested that if the authority was uncomfortable with announcing the report, it should at least post the findings on its website. That had been the practice until 2012, when, at Wernick’s urging, the authority voted not to release that year’s report. She said the authority should not condone that kind of secrecy anymore.
An authority member, who did not want to be named, told me the rest of the board was not convinced: “Even if the cost of care is too much, there was agreement in the room that undermining Phoebe, damaging Phoebe publicly, criticizing Phoebe too harshly in public is bad for the community in that Phoebe is the biggest employer and the only place you can go if you’re getting sick.”
Singfield suggested tabling the discussion until the next meeting, saying he was committed to releasing the report but wanted to give the authority time to work on how to do so. Four years later, the authority has still not made the report public.
June 1-2, 2022
Palazzolo returned to meet with Mrs. Parker, Andrea and her sister, Kim. He asked again whether Dr. Parker had signed a living will. Andrea said that he had, but there was no need for one. Her mother knew her father’s wishes. She would make any and all calls on her father’s care, and the children would support her 100%. What they needed from Phoebe was a clear assessment of their father’s condition. She asked whether he was brain dead.
Palazzolo said that he wasn’t and that, in fact, Dr. Parker was largely breathing on his own. His cognitive function, though, had been damaged beyond repair and would likely make it impossible for him to ever be the person he was.
Kim asked him to say more. Palazzolo stammered, searching for the right words. That man in there, he said, is not …
“… our dad,” Kim said, finishing his sentence.
Palazzolo nodded.
Kim kept going. “Because our dad left the day of the procedure.”
Palazzolo’s eyes lowered.
Mrs. Parker wanted another opinion. How could Phoebe have gone from telling her one minute that there was a chance to save her husband to saying that he’d been doomed from the time his heart stopped beating a week ago? She tried to come up with the name of a doctor she trusted to put her family’s interests ahead of Phoebe’s. There wasn’t anyone who didn’t have ties to the hospital. She immediately thought of her own neurologist, Marla Morgan. On staff at Phoebe, she’d become close to Mrs. Parker.
Morgan came from another of Albany’s prominent Black families. Her late father had served as president of Albany State University for 16 years. She arrived at Phoebe late Thursday afternoon and spent about 20 minutes in Dr. Parker’s room. Afterward, she asked Mrs. Parker whether he’d ever responded to the sound of her voice, to her pleas to open his eyes or squeeze her hand? Mrs. Parker shook her head.
Morgan said she didn’t see any sign of cognitive brain function. There was only the slimmest chance there ever would be. She used the same language Mrs. Parker had heard from Palazzolo. Her husband wasn’t getting progressively better.
That was enough for Mrs. Parker. Anthony would never want to live in a vegetative state. She instructed the medical staff to withdraw nutritional and respiratory support. In the previous days, Phoebe executives had stopped coming by Dr. Parker’s room. She wondered whether their absence was a gesture of respect or avoidance. Ever since her meeting with Garrett, the kids were increasingly unable to keep up a polite front and were fine not to see them. Kim and Andrea did not want to watch their father die. They said their goodbyes and asked their mother to call them when it was over. Richard offered to stay.
Mrs. Parker felt that she and her family were on their own — and that they always had been. She couldn’t make sense of how this had happened, of how Phoebe had allowed this to happen. She wanted so badly to scream at someone and demand an explanation, but there was no one around.
She needed to write a text to her siblings, Dr. Parker’s staff and several of their close friends, but how was she going to explain what had occurred, much less what was ahead for her husband? The cruel truth, she thought to herself, was that he was doped up and dying — she knew she couldn’t say that, though. She pulled out her phone, summoned what felt like her last shred of sanity and composed a message, which said only that he had begun “transitioning” and thanked them for their prayers.
Anthony Parker and a pregnant Sandra in 1973 and the Parker children, Andrea, Kim and Richard, on a trip to Tennessee in 1984
CHAPTER 8
Mt. Zion Baptist Church, the home of the 1961 civil rights protests, remains one of the most influential Black congregations in the city. Its pastor, Daniel Simmons, told me that in 2007 his members helped fund the opening of a free clinic, called Samaritan, across the street from Phoebe, for people without health insurance. The country was in the throes of the Great Recession. “People were dying in our backyard,” he said. “It wasn’t because they didn’t want to go to the doctor. It was because they couldn’t afford it.”
Phoebe donated one of its properties — a single-story brick building across the street — to the clinic and agreed to provide lab work for patients who qualified for state indigent funds. When I sat down with Simmons 13 years later, the need for the clinic wasn’t all that different from when it had opened. Some 16% of Albany residents were uninsured, almost double the national average, in part because the governor and the legislature had decided not to expand Medicaid. Albany, though, had Phoebe, a hospital whose mission was to care for people no matter their race or ability to pay. So I asked Simmons why a safety-net hospital needed a safety net.
Simmons arranged for me to meet Nedra Fortson, the nurse practitioner who runs the clinic. The day I met Fortson, she wasn’t seeing patients but was waiting for a repairman to come patch two holes in the building’s leaky roof. Phoebe hadn’t done much to maintain the property, she told me. (A Phoebe spokesperson said that over the years the hospital had “invested significantly in maintenance and repairs” to the building.)
As I began to ask the same question I had asked Simmons — why would people seek care at the clinic when Phoebe’s emergency room was right across the street — there was a knock at the door. In came a tall, muscular man wearing carpenter’s jeans, a face mask with Phoebe’s logo and a T-shirt with the words, “I am Phoebe.” His jaw was swollen from an infected tooth, and he was wondering whether Fortson could help him find someone to take it out.
The man told me he was 36 and worked on contract as a groundskeeper at the hospital. I recalled that Wernick had gotten his start as a hospital groundskeeper. I also thought that this man’s story was such a perfect illustration of the clinic’s importance that if his jaw hadn’t been oozing with pus, I might have thought I was being set up.
I asked him whether he’d sought help from Phoebe. He explained that he’d gone to the emergency room a few days earlier, and after a 10-hour wait and a 10-minute examination by a nurse, he walked out with two slips of paper: one with a prescription for antibiotics, the other with a list of dentists. I asked what happened to the slips of paper. He rolled his eyes and said, “I threw ’em away.”
On his $9-an-hour salary, he said, he couldn’t afford health insurance, and without insurance, he couldn’t afford antibiotics or a dentist. He had tried home remedies — mostly gargling with saltwater — but the pain in his mouth got worse. “It feels like I got hit with a fastball,” he said. The groundskeeper, who asked not to be identified because he didn’t want to put his job at risk, still forced himself to go to work because he needed the money. That turned out to be a good thing, he said, because one of his colleagues spotted Fortson driving into the clinic parking lot and sent him over to see whether Samaritan could refer him to a dentist who could treat him for free.
Then it was Fortson who rolled her eyes, not about the request of finding a dentist, which she managed to do that afternoon, but about someone doing work for Phoebe and coming to her for medical care. The groundskeeper wasn’t an anomaly, she told me. Nodding in the direction of the hospital, she said: “They all know us over there. Their cafeteria workers, their janitors, their clerks, their nursing assistants and so on.”
With more than 5,500 workers, Phoebe Putney Health System is the largest employer in southwest Georgia. Its growth tracks with what’s happening across the country as the health care sector expands and manufacturing declines. But national studies have shown that hospital jobs are not like the manufacturing jobs they’ve replaced. The latter generally pay salaries that help lift unskilled workers into the middle class. Most hospital jobs don’t, which has an effect on both the workers and their ability to stimulate the local economy.
One 2017 study of workers in 11 industrial states found that for every higher-paying job held by doctors, six health care employees — including phlebotomists, orderlies, cooks — make less than $15 an hour. In Albany, where 78% of residents do not have college degrees, they were making on average less than $10.
Jack Nicholas Hilton, a former Cooper Tire worker, told me that at the time he’d gotten laid off, he was making $24 an hour. He said he was lucky enough to have a wife who was working as a nurse at Phoebe and could support him while he went back to school for a nursing degree. He made $21 an hour when he started at Phoebe in 2010. In addition, health benefits for him and his family of four came with a $5,000 deductible. If he had a kidney stone, which he did from time to time, that was $2,500 out of his pocket. “People think that if you work in health care you get good benefits,” he said. “Mine were terrible.” Hilton left Phoebe after three years and no longer works as a nurse.
Numerous other nurses at Phoebe shared similar stories. One former senior nursing manager told me she paid $300 every two weeks to cover herself, her husband and two children, including one in college, who had to drive home three hours for routine exams because Phoebe’s health plans did not cover those services elsewhere. The nurse now works for a hospital in California and pays $80 a month for the same coverage, and her daughter can receive care in the town where she goes to school.
An ICU nursing supervisor, who suffers serious allergies, told me he got his EpiPens from a school nurse, who would give him the extras she had every month. One day he and his wife went to see a Phoebe doctor to discuss a vasectomy and were told he’d have a $900 copay up front, which was not reimbursable. He said that he joked about it with his wife, saying, “$900 will buy us a lot of condoms.”
East AlbanyAlmudena Toral/ProPublica
A Phoebe spokesperson said the health system offered high-deductible health insurance plans “for those who wish to minimize premiums, as well as offering a co-pay plan for those who prefer not to have a high-deductible plan.” This year, he added, Phoebe is paying 87% of the cost of health insurance premiums for employees.
Like hospitals across the country, Phoebe has been overwhelmed by nursing and physician shortages. According to the hospital’s financial records, between 2014 to 2022, its spending on contract staff exploded from $2.5 million to $150.2 million. Administrators told me that about $100 million of that went to pay for traveling nurses. Although they don’t receive health benefits, traveling nurses fetch salaries that are at least twice as high as those paid to the permanent nursing staff. This transient staff is not only a drain on Phoebe’s resources but typically doesn’t invest in the community by buying homes or sending their children to local schools.
It’s part of a vicious cycle that incentivizes permanent nurses to travel, further crippling Albany’s economy. The people who remain in town, for the most part, are low-skilled, low-paid employees, like the certified nursing assistant who worked part-time as a DoorDash delivery driver; the oncology scheduler whose colonoscopy bill had been sent to a collection agency; and Louise Williams, 51-year-old single mother and grandmother, known by her nickname, “Weezie.” She worked 22 years at Phoebe in what is called the environmental services — cleaning and disinfecting patient rooms. During the first year of the pandemic, she was the only person on Phoebe’s staff to die of COVID-19.
