As New Zealand marks two years of living with covid-19, 14,633 new community cases of the virus were announced yesterday alone and a total of 56 people have died from it.
In a statement, the Ministry of Health said there were also 344 community cases of the cases in hospital and five in ICU.
Lowest death rate in OECD
Epidemiologist Professor Michael Baker of Otago University said this country still had the lowest death rate from covid-19 in the OECD by a large margin.
“The pandemic is now thought to have killed about 20 million people across the globe,” he said.
“And they’re mainly in countries where, obviously, they’ve had limited resources, or they’ve had very poor leadership from the governments.
“It’s interesting to see, in somewhere like Russia, the pandemic has now killed almost 0.8 percent of the entire population.”
The centre reported more than 435 million cases of the virus and 5.9 million deaths globally.
Professor Baker said he was still optimistic about the future, highlighting that life expectancy in New Zealand had risen by about eight months over the course of the pandemic — one of the only countries in which this has happened.
Russian life expectancy dropped
By comparison, the life expectancy of Russian residents had dropped by about two years, he said.
“We haven’t seen those kinds of impacts since the Second World War.”
Professor Baker said the outbreak would peak over the next month before declining. He warned that New Zealand would see tens of thousands of new infections every day, and the total number of people with covid-19 was likely to be much higher than the number of people that get tested.
However, he said New Zealand had fared well compared to other countries.
“By delaying the arrival of the omicron variant, it’s given us a good opportunity to get highly vaccinated and boosted. And also, we have what is called peak immunity, because we’ve had our vaccine doses and boosters very recently and that means we’re ready to meet this virus with a lot of antibodies.”
The Ministry of Health said more than two thirds of eligible New Zealanders had now had their booster dose, with 28,836 people receiving their boosters on Saturday.
Four people were arrested at the Parliament grounds anti-covid public health protest overnight — two for breaking bail conditions, one for possessing an offensive weapon and one for trespass.
Police said the number of protesters had shrunk to about 200 people.
This article is republished under a community partnership agreement with RNZ.
Auckland Mayor Phil Goff says council has trespass orders “ready to go” as Auckland Domain remains closed to vehicles due to a small number of anti-covid public health measures protesters refusing to leave.
The small group of protesters set up camp at Auckland Domain after walking over the Harbour Bridge for another protest organised by Freedoms and Rights Coalition at the weekend.
Goff told Morning Report everyone had a right to protest, but he hoped this was not a repeat of Wellington’s protest.
“What I absolutely oppose is a sense of entitlement and self-given right to disrupt others’ lives when people want to make their point. We’ve seen that at Parliament, we don’t want to see it in Auckland,” he said.
“People say, ‘Why don’t you talk to the protesters? Why don’t you negotiate with them?’ How do you negotiate with people in bad faith, who agree one thing and then immediately dishonour their promise?
‘They’re not entitled to disrupt lives’
“These are people that we know from a range of other protests around the city … they are not entitled to camp on the domain, they are not entitled to disrupt the lives of others as they are doing.”
Goff said he was in regular discussion with police, right up to the commissioner’s level, and had made his views clear.
“I’ve indicated that the council has trespass orders and its compliance team ready to go, as soon as police indicate they’re ready to enforce those trespass orders and remove the people, and I hope that that will happen,” he said.
“Nobody is above the law, nobody is entitled to believe they can break the law and there are no consequences and that’s what we’re seeing at the moment and I think that’s got to stop.”
Goff said he respected the independence of police on operational issues, but he did not “want to see the same sort of disruption of people’s lives and the tolerance of appalling behaviour that we’ve seen in Wellington”.
Convoy protesters install their own toilets in Wellington Meanwhile, Wellington City Council engineers have confirmed that the protesters at Parliament have plumbed toilets into the Capital’s sewer system.
A plywood structure next to the portaloos at the intersection of Molesworth and Hill streets has pipes that connect to the sewer.
Wellington Mayor Andy Foster, who has been at the site to take a look, told Morning Report he would be discussing with police as to how the protesters managed to get all the required material onto the site.
He said he had been advised by Wellington Water and people at the site that it was connected to the wastewater system.
“If they were going into the stormwater, that would be completely unacceptable. As I said, it’s unlawful to have put them into the wastewater. [If it was going into] the stormwater, [that] will be a real environmental problem, whereas the wastewater is simply an unlawful connection.”
Discussions with protesters were still ongoing to end the occupation which started earlier this month, he said.
This article is republished under a community partnership agreement with RNZ.
The Auckland Domain remained closed today to vehicles until further notice, because a small number of anti-covid protesters have set up tents there and stayed overnight.
