
Water became a commodity traded on Wall Street in December amid fear of scarcity, and now oxygen is being speculated on in Mexico.
With most hospitals full, many Mexicans are battling COVID-19 at home. Oxygen tanks and oxygen concentrators (devices that concentrate the oxygen from a gas supply, typically the air) have become scarce, as individuals and companies are taking advantage of the pandemic and selling or renting them at extremely high prices. Others are using the situation to fraudulently sell tanks without delivering them, or to steal customers’ personal information. The situation is only compounding the debt, poverty and inequality that has worsened with the pandemic. It also portends a new wave of fraud and speculation, when vaccines arrive.
At the time of writing, Mexico had registered 160,000 deaths from COVID-19. However, Mexico’s emergency service says the real figures are at least three times that, given how many people are dying at home, and given that testing — especially outside of the capital, Mexico City — is expensive and difficult to access.
In Mexico City, people have been lining up for up to five hours to refill tanks, many of which only provide a few hours’ worth of oxygen. The demand for oxygen has grown by 700 percent over the past month, according to the Office of the Federal Prosecutor for the Consumer (PROFECO).
People have turned to social networks to try to find oxygen supplies, using lists compiled informally by individuals, as the government is not providing such information. Most of the companies or names on these lists are part of an underground market, and the minister for internal affairs, Olga Sánchez, says crime networks are getting involved.
Speculating With Human Lives
I contacted various numbers on a list for the city of Puebla to confirm whether the owners of the listed numbers were speculating, and under what conditions they were supplying oxygen products. Many of them never replied. I wrote to someone identifying as Andres Madrid on Twitter, who was advertising oxygen concentrators for sale in Puebla. He said he was selling six-liter concentrators for 30,000 pesos (US$1,484), but when I asked if he represented a laboratory or where he got the concentrators from, he stopped replying.
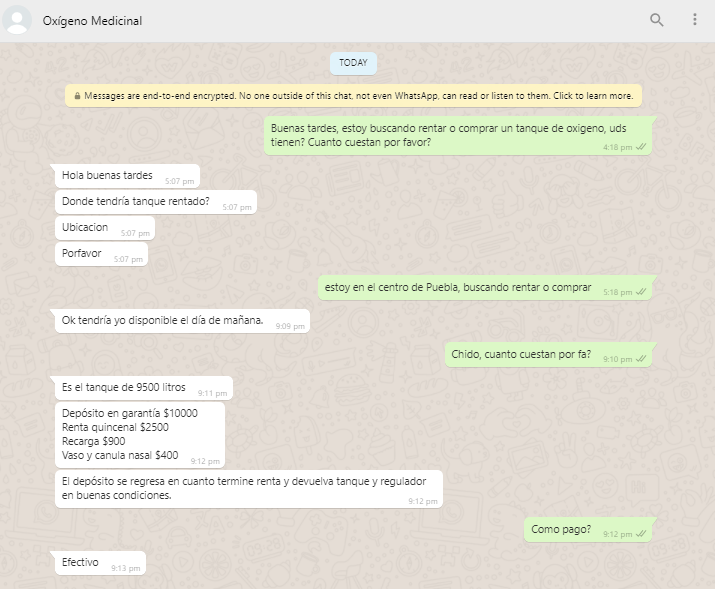
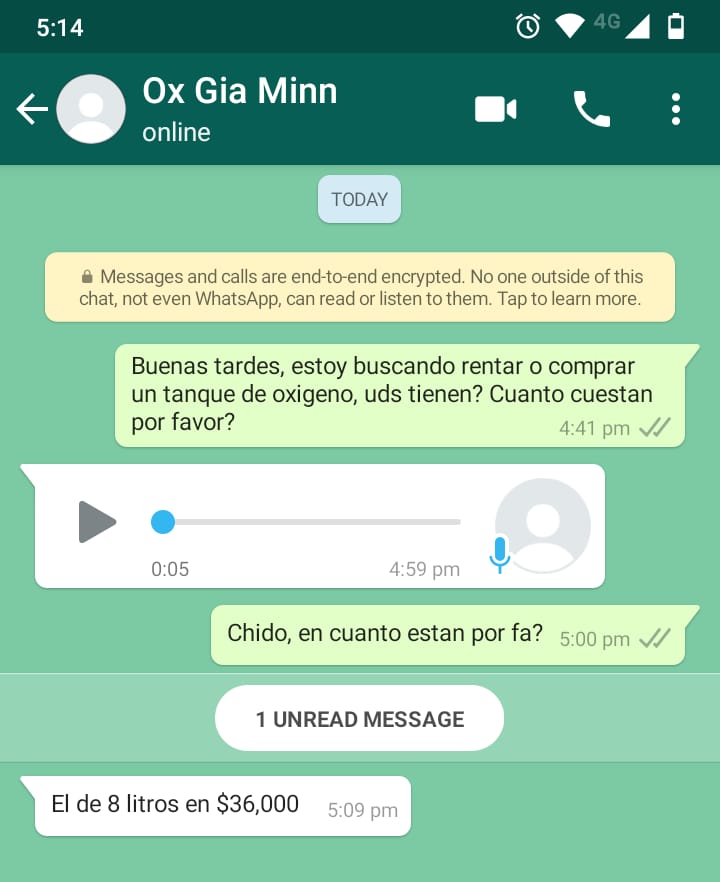
Another supplier asked for a 10,000 peso deposit (US$495) and would only accept cash, while another was selling a normal eight-liter tank for 36,000 pesos (US$1,782). Those only accepting cash likely didn’t want any records of the transactions.