In her honor, the hospital renovated the environmental services staff break room, installing recliners, a refrigerator stocked with healthy snacks and a flat-screen TV. At a ribbon-cutting ceremony that was attended by Steiner and other hospital executives, the room was christened Weezie’s Place. The hospital invited her family, including her daughter, Shabreka Dent, who thanked Phoebe for remembering unsung heroes like her mother. “My mom was a Phoebe person,” she said. “She loved working here.”
A few months before the dedication, I had gone to see Williams’ family because two nurses at the hospital had told me they were taking up a collection to help pay her funeral costs. Dent said the same thing to me that she would say at Phoebe: Her mother loved working at the hospital.
“Nothing we ever said would get her to leave that place,” Dent told me.
Did you try to get her to leave? I asked.
“I used to tell her all the time she should quit that job,” she said.
Why? I asked.
“Because she was always struggling.”
Dent said that when her mother first started at Phoebe more than 20 years ago, she worked part time, thinking she’d eventually find a different job with better hours and better pay. But Williams’ prospects were limited, because she hadn’t finished high school, factories were starting to lay people off and the only employer whose future looked bright was the hospital. Two decades later, Williams was earning less than $10 an hour, often taking home less than $300 a week.
When Williams died, she was late on her rent, which Dent said happened frequently. Her mother’s day-to-day existence, she said, was a gantlet of overdue bills and payday loans, which became even more crushing in 2014, after Dent’s older sister died of cervical cancer and Williams took custody of her two teenage grandsons.
“She would call me, and say, ‘Hey, I’m fine, but if you could get the boys something to eat.’ Or there were several times I paid the light bill for her, or she’d come around, and I’d pay her cellphone bill, or when time for school came around, I’d get clothes for all the kids.”
Dent showed me where she’d gotten her mother’s name tattooed on her right forearm. “She used to say she liked taking care of people,” she said. “I told her, ‘That’s all good, but you got to take care of you, too.’”
Sandra Parker in front of a portrait of her husband at Georgia’s Albany Technical College
Alyssa Pointer for ProPublica
June 3-6, 2022
There was no longer any reason to keep Dr. Parker in the ICU. On Friday, Mrs. Parker agreed to have him moved to a regular medical floor. The next day, a nurse asked whether she wouldn’t like to have him transferred to Phoebe’s hospice, which is set in a quiet, wooded area of northwest Albany. Its design was inspired by Frank Lloyd Wright, and it was named for William Harry Willson, the pecan magnate who’d first invited Dr. Parker to join the hospital’s board.
“This room was made for daddy,” Richard said when he walked in, marveling at the prints of World War II fighter planes on the walls and at the floor-to-ceiling windows that looked out onto a patio, shaded by pine trees.
On Sunday afternoon, Mrs. Parker’s nephew brought ribs from the Parkers’ favorite barbecue restaurant in Columbus. Two friends, including a woman who’d worked as the executive assistant to Joel Wernick, the former CEO, joined for lunch. Pastor Daniel Simmons of Mt. Zion Baptist Church stopped by to pray. And then Mrs. Parker spoke by telephone with her daughters, giggling with them about the plans she’d made for that evening. The NBA finals were on television. She was going to put the game on and cheer for Steph Curry while cuddling beside her husband, as they’d done on so many date nights.
When Mrs. Parker scooted in the bed, Dr. Parker began to spasm. She hopped out and made a joke of the whole thing to the kids. “Can you believe your daddy kicked me out of the bed?” she texted. “I told him,‘That’s fine. I didn’t really want to sleep with you either.’”
After the game, she brushed her teeth and then sat next to the bed to pray. She started by thanking God for the time she’d had with Anthony and for whatever time they had left. “Let your will be done,” she said, “and allow us to be able to accept your will.” Then she looked up at her husband. He would have hated the way he looked, she thought; unbathed, mouth stuck open, face covered with stubble, a cold sore on his top lip. She whispered to him: “We’re going to be OK. Don’t worry about us.” Then she laid her head on his stomach and was lulled to sleep by the rise and fall of his breathing.
At about 1:30 in the morning, she woke up with a start. His stomach had stopped moving.
“Well, damn,” she whispered. For some crazy reason, she had held out hope that her husband would prove the doctors wrong.
She drew his South Carolina State blanket up over his chest, pulled out her phone and took a couple of pictures in case she wanted to remember the moment, in case there came a time when she’d want others to know.
Then she kissed him, told him she loved him and let the undertaker take him away.
Anthony Parker watching his son, Richard, play Pee Wee football in 1990
CHAPTER 9
I learned about Dr. Parker’s death from Nyota Tucker. The hospital authority board member knew the Parker family because her daughter, who was chief of pediatrics at a large Boston hospital, was close to Andrea, the Parkers’ younger daughter. In a small town like Albany, the death of someone as important as Dr. Parker was big news. Phoebe issued a statement lamenting the loss of a beloved board member that didn’t mention he’d died in its care. The Albany Herald ran statements of appreciation from other leaders in the community and an obituary, without saying how and where he’d died. There was a flurry of posts on the not-always-reliable Phoebe Factoids Facebook page, alleging that something at the hospital had gone terribly wrong.
If true, the quality of care Phoebe provided was worse than I’d thought. Dr. Parker had not died like so many of the patients I’d learned about amid the chaos of the pandemic — Maude Burke, LaTosha Almond and Louise Williams. He wasn’t a poor, uninsured person unable to afford to take care of himself, like the people I’d met at the Samaritan clinic. He was a well-known, well-off, widely respected pillar of the community who seemed to have gone to the hospital for a routine, elective procedure. Even more than that, he was a member of the health system’s board. If he couldn’t get good care at Phoebe, then who could?
Tucker was sure that Mrs. Parker would hire a lawyer to demand answers from the hospital and file suit for restitution. She wasn’t sure what the CEO, Scott Steiner, would do, though. Would he help the Parkers get to the bottom of what happened or fight them? That, in her mind, would indicate how much Phoebe’s relationship with Albany had or had not changed.
She had no idea, however, that there was another clash looming between Phoebe and Albany, that it would play out in the open and that Tucker would wind up on the losing side.
The issue was such a hyperlocal affair that I ignored it for the longest time. It involved the hospital’s plans to demolish the old Albany Middle School and use the property for the construction of the nurses’ living and learning center that had been Dr. Parker’s dream. Phoebe had acquired the building 20 years earlier, shortly after it had been replaced by a modern facility. Like so many of its properties, the hospital had done little to maintain it. Now Phoebe was saying that the school had fallen into such disrepair that demolishing it was much cheaper than restoring and adapting it. But to raze the school, Phoebe had to gain the approval of Albany’s Historic Preservation Commission, an eight-member panel of volunteers appointed by the city and county councils.
In a 4-3 vote, the commission denied Phoebe’s request. The majority argued that the school, which opened in 1925 for whites only, was one of the last remaining examples of Beaux Arts architecture in town and was on the commission’s register of historically significant structures. The city planning department also recommended that the building be preserved and urged Phoebe to consider one of its other properties for the project, including the old Palmyra building.
The hostility coming from the overwhelmingly white crowd felt so visceral to the preservationists that the one Black member of the commission, who’d voted in favor of the demolition, felt compelled to defend her colleagues on the other side. She told the crowd that there was more than bricks and mortar at stake, that landmarks held history.
“We’re not the enemy sitting up here,” she said. “I was born at Phoebe Putney hospital. My grandfather installed the first air conditioning at Phoebe Putney hospital.” She went on to say, “My aunt was one of the first African American social workers at the hospital.”
The editor of the Albany Herald, Carlton Fletcher, had weighed in with a column under the headline “Attempt to stop Phoebe/Albany Tech project beyond ridiculous.” He laid out an argument that was so similar to the one I had heard from Steiner that if I didn’t know better, I’d have thought he had written it. Opponents to the demolition were motivated by old grudges toward Wernick, Fletcher wrote. Their position was an example of “the depths to which some would sink to sabotage the health care facility’s moving forward.”
Tucker was paying close attention to the fight. She had no doubt the new nursing school would be good for Albany and Phoebe. But she didn’t think the preservationists were being unreasonable either, and she was increasingly troubled by the tone of the hospital’s campaign. Phoebe had plenty of other properties that could be used for the living and learning center, and even if the hospital was dead-set on tearing down the school, she hoped it, and Steiner, would proceed with the same together-we-rise spirit that they’d professed during the pandemic.
A week after the vote, Phoebe and the hospital authority filed an appeal with the City Commission, accusing the preservation commission of abusing its discretion. Tucker didn’t believe me when I asked her about the appeal. The authority, she said, had never held a vote to take such an action. I sent her a copy of the appeal, which showed that it had been filed by the authority and signed by Phoebe’s lawyer.
Tucker said she had no idea what was going on. The authority was independent of the hospital, or at least that’s what she’d been led to believe. Phoebe’s lawyer should not be acting on the authority’s behalf, she said. She called Glenn Singfield, the authority’s chair. According to Tucker, he told her he believed the members of the authority supported the hospital and had taken it upon himself to sign on to the appeal, at Phoebe’s request. She told him his actions “bordered on unethical behavior” and could be seen as a “violation of public trust.”
Singfield refused to talk to me about the phone call with Tucker but insisted that he was not doing the hospital’s bidding. He said the same to her and later, in a text, promised, “I will protect our independence.” He convened a special meeting of the authority for later that day to take a formal vote on what he’d already done without one. Tucker called as soon as the meeting was over and told me that several members expressed concern about the way Singfield had handled the appeal but still threw their support behind Phoebe. She was the only one who voted against the appeal.
A month later, the Albany City Commission convened to consider Phoebe’s appeal. Mayor Kermit “Bo” Dorough, who had long vowed to rein in Phoebe, oversaw the proceedings. I was watching the livestream but couldn’t see the crowd. Tucker and the mayor told me the room was packed.
Bryant Harden, a political science professor at Mercer University and chair of the preservation commission, spoke first to explain the group’s vote against demolition. Its majority wasn’t opposed to the construction of a nursing school, he said, but the hospital had so many places it could build the new campus without knocking down an important part of the city’s history. What was the harm in considering other options?
The Steiner who took the podium sounded different from the man I’d met during the pandemic. From his first words he was confrontational. He said there were “a few loud people in our country, our state of Georgia and here locally in Dougherty County and Albany that seek to keep us all divided.” The project’s opponents were pushing their “own selfish causes and not what’s in the best interests of our businesses, our people, our police, our region, our nurses, our schools, our churches and certainly not our community.”
When a city council member asked Steiner about the preservation commission’s plea to find an alternative location for the project, he thought for a second and said: “You know, if you just salvaged the front exterior or the whole building and created the world’s biggest liquor store, it would be OK with the HPC.”
Tucker told me people gasped — the proliferation of liquor stores in poor Black neighborhoods had long been a sensitive subject in Albany — and her hope for a new kind of leadership at Phoebe evaporated. She lamented that Steiner would take “such a cheap shot,” and added, “At that moment, he reminded me of Joel Wernick.”
I’ll admit that I gasped too — not just because it seemed like such a gratuitous comment; it was how it embodied the hospital’s conduct during the entire fight. At every turn, Phoebe sought to beat the preservationists into submission. Ultimately it worked. The City Commission, which includes the mayor, voted unanimously to approve the demolition. “We’ve only got one hospital,” Dorough told me, “and we’re not going to get another one.”
The preservationists took their fight to the Dougherty County Superior Court and found Phoebe’s reach extended even there. The chief judge recused himself because his daughter worked for the hospital. The next judge, who acknowledged that she served on a bank board with Steiner and Phoebe’s outside counsel, denied the preservationists’ request that she recuse herself and ruled in favor of the demolition.
If that wasn’t enough of a victory, the City Commission voted not to renew two of the four members who had opposed the demolition, prompting two other members to resign in protest. The city commissioners replaced them with four new members. One of them had financial ties to Phoebe, another to Albany Tech. A city commissioner told the Albany Herald that he “certainly wasn’t letting politics get in the way of my vote.” Another said, “We chose who we thought were the best.”
Then Albany and Phoebe turned on Tucker. She had come to the end of her first five-year term on the hospital authority and was up for reappointment, which required a vote by the county commission. Reappointment to the authority had previously been a perfunctory affair. All a sitting member needed to do was to tell the county that they were willing to serve again. Tucker was so sure of it that she didn’t attend the vote. Afterward, however, a clerk called to notify her that she hadn’t been renewed.
I asked a board member who served with Tucker about her removal. He told me that the hospital and the authority didn’t see her as a team player and wanted her off. “She was for sure not reappointed for that reason,” he said. “I have no doubt about that.” (When asked about Phoebe’s role in her departure, a hospital spokesperson said the Dougherty County Commission “has the sole responsibility of deciding whether to reappoint any member.”)
Several weeks later, Tucker addressed the county commission. She had no illusions about getting reinstated, and she had no intention of asking. Nervous and halting, she said that when she joined the hospital authority, she committed herself to serving the public, not Phoebe. The commission’s decision made her wonder whose team they were on. “An independent hospital authority board does not happen in a vacuum,” she said. “It cannot happen if members are removed from the board who question or who point out discrepancies. When they are removed from the board, you can expect that independence will end.”
Crews demolish the old Albany Middle School to make way for Phoebe Putney Memorial Hospital’s living and learning center.
Alyssa Pointer for ProPublica
August 2023
Shortly after her husband died, Mrs. Parker retained a lawyer named Adam Malone. She was prepared to sue, she told her kids, but she was hoping she wouldn’t have to. Malone had won some of the largest malpractice awards in Georgia’s history. But what appealed to Mrs. Parker was that although he lived in Atlanta, he had grown up in Albany. His father had been a prominent lawyer there in the 1950s and ’60s and was one of the few whites willing to collaborate with Black law firms and take on Black clients. If she sued, she believed, Malone would understand the forces he was up against and not be intimidated by them.
Mrs. Parker had no idea what had caused her husband’s death. None of the executives who had sat with her and her family at her husband’s bedside had called or visited to offer an explanation. She’d invited Steiner to speak at the funeral, but that was to keep up appearances. She took his invitation to attend a health system board ceremony in honor of Dr. Parker as evidence of his trying to do the same. Phoebe’s silence felt like a conspiracy. Even worse, at times, were calls from people she and Phoebe had in common. They always left her wondering whose side were they really on.
It was a question that nagged at her as she considered the lawsuit. She doubted that many of those people would stand with her if she sued — at least not publicly. People like Glenn Singfield, who would check in from time to time to see how she was doing and say how sorry he was about what had happened. She had every right to demand an explanation, he’d say, but she kept her plans to herself because as close as the two were, he was chair of the hospital authority.
The relationship with her husband’s successor at Albany Tech changed, too. He’d been her husband’s protégé, but the school needed the financial boost from its new partnership with Phoebe. She knew he couldn’t risk that project by calling out the hospital. (He did not respond to a request for comment.)
I asked Mrs. Parker what she thought her husband would have done if he was alive and a different board member had died under the same circumstances. She said she would like to think that he would privately press the hospital for answers, but she doubted that he’d have questioned or criticized the hospital in public. Dr. Parker was a loyal member of the Phoebe family, she said, adding air quotes. Whenever the hospital had come under fire, he gave it the benefit of the doubt, partly because he didn’t want to be marked as a traitor, much less painted as a crank like the people behind Phoebe Factoids, and lose his place on the board, and partly because few people had ever taken on Phoebe and won.
“He wasn’t a naive man,” Mrs. Parker said, “but I think he drank the Kool-Aid.”
In August 2023, 14 months after Dr. Parker died, Mrs. Parker filed a lawsuit against both the hospital and the health system, as well as three members of the anesthesiology team involved in her husband’s operation, accusing them of negligence. She told me she wanted Phoebe to pay restitution to her and her children. She wanted answers about what caused his death, and she believed Phoebe wouldn’t give them to her unless it had to. She wanted to give her husband’s death, and her own future, some meaning. But there was something else. She worried about what message it would send if she didn’t sue: “I don’t want them to get away with it this time.”
CHAPTER 10
Over a couple of days, at the end of last year, Scott Steiner and I talked. He looked like a different person than when we first met. He’d lost a lot of weight. He’d previously struck me as someone who didn’t fuss over his appearance, but it was hard to miss the attention he now paid to his hair, beard and close-fitting blazer. I would have been embarrassed to tell him that he seemed like a guy in the throes of a midlife crisis, but, without prompting, he admitted as much, sharing a picture of his new car: a 1979 Pontiac Trans Am. “It was either a new car or a girlfriend,” he joked. “A car is cheaper.”
With some $200 million in new projects — nearly half of which was funded with county bonds — parts of Phoebe looked different, too. A glass-encased trauma center had recently opened, with an ICU for newborns and a helipad on the roof, which was now the highest point in Albany. At the same time, he’d begun to put several of Phoebe’s unused properties on the market and donated four of them to Habitat for Humanity.
Steiner took me on a short tour of the new living and learning center, whose lobby is dominated by a large mural that includes likenesses of the hospital’s first Black nurses and whose 80 fully furnished apartments have walk-in closets that I told him might qualify as bedrooms in New York City. He pointed out that some of the brick, benches and light fixtures inside the lobby were original to the building. So, too, were some of the arches and moldings on the facade. I’d been warned that he wasn’t going to comment on the Parkers’ lawsuit. Still, I thought it was telling that he didn’t show me Dr. Parker’s portrait, which was hanging in an alcove toward the rear. What was even more telling was how a man who’d made so many changes at Phoebe and who’d insisted that he wanted everyone to let go of past grudges was still quick to raise them. Within 20 minutes after we sat down in the lobby, I asked him how he’d describe Albany to someone who wasn’t from there, and the words “Joel Wernick” were part of his answer.
He’d begun by riffing on how Albany is a “very historical community” and a “melting pot of race.” He said it has “issues like any community” and that Albany’s were crime and poor schools. As for the people, he recalled how friendly they were to him and his wife when they first arrived. He’d gotten used to their tendency to obsess over the things Albany “could have been.” But there were qualities that still really bothered him. “I think there’s a segment of the population that doesn’t want to see it better,” he said. Then he added: “People want to live in the past so much. People still want to talk about Joel Wernick’s shortcomings.”
I wanted to make clear that’s not why I was there and tried to move the focus of our conversation to some of the things I’d learned during my reporting, like the way diabetes rates spiked in the years after Phoebe acquired Palmyra. I hadn’t come up with a way to explain it, I told Steiner, but in reading the hospital’s nonprofit filings, I couldn’t help noticing that the spike coincided with a decline in the share of revenue that Phoebe spent on preventive health services and on providing free and subsidized care to the poor.
Steiner pointed out that Phoebe’s lease with the county only required it to spend 3% of its revenue on charity care and that it had never never failed to meet that requirement. That was true, I acknowledged, but I reminded him that Phoebe’s own lease analysis showed that at the time Steiner arrived the hospital wasn’t providing as much assistance to the poor as its state and regional peers. Some of them were spending as much as 10% of their revenue on charity care.
Steiner held firm. “But we still met the lease.”
Actually, Steiner had done more than that. After getting the results of the lease analysis, which showed that Phoebe was not spending as big a share of its revenue on free and subsidized care as its peers, he expanded the pool of people who were eligible for assistance. His staff had also increased its efforts to get more patients to apply for care.
Steiner said he wasn’t measuring the hospital’s contributions entirely on dollars spent. “I want to do the most impactful programs. I want to impact the most lives,” he said.
He looked around at the soaring lobby in which we were sitting and talked about how the living and learning center would address one of the biggest drains on the hospital’s budget: traveling doctors and nurses. “People could question: ‘Why’d y’all spend money on this? Y’all spent $40 million, $45 million.’ And yeah, I can understand that, but I also know the cost and the impact of having a rotating staff and that it’s not good. It’s not good financially. It’s not good from a patient care standpoint. It’s not good for our community.”
He said that the nursing shortage at Phoebe was nowhere near what it had been during the pandemic, but that even as we spoke, half of the 500 job openings at the hospital were for nurses. When I asked whether that affected the quality of care, he said, “Absolutely, 100%.”
Speaking about the differences between staff nurses and travelers, he said, “We know that when it’s our own team, when it’s a Phoebe employee, there are less errors and quality’s higher, and we know when it’s contract nurses, there are higher errors, and our patients are less safe.”