The figures represent roughly a quadrupling of prices since November. The National Alliance for Small Businesses (Anpec) stated that an oxygen refill has gone from 250 pesos in December, to 690 pesos on average today, while concentrators used to cost 11,000 pesos, and on average are being sold for 60,000 pesos. In most of Mexico, the minimum wage is 123 pesos per day, though many informal workers don’t earn that much. Such prices mean people having to pay up to 20 months’ wage for an oxygen concentrator.
Given the demand and profit rates, it is no surprise that there have been incidences of people intercepting trucks delivering oxygen tanks and stealing all of them, and that police escorts sometimes have to be provided when oxygen is being transported.
There are numerous Twitter accounts and fake websites selling oxygen tanks. Some are being used to commit fraud and obtain people’s personal and banking details; many involve using stolen IDs when sending quotes to customers, and others ask for an advance payment and then don’t follow through.
PROFECO acknowledges that the situation is serious. The head of the office, Ricardo Sheffield, says the agency has already deactivated 700 Facebook profiles and 100 pages involved in the fraudulent sale of oxygen. He also noted that some companies sell industrial oxygen tanks that aren’t medical grade and thus not fit for personal use, and told people to only buy from officially recognized companies like INFRA, Linde or Air Liquide.
INFRA is a producer and distributor of industrial gases and welding materials, but is also one of the main suppliers of medicinal oxygen. I visited one of its stores in Puebla. People were lining up in cars going back almost three blocks. I wondered what the majority of people, who don’t own cars, were doing to transport tanks — which are extremely heavy.
One person waiting for a refill, Antonia Garcia, said, “At first, it was hard because you don’t know where to get oxygen, and then you find out about the different shops, but then you don’t have a tank to refill. We had to buy a tank — it cost 30,000 pesos. It was full, but then we have to fill it up every day, and that costs 470 pesos. We are shopkeepers and we covered the costs between the whole family, but I don’t know what other people do. You wouldn’t be able to pay it because it costs a lot.”
Gloria Gonzalez, who was refilling a tank for her sick grandmother, said, “We asked friends and we went on social media asking for tanks. They are very hard to get, and in the end, we borrowed one. The prices keep going up. The tiny one we’re using costs 6,000 pesos and you have to refill it a few times a day. It’s very stressful, and it’s very sad.”