I brought up the hospital’s persistently poor quality of care scores — that Phoebe still only had two stars from the Centers for Medicare & Medicaid Services, and its grade from the Leapfrog Group, a coalition of large health insurers and leading patient safety experts, had gone down from an A in 2022 to a C in 2024 and remained there in 2025. The ratings reports indicated that the hospital had made improvements in crucial areas like sepsis prevention, but it continued to have trouble with readmission rates, accidental cuts and tears after surgery, bedsores and dangerous blood clots.
Steiner didn’t deny the findings but criticized them as unreliable because they’re based on data that is at least three years old. CMS’ ratings were particularly misleading, he said, because they included how patients feel about being in the hospital as well as how well a hospital follows standards of care — and no patient likes being in the hospital. “Consumers are inherently unhappy,” he said, “whether it’s Subway, whether it’s a gas station.”
I pressed him to clarify, because Subway sandwiches are different from readmission rates. “I’m just saying there are big chunks of these ratings, they’re saying patient safety is how good the food is,” he said.
When I returned to the hospital’s high readmission rates, Steiner retreated. “We have work to do, no doubt,” he said and then went back to laying the blame elsewhere. “Would I like to be a five star? Absolutely. But when you look at who four- and five-star hospitals are, they’re usually not in challenging communities that have a lot of poverty.”
That’s not entirely true. A good number of hospitals with three and four stars are in poor places. What Steiner said next made clear he knew that. “We’re not OK being a one- or two-star hospital,” he said. “We’re not OK being a C. Our community deserves for us to be better.”
Then I talked to Steiner about some of the patients whose stories I’d looked into during my time in Albany. I told him about LaTosha Almond having been sent home with a bedsore so severe she was readmitted to the hospital the day after she’d been discharged, then was sent home with a trach no one had taught her to manage and ultimately died. I also brought up the hospital groundskeeper I’d met at the Samaritan clinic and asked Steiner why he thought a man who worked for a safety-net hospital would have to turn to a free clinic for medical care?
Steiner seemed moved. He told me that he didn’t know Almond but that if what I’d told him was true, there was no excuse for what happened to her. As for the groundskeeper, he was troubled by that story, too. But he painted it as less an indictment of Phoebe and instead as “part of the brokenness in general of the health care system.” He said, “Even though I think we are a safety net — we’re an essential hospital for tens of thousands of people a year — a net still has openings.” He added, “I don’t think the health care system in the United States is set up to help him.”
The Westover neighborhood of AlbanyRoss Landenberger for ProPublica
After about two and a half hours, Steiner’s spokesperson reminded him it was time to wrap up. Before we did, I wanted to go back to something he’d said earlier. He’d told me that when it came to choosing which services Phoebe provides, he made the call, and he wasn’t afraid to be held responsible. What I asked him was: Who holds him to account?
He said something that surprised me. Or perhaps it was me not thinking of Phoebe the way it thinks of itself — as a business. “I hope that our consumers do, right?” he said. “They can do that by electing to get care elsewhere.”
What he didn’t say was that most people in Albany don’t have anywhere else.
A couple of days later, Steiner agreed to meet again. I wondered, with the passage of time, whether he regretted his liquor store comment during the Albany Middle School fight. But nope, he repeated it. “I could have opened Georgia’s largest liquor store, and that group didn’t care,” he told me. “They would’ve said, ‘We approve.’”
For his part, he’d been mulling over what I’d told him about the groundskeeper and the Samaritan clinic. “There’s a fine line between providing everything at no cost and at no responsibility and being able to run any business,” he said. “I think it’s just like somebody walking into a grocery store saying: ‘I’m hungry. My children are hungry. I’m malnourished, so I’m going to fill my cart up and I’m going to walk out.’ Where’s that balance, right?”
Yes, he said, the hospital’s mission is to provide care regardless of race, religion and ability to pay, “but we’re always trying to balance that out with paying the bills.” He added, “We’ve got human beings’ lives in our hands. Most days we get it absolutely correct, and some days we don’t.”
He reminded me that Phoebe had allowed the clinic to operate in one of the health system’s properties without charging rent. He said it had done so precisely because it understood there were uninsured people who might fall through the cracks. The clinic, he said, was not some separate safety net, it was part of Phoebe’s.
I asked Steiner whether he was aware that the net had collapsed: Samaritan’s offices and exam rooms had been so overtaken by mold that they’d been deemed unsafe and had been shuttered for more than a month.
A few days later, Nedra Fortson, the clinic’s administrator, called to tell me that Steiner had surprised her with a request to visit the facility. He did a walk-through and arranged for the clinic to move into another building.
Epilogue
In April, a Dougherty County jury awarded $70 million to a woman from nearby Camilla who had accused Phoebe and three Albany-area physicians of negligence. She charged that the doctors administered an overdose of blood pressure medications without adequate oversight for more than 40 hours. The blood flow to her extremities was severely constricted, she argued, and caused such irreparable damage to her legs they had to be amputated above the knee. She was 28 at the time.
Phoebe reached a settlement with her before the case went to trial. A spokesperson described what had happened to the patient as “undeniably tragic” but added that “the evidence indicates she would have died without the interventions provided by the care teams.” The physicians held out. They, too, asserted that they had saved the patient’s life. After the verdict — one of the largest in Georgia’s history — the doctors settled for an undisclosed amount.
I suspected that Phoebe would quickly settle the Parker lawsuit, making it almost impossible for the family to find out what had happened to Dr. Parker. Instead, the case stretched out for almost 20 months, with both parties gathering medical records and conducting depositions. What occurred during his ablation began to emerge. Most damning was a statement from Dr. José Ernesto Betancourt, the cardiologist who oversaw the procedure to correct Dr. Parker’s irregular heartbeat. He described Dr. Parker’s cardiac arrest as a “preventable event,” saying it happened “very unfortunately.”
According to the depositions, Dr. Parker’s blood pressure plummeted so low partway through the procedure that Betancourt paused to make sure that he hadn’t inadvertently punctured Dr. Parker’s heart. Once he determined that he hadn’t, he gave the nurse anesthetist, Alan-Wayne Howard, time to stabilize Dr. Parker with medication, then resumed the procedure, finishing a little before 4 p.m.
At this point, Howard took over Dr. Parker’s care. Neither he nor Betancourt were on staff at the hospital. Both were contract workers. Both lived hours away in Florida but stayed in Albany when on duty. It’s also important to know that Howard was a nurse practitioner, not a doctor. Nurse anesthetists — who have advanced degrees specializing in anesthesia care — are often used at hospitals and surgery centers as a way to cut costs or fill staffing shortages. Because they don’t have the same years of training as a physician, their work is usually done under supervision by an anesthesiologist, who is responsible for the care they provide. He is supposed to check in on them from time to time and is on call for any emergencies.
Betancourt testified that after the ablation Howard recommended sending Dr. Parker to the ICU for observation before removing his breathing tube and withdrawing anesthesia. He said Howard wanted to make sure Dr. Parker’s vital signs were stable before extubating him, and he also wanted Dr. Parker to have the medical support he needed if his blood pressure crashed. “We will need a couple of hours to be able to titrate down the medication to support the blood pressure until it can be completely withdrawn,” Betancourt recalled Howard saying.
Betancourt agreed with that plan, and he left the recovery room to talk to Mrs. Parker. He said he was gone for 10 minutes.
When he returned, at about 4:44 p.m., he said that he looked in again on Dr. Parker and found that Howard had changed the post-operative plan. The anesthetist had removed the breathing tube and begun withdrawing anesthesia. Betancourt said he was surprised but didn’t question the decision: It was Howard’s call to make. He said he asked how Dr. Parker was doing, and Howard assured him that “everything was great.” He left to start his report.
A minute later, Dr. Parker went into crisis. According to handwritten notes by Dr. Michael Coleman, one of the two anesthesiologists assigned to supervise Howard, Dr. Parker “developed bradycardia and hypotension, leading quickly to asystole.” In lay terms that meant that his heart rate and blood pressure plummeted, losing oxygen to his brain, until his heart eventually stopped.
In his deposition, Howard said that it wasn’t until 4:54 — nine minutes later — that he summoned Betancourt and Coleman for help. Betancourt said he was at Dr. Parker’s side at 4:55 — 10 minutes with little to no oxygen going to his brain — and began chest compressions. Coleman arrived a minute later and helped Howard reintubate Dr. Parker, whose heart began beating again at 5 p.m.
None of the doctors or nurses who testified could say exactly when Dr. Parker’s heart had stopped beating during that 15-minute window, which is why there was, and still is, confusion about whether his brain went without oxygen for five or 14 minutes. When asked whether her record was reliable, the nurse assigned to keep track of the time testified that “based on my documentation, I don’t think they have an accurate time. No.”
Howard wasn’t asked during his deposition about why he’d decided to remove respiratory and blood pressure support earlier than initially planned. (His deposition occurred months before Betancourt’s.) However, Howard did let on that he was in a hurry that afternoon. He said that he had hoped to tend to his elderly father in Florida and that Dr. Parker’s procedure went on for so long that he was running late.
In its initial response to the lawsuit, Phoebe argued that because the health system did not employ “any nurse, physician or advanced practice provider” involved in Dr. Parker’s care, it was not liable for his death. It’s an argument that many hospitals make when they are sued and traveling nurses and doctors are involved. Howard denied that he was negligent “in any manner whatsoever.”
This summer, Phoebe, the two supervising anesthesiologists and Howard settled for an undisclosed sum. The three clinicians declined to comment. A Phoebe spokesperson said: “While rare, complications like those that occurred in this case are possible with a cardiac ablation. The care provided in this instance matched the standard of care that should be expected, and we do not believe there is evidence of negligence or malpractice.”
As part of the agreement, Mrs. Parker promised not to disclose the sum but made clear that she was relieved that she and the hospital had come to terms before Georgia capped malpractice awards at $1.05 million. By this time Mrs. Parker had moved to South Carolina, where she could be closer to her siblings.
Before leaving Albany, she’d hired painters to help get her house ready to put on the market. The crew’s chief came to the door to express his condolences. He knew a little something about her pain, he said.
His 35-year-old brother had recently died from sepsis at Phoebe and left him and his family with a lot of questions. Mrs. Parker asked whether they had tried to get answers. The painter shrugged and shook his head no. When she asked him why not, he said, “What good would it do? It’s Phoebe.”
Kim and Sandra Parker in South Carolina in 2024Almudena Toral/ProPublica
The open enrollment period for Medicare ends on December 7, and chaos in the privatized Medicare Advantage market has left many who depend on MA plans confused and possibly uninsured in 2026. Health insurance companies that sponsor Medicare Advantage (MA) plans have aggressively recruited members in the past. Low or $0 premiums plus supplemental benefits that traditional Medicare is not…
A Medicare pilot program will allow private companies to use artificial intelligence to review older Americans’ requests for certain medical care — and will reward the companies when they deny it. In January, the federal Centers for Medicare & Medicaid Services will launch the Wasteful and Inappropriate Services Reduction (WISeR) Model to test AI-powered prior authorizations on certain health…
A new survey of Americans currently enrolled in the Affordable Care Act (ACA) marketplace finds that most would not be able to afford even modest increases in costs. The poll comes as tax credits intended to help some on the program afford their health expenses are just weeks away from expiring. According to KFF, which administered the poll, if no action is taken to remedy the situation…
A newly published study reveals that a certain kind of gender-affirming care for transgender kids and young adults likely lowers rates of suicidality among those populations.
The study, published in the Journal of Pediatrics, examined 432 patients between the ages of 12 and 20 years old who received treatment at an unnamed Midwestern academic medical center. Patients who were set to receive gender-affirming care filled out Ask Suicide-Screening Questions (ASQ) surveys prior to receiving hormone therapy (HT) treatment, then repeated the questionnaire at future visits.
In the first 18 months of the COVID-19 pandemic, tens of thousands of pregnant women were wheeled into hospitals where they fought for their lives and the lives of the babies they carried.
It took the Centers for Disease Control and Prevention until August 2021, eight months after the first vaccine was administered, to formally recommend the COVID-19 shot for pregnant and breastfeeding mothers. The CDC had found that pregnant women with COVID-19 faced a 70% increased risk of dying, compared with those who weren’t. They also faced an increased risk of being admitted to the intensive care unit, needing a form of life support reserved for the sickest patients, and delivering a stillborn baby. In recommending the vaccine, the CDC assured them that the shot was safe and did not cause fertility problems.
ProPublica examined the harm caused by the delay in rolling out and endorsing the vaccine for pregnant mothers. Federal officials at the time told us that they wanted to ensure “an abundance of evidence” before issuing guidance.
But a surprising turn of events this summer reversed that guidance.
In May, Robert F. Kennedy Jr., the Health and Human Services secretary and a longtime vaccine critic, announced on X that “the COVID vaccine for healthy children and healthy pregnant women has been removed from @CDCgov recommended immunization schedule. Bottom line: it’s common sense and it’s good science. We are now one step closer to realizing @POTUS’s promise to Make America Healthy Again.”
The next month, Kennedy fired all 17 sitting members of the CDC’s Advisory Committee on Immunization Practices and replaced them with a selection of hand-picked members. The committee has since shifted its guidance, encouraging people to decide on their own whether to get the shot and to consider individual risk factors.
Doctors and national medical organizations said the new guidance from the CDC has caused confusion among patients and could put pregnant women and their babies at risk of severe illness or hospitalization.
“COVID-19 infection during pregnancy increases the risk of preterm birth, preeclampsia, and stillbirth,” read a statement from the Society for Maternal-Fetal Medicine.
The organization, as well as the American College of Obstetricians and Gynecologists, the nation’s leading professional organization for OB-GYNs, reiterated their recommendations that all those who are pregnant or breastfeeding receive the updated vaccine and booster, regardless of the trimester they’re in.
ProPublica found that though unvaccinated women faced devastating risks, the COVID-19 vaccine had been commandeered by disinformation and doubt. Pharmaceutical companies and government officials had not ensured that pregnant women were included in the early development of the vaccine, despite federal guidance on how to safely include pregnant and breastfeeding people in biomedical research.
The HHS’ communications director, Andrew G. Nixon, defended the federal government’s actions, saying in a statement: “ACIP’s recommendation applies to all individuals six months and older. It includes an emphasis that the risk-benefit of vaccination in individuals under age 65 is most favorable for those who are at an increased risk for severe COVID-19 and lowest for individuals who are not at an increased risk, according to the CDC list of COVID-19 risk factors.”
Pregnancy is listed as a condition that can increase risk.
In the midst of the backlash against the CDC’s guidance, a recent Harvard University study highlights a new risk of COVID-19 during pregnancy. In a rare look at the children of women who contracted COVID-19 while pregnant, the study found that they may be at increased risk for autism and other neurodevelopmental diagnoses by age 3.
Researchers, who followed the children via their medical records from birth through their toddler years, observed some initial developmental delays at 12 months and again around 18 months, said Dr. Andrea Edlow, one of the study’s senior authors and an OB-GYN at Harvard Medical School.
“We were seeing speech and motor delays, but we really didn’t know if they were going to be persistent or evolve into other diagnoses like autism, or if children were maybe going to catch up,” Edlow said. “But that, unfortunately, hasn’t been the case.”
Edlow treated many pregnant patients during the pandemic, including some who experienced a life-threatening condition known as a cytokine storm. They often had high fevers and severe inflammation for several days. The condition, she remembers thinking, couldn’t be good for the placenta or the developing fetal brain.
Edlow and her team studied more than 18,000 live births to mothers who delivered between March 2020 and May 2021. Of those, more than 800 had been diagnosed with COVID-19. What surprised them was that 16.3% of those babies received a neurodevelopmental diagnosis by three years, compared with 9.7% of the babies who were not exposed to COVID-19 in utero. That was a statistically significant finding. During the period covered by the study, the CDC had not yet come out with its formal recommendation for pregnant women to get the COVID-19 vaccine, and as such, most of the mothers were unvaccinated.
The children of mothers who contracted COVID-19 in the third trimester, a critical time for fetal brain development, and boys had an even higher risk. The male placenta and fetal brain, the researchers wrote, are more susceptible to a mother’s immune response to COVID-19 and other infections.
“I know it’s alarming,” Edlow said.
The researchers, she said, are not out to stoke fear. While the risk of autism is increased, Edlow said, the overall risk still remains low. The study underscores the importance of monitoring children born to mothers who had COVID-19 while pregnant for neurodevelopmental conditions.
Edlow encouraged pregnant women to do everything they can to avoid getting COVID-19, including wearing masks, avoiding crowded indoor spaces and getting vaccinated and boosted.
“COVID is a real problem that poses risk to the mom in pregnancy and to the child,” she said. “And it’s still worth preventing, even at this point.”
Dr. Naima Joseph worries about how the reversal of the COVID-19 vaccine recommendation for pregnant patients will affect the health of the country, particularly its most vulnerable residents, women and children.
She remembers standing in line during the pandemic to get her COVID-19 vaccine when her husband, who is also a doctor, turned to her.
“Are you sure you should be doing this?” he asked.
Joseph, a maternal fetal medicine doctor at Boston Medical Center who serves on ACOG’s Immunization, Infectious Disease, and Public Health Preparedness Expert Work Group, paused. She was pregnant with twins. Like so many mothers, what she cared about most in this world was protecting her babies, but she also treated many pregnant patients sick with COVID-19 who spent months fighting for their lives from a hospital bed. Some died or lost their babies.
“Yes,” she replied to her husband before getting the shot.
Senate Republican Ron Johnson (Wisconsin) has said that the U.S. “can’t afford” to implement Donald Trump’s proposal to send out $2,000 checks to supposedly offset costs of tariffs — just days after the president wined and dined some of the richest people on the planet at an extravagant black tie dinner in the White House. “Look, we can’t afford it. I wish we were in a position to return the…
A nurse at Pennsylvania’s York County Prison told a pre-trial detainee, Willie Cunningham, who was suffering from appendicitis that he had heartburn and gave him Pepto-Bismol, according to a lawsuit filed on November 14 by the Pennsylvania Institutional Law Project. The suit was filed against York County, the facility’s then-medical provider, PrimeCare Medical, Inc., and three nurses who…
A year ago, the federal Indian Health Service posted dozens of flyers on Facebook promoting flu and COVID-19 vaccine clinics across the Navajo Nation, where the pandemic had inflicted a staggering toll just a few years earlier.
The notices, featuring photos of smiling families and elders in traditional clothing, tied immunization to tribal values like community responsibility and made a clear case for getting the shots. “Vaccines are effective at preventing serious illness or hospitalization,” one of them said.
But this year, as Health and Human Services Secretary Robert F. Kennedy Jr., a vaccine critic, has put his stamp on federal immunization policy, IHS’ public messaging on vaccines has taken a stark turn.
In internal emails obtained by ProPublica, IHS officials have flagged terms such as “immunizations” and “vaccines” for additional scrutiny, deeming them risky “buzzwords” that require approval from agency public information officers to be used in social media posts, pamphlets and presentations for patients.
Through mid-October, IHS had published far fewer posts on Facebook promoting vaccine clinics this year than last, ProPublica found. And in those posts as well as other notices, it replaced language touting immunization’s benefits with wording that frames both routine childhood vaccinations and annual flu and COVID-19 shots as a personal choice, advising patients to consult health care providers about their “options regarding vaccines.”
Current and former IHS clinicians told ProPublica the changes threaten vaccine uptake in Navajo communities and have left medical practitioners who serve this population feeling censored.
“It seems to me that they’re trying to put up barriers,” said Harry Brown, a physician and epidemiologist who left IHS in 2016 and now works for a tribally operated health facility in North Carolina. In a 26-year career with IHS, he said, he had never encountered an effort to stifle public health campaigns or restrict what medical providers said publicly about vaccines.
Aside from Brown, the health care providers who spoke with ProPublica didn’t want their names used, concerned it could endanger their jobs. One physician said the new IHS restrictions on vaccine-related speech factored into her decision to leave the agency this year.
“I can’t keep people safe,” she said in an interview just before she quit. “I don’t have any of the words anymore to say anything I need to say.”
Two Facebook posts from 2024 by the Indian Health Service in the Navajo area emphasize the importance of vaccination.Navajo Indian Health Service via FacebookA more recent post about COVID-19 vaccine availability by the Indian Health Service in the Navajo area uses more restrained language, no color and no inviting imagery. Navajo Indian Health Service via Facebook
IHS’ shift in vaccine messaging has not been previously reported but aligns with widely publicized changes within the Department of Health and Human Services under Kennedy’s leadership. In the past 10 months, as measles cases have hit their highest levels in decades, Kennedy has been tepid in endorsing the vaccine to prevent the disease while taking several steps critics predict will undermine public confidence in immunization.