Given the under-the-table nature of the underground market, and the lack of studies or reporting into the situation, it is hard to quantify the impact this is having. However, there is no doubt that many people are going into debt to buy oxygen tanks, to pay bills and rent, or even just to get COVID-19 tests. And the loans are likely coming from friends or organized crime, as government credit or banking loans are inaccessible for most.
Local media reported that in one hospital in southern Puebla, four patients died after a private contractor didn’t provide the necessary quantity of oxygen, and around the country, 40 percent of people say that they or a family member have now lost all of their income due to the pandemic and its impacts.
Violence and Inequality in Underground Markets
This new underground market and the other crimes only flourish because of already existing black-market structures, organized crime and inequality. The U.S.’s Merida Initiative — an agreement with Mexico and Central America to combat cross-border crime, drug trafficking and money laundering — and the “war on drugs” saw a drastic militarization of Mexico, massive increases in drug prices, an intensification of organized gangs and cartels, increased extortion and an arms black market estimated to be worth US$100 million.
And with unreliable water and health care systems, there are underground markets flourishing in those sectors as well. For those who can’t access any or enough water, there is a private market of water trucks selling water at elevated prices, while in 2018, Mexico had the sixth-largest medicine black market in the world.
The pandemic has only seen that worsen, as surgeries are being canceled. There is an increased demand for cancer medications, and in Mexico City, for example, 38,000 of such medicines were stolen from storage by armed men.
Some 57 percent of the working population are informal workers and therefore not registered for social security, and only 14 percent of second-level hospitals* attend to such people. On top of that, high levels of corruption in the sector mean health resources (from medicine to machines) are diverted into the coffers of private companies. In 2016, at least 6 billion pesos (US$295 million) worth of federal resources assigned to Seguro Popular (public health insurance that covers a wide range of services without co-pays for its affiliates) were mismanaged.
Corruption also means many hospital buildings contracts were never completed. The disastrous state of Mexico’s health care system, combined with the pandemic and a lack of official information, means that many people feel desperate and helpless when they contract COVID-19. They often don’t investigate or ask questions, because it is better not to know, and many are highly susceptible to social media scams.
Is the Global Vaccine Market Next?
In Mexico, there have already been various instances of people trying to profit from the demand for vaccines. Though currently only available through a government program, Mexico has said private companies will be allowed to import the vaccine.
Meanwhile, the federal health commission, COFEPRIS, is already worried about fake sales of the AstraZeneca vaccine. In the states of Guanajuato and Quintana Roo, there were reports of people visiting houses or calling and asking for personal information with the vaccine as the pretext. One website pretended to be Pfizer Mexico and tried to sell a fake vaccine, and people have tried to sell fake vaccines through social networks.
This issue isn’t limited to Mexico. The inequality experienced here is also reflected on a global scale; wealthy countries hoarding vaccines will lead to insecurity and deep economic problems that will end up impacting them as well, since poorer countries tend to manufacture and produce a lot of the goods that wealthier countries use.
Interpol warned of the potential for organized crime related to vaccines, as the pandemic has “already triggered unprecedented opportunistic and predatory criminal behavior.”
Already, 2 billion people globally lack access to medicines and medical devices, which leaves a gap that is often filled by substandard and falsified products. Up to 169,000 children die yearly from pneumonia after receiving counterfeit drugs, and the figure is similar for adults for fake anti-malarial medication.
While high-income countries so far have 60 percent of the vaccines (but only 16 percent of the world’s population), the European Union has confirmed it will control vaccine exports in order to put its citizens first. But World Health Organization Director-General Tedros Adhanom Ghebreyesu says, “We will not end the pandemic anywhere until we end it everywhere.”
* Mexico has three levels of health care. The first is preventative, emergency etc. The second is the biggest area and covers most health issues that involve hospitalization, such as surgeries, urgent care, as well as children and gynecology. The third level is specialist care.
This post was originally published on Latest – Truthout.








{kind=link}
{kind=link}
{kind=link}