He’s launched a federal probe into scientifically debunked links between immunizations and autism and canceled nearly $500 million in contracts and research grants for mRNA vaccines. This technology was central to the speedy development of the COVID-19 vaccine.
In June, he removed all 17 members of the Advisory Committee on Immunization Practices, which advises the Centers for Disease Control and Prevention on vaccine policy, replacing them with his own appointments, including several vaccine skeptics. Kennedy has also endorsed the founders of Idaho’s medical freedom movement, who helped persuade the state to ban vaccine mandates this year.
At IHS, the only branch of HHS that operates its own network of hospitals and clinics, the altered federal landscape on vaccine policy has had a more direct effect on patient care, clinicians said.
In a statement, an HHS spokesperson said the redrafting of IHS’ public messaging materials was designed to encourage “shared decision-making” between patients and their health care providers.
“The Indian Health Service continues to provide accurate, evidence-based information on vaccines and infectious-disease prevention,” the statement said. “Our focus remains ensuring Tribal communities have clear, trusted guidance and access to the care they choose.”
The statement didn’t address questions about what prompted the revamped messaging or concerns raised by doctors about its potential effect.
In a separate statement, Matthew Clark, the IHS’ deputy chief medical officer, insisted the agency’s approach to immunizations has remained consistent, even if its messaging about them has changed.
“We continue to advocate that every patient at every encounter be offered every FDA-approved and ACIP-recommended vaccine, when appropriate,” Clark’s statement said.
It’s not clear yet what effect the changes are having. Data hasn’t been released showing this season’s flu and COVID-19 vaccination rates for the Navajo Nation. Through September, the uptake rate for the measles, mumps and rubella vaccine, known as MMR, for 2-year-olds has held steady at around 95%, the level of herd immunity needed to prevent outbreaks, IHS data shows.
Still, IHS clinicians said, the agency’s lack of public messaging about vaccines was especially notable during the winter and spring, when a measles outbreak emerged in Texas and then neared the reservation’s borders in New Mexico.
The outbreak had spurred alarm. Tribal health facilities, which operate independently from IHS, flooded Facebook with information about MMR shots at the end of February and urged residents to get themselves and their children vaccinated.
Yet two IHS doctors said that at about the same time, the agency installed its new restrictions on vaccine-related speech.
According to a March 13 email that Ryan Goldtooth, a public information officer at one Navajo Nation hospital, sent to colleagues, members of the group had been instructed to take down social media posts or flyers that contained the terms “vaccines (namely Measles)” and “immunizations” from the agency’s Facebook pages. “We cannot forward or post to the public,” the email said.
The email also said that the terms “immunizations” and “vaccines” had been reclassified “from low to medium-risk.” As a result, if clinicians used these words in public presentations and printed materials, they needed to be cleared by a public information officer first, Goldtooth wrote.
The email listed several other topics or types of information that could no longer be freely shared or talked about publicly. Starting from the date President Donald Trump returned to office, any information shared from a state health department, for instance, had to be removed from Facebook, the email said, without providing a reason. Any posts about executive orders also had to come down.
Goldtooth, who still works for IHS, did not respond to requests for comment about the email.
Laura Hammitt, the director of infectious disease programs for the Center for Indigenous Health at Johns Hopkins Bloomberg School of Public Health, has worked closely with IHS staffers on vaccination efforts. Limiting what they can say about vaccines could harm their ability to respond to future outbreaks, she said.
“People are really trying to be compliant with changes required by the administration but also have a responsibility to care for their patients,” Hammitt said. “Those two things can seem to be at odds.”
The Navajo Nation, the country’s largest tribal jurisdiction with around 170,000 residents, has long been a focal point and challenge for IHS. The reservation is served by four of the agency’s 22 hospitals, but pockets within its 27,000 square miles of mountains and high desert have no cellphone service, internet access or electricity, creating hurdles for clinicians when it comes to communicating information and delivering care.
These structural issues had a devastating effect at the start of the pandemic, when the reservation’s rates of COVID-19 infections, hospitalizations and deaths were among the highest in the country. The virus claimed the lives of at least 2,300 Navajo citizens.
In the previous decade, vaccination rates among Navajos, especially for MMR and the flu, had regularly exceeded figures for the nation overall. They also exceeded rates for tribal communities in other regions served by IHS, which typically lagged behind the national average, according to the agency’s data. When the COVID-19 vaccine arrived in 2021, Native Americans’ uptake exceeded 60%, an effort bolstered by IHS public service messages and outreach.
On the Navajo Nation, IHS hospitals posted messages on their Facebook pages and circulated flyers that pushed community members to get the shots. “Protect yourself, protect your family, protect your elders,” the flyers said. Tribal members responded, arriving at clinics in droves, lining up in their vehicles to get vaccinated at hospitals and clinics.
For those who couldn’t travel to larger towns on the reservation that had health care facilities, teams working for IHS, the tribe and Johns Hopkins set up mobile clinics and made home visits to especially remote communities.
After the pandemic, IHS and tribal teams on the Navajo Nation sought to extend the COVID-19 shot success to routine vaccines. MMR immunization rates among 2-year-olds had dropped to 85%, but another coordinated effort restored communities on the reservation to prepandemic levels.
IHS was the engine driving the campaign, said Hammitt, the Johns Hopkins doctor. Agency flyers and Facebook posts retooled appeals used to promote COVID-19 shots to endorse the MMR vaccine, adding a call to protect “future generations.”
In the first few months of this year, however, the messaging began to morph again, with mentions of “measles” and “COVID” disappearing from IHS social media pages.
The weeks leading up to flu season and the new school year typically usher in a robust vaccine campaign in IHS hospitals. But this year, doctors took note of how few notices went out, they said, as New Mexico continued to contend with the measles outbreak that began in Texas and the Navajo Nation encountered a late-summer surge in COVID-19 cases.
One exception came in May, when IHS officials shared a New Mexico Department of Health alert on Facebook saying measles had reached Sandoval County, which overlaps with the eastern flank of the Navajo reservation. Another came that same month, when the IHS hospital in the town of Gallup, New Mexico, announced a clinic for people who wanted to get vaccinated for measles.
The IHS hospital in Shiprock, New Mexico, was the only facility to post a public service announcement about a back-to-school vaccine clinic for children. It included language telling patients to talk to doctors about their options and didn’t specifically mention measles, COVID-19 or any other infectious disease as such announcements had in the past.
Another measles outbreak surfaced in the Southwest in mid-August, this time just to the west of the Navajo Nation along the Arizona-Utah border. In early November, it had grown to at least 200 confirmed cases, according to Arizona and Utah health officials. IHS didn’t issue any advisories or notices on Facebook about this outbreak. The new approval processes for greenlighting public health alerts slowed down local administrators’ and hospitals’ response, the clinicians who spoke to ProPublica noted.
Several clinicians said the restrictions on vaccine-related speech alter the relationship between IHS doctors and patients, even if they apply only to public communications and not to one-on-one consultations.
“This is what we do for a living, and the most important thing we do is explain what’s going on to patients,” one of the doctors said. “If there is an external body interfering with that, as there is now, then that is shaping the fundamental trust between patients and the people trying to provide their care.”
On Nov. 13, a small team of advocates for people with disabilities stepped through White House security and into the narrow, bustling corridors of the West Wing, unsure what to expect. They’d managed to get a short meeting with James Blair, who is one of President Donald Trump’s deputy chiefs of staff, in the hopes of preventing a planned policy change. In recent weeks, ProPublica and The Washington Post had reported that officials at the Social Security Administration were working on a proposed regulation that could result in at least 830,000 mostly older blue-collar workers being denied disability benefits.
The advocates, led by Jason Turkish, co-founder of the Social Security disability rights group Alliance for America’s Promise, had sent the White House team ProPublica’s Oct. 31 article and other materials. The reporting showed that if the Trump administration enacted this regulation, the harm would disproportionately fall on some of the president’s most loyal supporters: 50- to 60-year-old coal miners, factory workers and other manual laborers, especially in West Virginia, Arkansas, Kentucky, Mississippi and Alabama. The administration’s logic for cutting these workers’ eligibility was that even if they have a severe physical disability, they should be able, in the modern economy, to find a more sedentary job at a computer or perhaps driving for Uber or DoorDash. Disability advocates countered that people who’ve worked in grueling fields for decades, some of whom don’t have a high school education — and who grew up before the digital age — would face severe obstacles to such a career change, including age discrimination in the hiring process, the lack of desk jobs in rural areas and the difficulty of mastering unfamiliar skills at this point in their lives.
A few doors down from the Oval Office, Turkish and his colleagues turned a corner into Blair’s office. Sitting across from him was a second person, one the advocates hadn’t expected to encounter: Russell Vought, the powerful White House budget director. He looked displeased.
After several minutes of dialogue about the disability regulation, according to Turkish and another person present, Vought said, “I know that this is being written about.” But, he added, the rule change “isn’t going to be happening.”
It was a startling announcement from an often uncompromising senior official in an administration with little history of changing its mind in response to journalistic scrutiny and pressure from advocates for the vulnerable. But that’s what Turkish and three other sources say has happened: The Trump administration has decided not to pursue the disability cuts that it has been working on all year — and in fact since at least 2019, when officials during Trump’s first term were close to finalizing a similar regulation.
Turkish, who is also president and managing partner of one of the nation’s largest law firms that represents disability claimants and beneficiaries, said in an interview that Vought and Blair seemed to have absorbed the recent reporting on the issue. He said they acknowledged the anxiety that disabled workers were experiencing — people like Christopher Tincher, a former coal miner who lost his leg on the job at a wastewater treatment facility in Arkansas and was featured in ProPublica’s story. Both officials were unambiguous, Turkish and another person present confirmed, that the regulation would not proceed in any form.
Turkish’s takeaway is that in the West Wing, vulnerable Americans with disabilities like Tincher don’t get talked about enough. “To have his story read by senior White House staffers, to remember what this program is, to remember that Social Security disability is not partisan,” was crucial, Turkish said.
Afterward, they walked out together, back through the corridors, and Vought was walking in the same direction. He didn’t say another word the whole way, according to one of the people present.
Spokespeople for the Social Security Administration and the White House Office of Management and Budget did not respond to questions from ProPublica, including whether they would contest the advocates’ assertion that the planned regulation has been nixed. A top Social Security Administration official confirmed in a meeting yesterday that the regulation has indeed been called off, according to a person present. It’s not clear why officials have said this in meetings, including with advocates, but haven’t made any public announcement.
At the White House meeting, according to two participants, Blair told Turkish to go to Frank Bisignano, the commissioner of the Social Security Administration, and “ask him point blank” if the regulation is in fact no longer being pursued.
On Tuesday, Turkish said, he did just that and met with Bisignano. Also present at this second meeting were the longtime lobbyist Andrew Woods as well as Mark Steffensen, the Social Security Administration’s general counsel. Bisignano, according to both Turkish and Woods, asked them what the White House had said about the disability issue — and he, too, “decisively” confirmed that the regulation would not proceed.
The commissioner, they said, made clear that his focus is on modernizing the Social Security Administration, not cutting disability benefits. “I take him at face value,” Turkish said, adding that Bisignano may not have been actively involved in crafting or discussing the regulation and decided against pursuing it when it “reached his level.”
Turkish and Woods say Bisignano told them to convey to the disability advocacy community that “there is no daylight between this office and the White House with respect to us not moving forward” with the regulation. On Monday, Bisignano should be able to tell them that himself: He’s considering participating in a town hall with advocates and people with disabilities.
Turkish has told other advocates in a group email that his organization will “remain vigilant to ensure these assurances are honored.”
The regulation that the Trump administration had been drafting — which remains listed on a federal bulletin with a scheduled publication date in December — would have made two major changes to the Social Security Administration’s disability system, according to four officials from the agency who had knowledge of the plans. First, it would’ve modernized the job listings that Social Security’s disability adjudicators use to decide if there’s work available in the U.S. economy that a manual laborer could still do despite physical impairments. This proposed change, which would’ve updated severely outdated jobs data, arose from a bipartisan effort that’s been in the works since the Obama administration.
The second provision was the controversial one. It would’ve almost entirely removed age as a criterion in these decisions, making a disabled 50-plus-year-old no more eligible for assistance than a 20-something. This would have had collateral effects: Losing eligibility for disability would block such workers’ access to Medicare, which they’re currently eligible for at an earlier age precisely because they’re disabled. And if workers were to be increasingly denied benefits in their 50s, many would be forced to draw down any savings they have, which could lead them to apply for Social Security’s retirement benefits early, in turn diminishing their and their spouses’ benefits until they die.
New polling by a Trump-aligned firm has suggested that older Trump voters would overwhelmingly oppose such changes to disability eligibility. In the wake of Democrats’ strong showing in recent elections, two people with knowledge of the situation said that the administration may have been particularly sensitive to these views. As one lobbyist put it, it’s all about the “elevation of an issue, and getting it on the right desks.”
Decades of progress in HIV treatment and prevention in the United States is being derailed by the Trump administration, public health experts say — and without reversing course, the damage will be devastating. Threats to key federal programs are unfolding just as science has significantly advanced how easily patients can treat and manage HIV — leaving experts deeply frustrated.
Chandra Hassan, an associate professor of surgery at the University of Illinois Chicago (UIC) College of Medicine, spent three weeks in Gaza in January 2024, treating patients who had survived tank shelling, drone strikes, and sniper fire amid Israel’s ongoing genocide. When Nasser Hospital in Khan Younis came under siege, Hassan and the MedGlobal doctors he was serving with were forced to flee. “We were evacuated when they bombed just across the street from the hospital [and] tanks were rolling in,” Hassan told Truthout.
When Hassan returned home to Chicago, he was eager to share his experiences and advocate for an end to Israel’s assault on Gaza, which has killed an estimated 68,000 Palestinians since October 2023.
US President Donald Trump and his Republican allies in Congress have made a show of criticizing insurance company greed as they stand firm against extending Affordable Care Act tax credits and offer ill-formed alternatives. But a report published Wednesday by the office of Sen. Ron Wyden (D-Ore.) explains how a scheme endorsed by Trump and some top Republicans would further enrich insurance…
Tierra Walker had reached her limit. In the weeks since she’d learned she was pregnant, the 37-year-old dental assistant had been wracked by unexplained seizures and mostly confined to a hospital cot. With soaring blood pressure and diabetes, she knew she was at high risk of developing preeclampsia, a pregnancy complication that could end her life. Her mind was made up on the morning of Oct.
San Diego — As 40,000 AFSCME Local 3299 workers throughout the ten-campus University of California system launched a two-day strike on Nov. 17, two Communist Party members—Alvin, an AFSCME-represented employee at University of California at San Diego (UCSD), and another worker, an AFSCME retiree from UC San Francisco—shared their thoughts before they prepared to picket.
Pay, or lack of it, is the big issue. But so is disparate treatment on a class basis.
While the university system fails to settle contracts addressing the cost of living and affordability crises facing its most economically vulnerable patient care workers, it’s also handed out six-figure salaries and housing subsidies to multiple high administrators.
Tierra Walker had reached her limit. In the weeks since she’d learned she was pregnant, the 37-year-old dental assistant had been wracked by unexplained seizures and mostly confined to a hospital cot. With soaring blood pressure and diabetes, she knew she was at high risk of developing preeclampsia, a pregnancy complication that could end her life.
Her mind was made up on the morning of Oct. 14, 2024: For the sake of her 14-year-old son, JJ, she needed to ask her doctor for an abortion to protect her health.
“Wouldn’t you think it would be better for me to not have the baby?” she asked a physician at Methodist Hospital Northeast near San Antonio, according to her aunt. Just a few years earlier, Walker had developed a dangerous case of preeclampsia that had led to the stillbirth of her twins.
But the doctor, her family said, told her what many other medical providers would say in the weeks that followed: There was no emergency; nothing was wrong with her pregnancy, only her health.
Just after Christmas, on his birthday, JJ found his mom draped over her bed, lifeless. An autopsy would later confirm what she had feared: Preeclampsia killed her at 20 weeks pregnant.
Every day, JJ revisits photos and videos of his mom.
Walker’s death is one of multiple cases ProPublica is investigating in which women with underlying health conditions died after they were unable to end their pregnancies.
Walker had known that abortion was illegal in Texas, but she had thought that hospitals could make an exception for patients like her, whose health was at risk.
The reality: In states that ban abortion, patients with chronic conditions and other high-risk pregnancies often have nowhere to turn.
They enter pregnancy sick and are expected to get sicker. Yet lawmakers who wrote the bans have refused to create exceptions for health risks. As a result, many hospitals and doctors, facing the threat of criminal charges, no longer offer these patients terminations, ProPublica found in interviews with more than 100 OB-GYNs across the country. Instead, these women are left to gamble with their lives.
As Walker’s blood pressure swung wildly and a blood clot threatened to kill her, she continued to press doctors at prenatal appointments and emergency room visits, asking if it was safe for her to continue the pregnancy. Although one doctor documented in her medical record that she was at “high risk of clinical deterioration and/or death,” she was told over and over again that she didn’t need to worry, her relatives say. More than 90 doctors were involved in Walker’s care, but not one offered her the option to end her pregnancy, according to medical records.
Walker’s case unfolded during the fall of 2024, when the dangers of abortion bans were a focus of protests, media coverage and electoral campaigns across the country. ProPublica had revealed that five women — threein Texasalone — had died after they were unable to access standard reproductive care under the new bans.
ProPublica condensed more than 6,500 pages of Walker’s medical records into a summary of her care with the guidance of two high-risk pregnancy specialists. More than a dozen OB-GYNs reviewed the case for ProPublica and said that since Walker had persistently high blood pressure, it would have been standard medical practice to advise her of the serious risks of her pregnancy early on, to revisit the conversation as new complications emerged and to offer termination at any point if she wanted it. Some described her condition as a “ticking time bomb.” Had Walker ended her pregnancy, every expert believed, she would not have died.
Many said that her case illustrated why they think all patients need the freedom to choose how much risk they are willing to take during pregnancy. Walker expressed that she didn’t want to take that risk, her family says. She had a vibrant life, a husband and son whom she loved.
Under Texas’ abortion law, though, that didn’t matter.
Walker’s mother, Pamela Walker, holds her daughter’s ashes.
“I Don’t Know How Much More I Can Take”
On a hot September day, Walker was lying down with JJ after a walk with their two small dogs, Milo and Twinkie, when she started shaking uncontrollably.
Terrified, JJ called 911, asking for an ambulance.
As the only child of a single mom, JJ had always considered Walker his closest friend, coach and protector wrapped in one. In their mobile home, JJ was greeted each morning by his mom’s wide smile and upturned eyes, as she shot off vocabulary quizzes or grilled him on state capitals. He loved how fearlessly she went after what she wanted; in 2021, she had proposed to her boyfriend, Eric Carson, and the two eloped. She’d just been talking about moving the family to Austin for a promotion she was offered at a dental clinic.
Eric Carson and Walker married in 2021.
At the hospital, JJ was shocked to see her so pale and helpless, with wires snaking from her head and arms.
To Walker’s surprise, doctors quickly discovered that she was five weeks pregnant. They also noted hypertension at levels so high that it reduces circulation to major organs and can cause a heart attack or stroke. That, and her weight, age and medical history, put Walker at an increased risk of developing preeclampsia, a pregnancy-related blood pressure disorder, said Dr. Jennifer Lewey, director of the Penn Women’s Cardiovascular Health Program and expert in hypertension.
“If I’m seeing a patient in her first trimester and her blood pressure is this uncontrolled — never mind anything else — what I’m talking about is: Your pregnancy will be so high risk, do we need to think about terminating the pregnancy and getting your health under control?”
As Walker’s first trimester continued, she kept seizing. Her body convulsed, her eyes rolled back and she was often unable to speak for up to 30 minutes at a time. Some days, the episodes came in rapid waves, with little relief.
For three weeks, she stayed at Methodist hospitals; doctors were not able to determine what was causing the spasms. Walker couldn’t get out of bed, in case a seizure made her fall, and this left her vulnerable to blood clots. She soon developed one in her leg that posed a new lethal threat: It could travel to her lungs and kill her instantly.
Carson watched over her during the day and her aunt Latanya Walker took the night shift. She was panicked that her tough niece, whose constant mantra was “quit your crying,” now seemed defeated. One evening, during Walker’s third hospitalization, when she was about 9 weeks pregnant, she told Latanya she’d had a vision during a seizure: Her grandmother and aunt, who had died years earlier, were preparing a place for her on the other side.
“You better tell them you’re not ready to go,” Latanya said.
“I don’t know how much more I can take of this,” Walker whispered.
Walker’s aunt, Latanya Walker, tried to advocate for her niece during her hospitalizations.
The next morning, Walker called for a doctor and asked about ending her pregnancy for the sake of her health. “When we get you under control, then everything will go smoothly,” the doctor replied, Latanya recalled. The physician on the floor was not an OB-GYN with the expertise to give a high-risk consultation, but the Walkers didn’t realize that this mattered. By the time the doctor left the room, her aunt said, tears streamed down Walker’s cheeks.
Dr. Elizabeth Langen, a maternal-fetal medicine specialist in Michigan who reviewed Walker’s case, said a physician comfortable with high-risk pregnancies should have counseled her on the dangers of continuing and offered her an abortion. “The safest thing for her was to terminate this pregnancy, that’s for sure.”
During Walker’s many hospital and prenatal visits, 21 OB-GYNs were among the more than 90 physicians involved in her care. None of them counseled her on the option — or the health benefits — of a termination, according to medical records.
In Texas, the law bars “aiding and abetting” an illegal abortion. As a result, many physicians have avoided even mentioning it, according to interviews with dozens of doctors.
In her condition, Walker couldn’t fathom leaving the state. When her aunt suggested ordering abortion medication online, Walker was worried she could go to jail. She was spending so much time in the hospital; what if she got caught taking the pills?
At 12 weeks pregnant, she was admitted to University Hospital. Doctors there noted that even on anticoagulation medication, the clotting in Walker’s leg was so profound that she needed a thrombectomy to remove it.
“At this point, we’ve gone from ‘complicated, but within the realm of normal’ to ‘we’ve got someone with a major procedure in pregnancy that tells us something isn’t going well,’” said Dr. Will Williams, a maternal-fetal medicine specialist in New Orleans, where an abortion ban is also in place. “In my practice, we’d have a frank discussion about whether this is a person we’d offer a termination to at the point of thrombectomy.”
ProPublica reached out to five physicians who were involved in key moments of Walker’s care: the hospitalist on duty on Oct. 14, 2024, when she asked about ending her pregnancy; three OB-GYNs; and a hospitalist on duty at the time of her thrombectomy. They did not respond. The hospitals Walker visited, including those run by University Health System and Methodist Healthcare, which is co-owned by HCA, did not comment on Walker’s care, despite permission from her family. Although the Walkers have not pursued legal action, they have engaged a lawyer. A University Health System spokesperson said that it is the company’s policy not to comment on potential litigation.
In her second trimester, Walker’s seizures continued and her hypertension remained out of control. At an appointment on Dec. 27, at around 20 weeks, a doctor noted spiking blood pressure and sent her to University Hospital’s ER. There, doctors recorded a diagnosis of preeclampsia.
The experts who reviewed Walker’s vital signs for ProPublica said her blood pressure of 174 over 115 was so concerning at that point, she needed to be admitted and monitored. Most questioned her doctor’s choice not to label her condition as severe. The treatment for severe preeclampsia, which points to a problem with the placenta, is delivery — or, at 20 weeks, an abortion.
Instead, doctors lowered her blood pressure with medication and sent her home.
Carson in the bedroom he shared with Walker
Three days later, JJ crawled into bed with his mom and fed her soup. “I’m so sorry,” Walker croaked. “It’s your birthday and it shouldn’t be like this.”
He told his mom it was okay. He hadn’t expected laser tag or a trip to Dave & Buster’s this year. Over the past few months, when his mom was home, he had tried his best to make things easier on her, walking the dogs when she was out of breath, checking in every hour or so with a hug. JJ knew that after missing so many days of work, she had lost her job. She was stressed about getting enough food for the house. He was relieved when he heard her snoring — at least she was resting.
That afternoon, when his stepdad was out grocery shopping and his grandmother was just getting back from dialysis, he cracked open the door to Walker’s room.
His mom was lying face-down in bed, as if she had fallen over while getting up. JJ ran over and tried to find any sign she was breathing. When he called 911, a dispatcher coached him to slide her to the rug and start CPR.
“I need you,” he shouted as he leaned over his mom, pressing down on her chest. “I need you!”
JJ receives prayers at church in San Antonio.
“We Have to Allow for More Exceptions”
The anti-abortion activists who helped shape America’s latest wave of abortion bans have long seen health exemptions as a loophole that would get in the way of their goals. They fear such exceptions, if included in the laws, would allow virtually anyone to terminate a pregnancy.
In Idaho, an anti-abortion leader testifying at a state Senate hearing suggested doctors would use health exceptions to give abortions to patients with headaches.
In South Dakota, a pregnant Republican lawmaker with a high risk of blood clots begged her colleagues to consider creating a health exception that would protect her; her bill never made it to a hearing.
In Tennessee, an anti-abortion lobbyist with no medical training fought and defeated an amendment to the state law that would allow a health exception to “prevent” an emergency. He testified in the state Capitol that the carve-out was too broad since some pregnancy complications “work themselves out.”
The refusal to entertain these broader exceptions is particularly consequential given the state of women’s health. Women are entering pregnancy older and sicker than they have in decades. The rate of blood pressure disorders in pregnancy has more than doubled since 1993; they now affect up to 15% of U.S. pregnancies. And they’re most prevalent in states with restrictive abortion policies, according to a 2023 study in the Journal of the American College of Cardiology. The burden of disease falls heaviest on Black women, like Walker, for an array of reasons: neighborhood disinvestment, poor access to health care and discrimination in the medical system. Cuts to Medicaid funding and changes to the Affordable Care Act are likely to exacerbate these problems, according to experts.
Other countries give pregnant women and their doctors far more control over the medical decision to terminate. Across Europe, for example, most laws permit abortion for any reason through the first trimester, when more than 90% of abortions occur. After that gestational limit, their statutes also tend to include broad health exceptions that can be used for chronic conditions, illnesses that develop in pregnancy, fetal anomalies and, in some countries, mental health.
U.S. abortion bans generally restrict interventions to a far more limited set of health risks, like a “life-threatening medical emergency” or “substantial and irreversible” harm to major organs. A small subset of lawyers and doctors argue that the law can and should be interpreted to cover patients with chronic conditions that are worsening in pregnancy. But the vaguely written bans threaten criminal penalties for performing an illegal abortion — in Texas, up to 99 years behind bars. In practice, few hospitals grant health exceptions, ProPublica’s reporting has found.
Dr. Jessica Tarleton, an OB-GYN who provides abortions in South Carolina, recalled how much changed at her hospital when the state’s ban was put in place: OB-GYNs who want to provide an abortion to a patient with a health risk now need to get a maternal-fetal medicine specialist to explicitly write in the chart that it is necessary, in compliance with the law. Not many doctors are willing to do so.
“Some people were not because of their personal beliefs, and some because they didn’t want to be involved in any kind of potential legal actions,” Tarleton said. “They didn’t want their opinion to have anything to do with a patient getting an abortion or not.”
Recently, for example, Cristina Nuñez sued two hospitals in El Paso for their inaction in her care in 2023. She had diabetes, uncontrolled blood pressure and end-stage kidney disease when she learned she was unexpectedly pregnant at 36. Doctors wrote in her medical record that “she needs termination based on threat to maternal life or health,” but Nuñez alleged that one hospital failed to find an anesthesiologist willing to participate. She remained pregnant for weeks, even as blood clots turned her right arm black, until an advocacy organization threatened legal action and she was able to obtain an abortion. The lawsuit is ongoing.
This year, Texas Republicans passed legislation with minor amendments to their ban after ProPublica reported the deaths of three miscarrying women who did not receive critical abortion care during emergencies. In the updated law, an emergency still needs to be “life-threatening” to qualify for an abortion, but it no longer needs to be “imminent.” Doctors expect that most hospitals still won’t provide abortions to women like Walker who have dangerous chronic conditions but no certain threat to their lives.
ProPublica asked Sen. Bryan Hughes, the author of Texas’ abortion ban, about how the specific complications Walker faced should be treated by doctors under the amended law. When her pregnancy began, would she be eligible for an abortion due to her health? Would she need to wait for a diagnosis of severe preeclampsia? Is there a reason the law doesn’t include an exception for health risks? ProPublica put the same questions to the 20 state senators who co-wrote the bipartisan amendment.
Only Sen. Carol Alvarado, a Democrat, responded. In her view, the amendment was far too narrow. But, she said, her Republican colleagues defer to the far right of their base and oppose broader exceptions.
“You can’t proclaim to be pro-life, but you’re passing laws that are endangering women and causing death,” she said. “We have to allow for more exceptions.”
Latanya and Pamela in San Antonio
“So You’d Rather Let Somebody Die?”
After Walker died, her family felt bewildered by her medical care. The doctors had assured them that her baby was healthy and she would be fine. The autopsy found that the fetus was indeed healthy, at just under a pound and measuring 9 inches long. But it showed that Walker had hypertensive cardiovascular disease with preeclampsia, along with an enlarged heart, dangerously full of fluid, and kidney damage — signs that her condition had declined even more than she knew.
In Carson’s mind, the many doctors they saw cast the risks as challenges that would be overcome if his wife followed directions. “She was doing what they told her to do,” he said. He couldn’t understand how no one suggested ending the pregnancy to keep Walker safe. “Nobody said nothing.”
Latanya worried the law played a role. “They didn’t want to offer to end the pregnancy, because the government or someone says you can’t? So you’d rather let somebody die?” she said. “Now we are the ones that have to suffer.”
JJ couldn’t bear to stay in the home where he had found his mom, so he moved in with Latanya. Each day, he scrolls through old videos on the computer so he can hear Walker’s voice.
Latanya does everything she can to support him, but she knows she can’t erase his pain.
She recalls watching JJ steady himself at Walker’s funeral, to see her one last time. Until that point, he hadn’t cried.
When he finally faced the open casket where his mom lay holding her fetus, JJ sank to his knees, overcome. His aunt, uncles, cousins and grandmother gathered around him and rocked him in their arms.