They moved there after thousands of people crossed the harbour bridge on foot yesterday, in a march organised protest against New Zealand’s covid-19 public health measures.
The Ministry of Health reported a record 14,941 new community cases of covid-19 in New Zealand today, with 305 people now in hospital — five of them in intensive care.
Camping is not permitted in the Domain, which lies between the suburbs of Parnell and Grafton.
Auckland Council director of customer and community services Claudia Wyss said it was working with event organisers on a safety-first approach.
She said there was no timeline for reopening at this stage and the council apologised for any inconvenience.
The campers include people who took part in the march over the Harbour Bridge, shutting down southbound traffic for an hour and a half.
The march was organised by Destiny Church’s Freedoms and Rights Coalition. Leaders had been in talks with the Auckland Council and police about their presence late on Saturday, and promised to leave the site by 9pm that night.
A protester in a video has claimed to have mana whenua status, and said they were occupying a pa site at the domain.
Auckland Council said it was continuing to work with police and to engage constructively with the group.
However, it has raised concerns the marchers and protesters risked spreading covid-19 by gathering.
In New Plymouth, about seven tents and about 30 people were at an anti-covid protest beside the Coastal Walkway on Sunday morning.
Fewer people at Wellington anti-covid protest About 300 vehicles remain in the protest area inside cordons at Parliament grounds, however an RNZ reporter said some protesters appeared to be packing up this morning ready to leave.
Police are maintaining a perimeter at access routes to the area amid the sounds of reggae music and the occasional car horn. The protesters are waving flags and shouting the word “freedom”, to passing cars.
Protesters have been camping in tents and in vehicles parked in and around the protest area, which covers grounds belonging to Victoria University as well as parts of Molesworth and Hill streets.
Businesses, schools, the university and residents in the area have reported major disruption since it began on February 7.
About 200 new protesters turned up at the campsite on Saturday, but police said that was far fewer than on previous weekends.
RNZ estimates that by Sunday the number of protesters had halved from last weekend, when more than 1000 people took part.
A group called Farmers for Freedom told followers this morning via social media that a convoy it had organised would reach the protest today with a trailer of food.
This article is republished under a community partnership agreement with RNZ.
Hospitals across New Zealand are receiving anti-covid-19 mandate protesters returning from Parliament, and are pleading with those experiencing cold and flu symptoms to get tested and isolate.
There were mounting tensions at the Parliament protest today, where police have formed a line to keep protesters back.
More people have turned up in Wellington to join the event.
Officers are trying to block access for cars into the bus interchange area and are using a forklift to reposition concrete bollards.
Some protesters are driving past the area, shouting at police to leave.
Meanwhile, hospitals are now reporting visits from protesters returning from the anti-covid-19 mandate protest at Parliament, and are pleading with those experiencing cold and flu symptoms to get tested and isolate.
The Ministry of Health said hospitals throughout the country had reported visits from people who have been at the anti-mandate protest at Parliament before returning home.
Widespread disruptions
Thousands of protesters have occupied the grounds of Parliament and nearby Wellington central streets since their convoy arrived on February 7 creating widespread disruptions, with many ignoring social distancing rules and not wearing masks.
The occupation is now a location of interest after people infectious with covid-19 were confirmed to be among the crowd, and anyone who is there on the listed times and dates is asked to carefully monitor for symptoms, and follow instructions about what to do next if they have any.
In a statement today, the ministry said the protest was a potential super spreader event as the spread of omicron hit a new record of 13,606 community cases today.
Five of the 263 people in hospital with the coronavirus were in intensive care.
Early in the protest leading epidemiologist Professor Michael Baker of Otago University warned this could happen, saying people mixing with groups from outside their household, singing, eating together and sharing transport and accommodation was a recipe for the spread of omicron from those at the protest out to other communities.
Yesterday police called on protesters to take children home, saying the event was not safe for families.
More than 130 people have been arrested at the event, and media have reported Corrections has confirmed they have been monitoring a “small number” of criminals subject to GPS monitoring conditions who were at the event.
‘Reassurance patrols’
Sewage leaks and assaults have also been connected to the event.
Police are carrying out “reassurance patrols” for residents that live near the protest at parliament today, and said officers would continue to be visible at the protest site.
“The focus for police is to contain the current perimeters of the protest and continue to maintain a safe community for our Wellington residents,” they said.
This article is republished under a community partnership agreement with RNZ.
Kaniva News correspondent Patimiosi Ngūngūtau took this photo of an emotional farewell for a grieving Tongan family at the Tanoa hotel in Nukua’alofa this week.
The family requested that they stop outside the quarantine facility so that her daughter, who was in managed isolation after recently arriving from New Zealand could pay her respects to her mother, Ngūngūtau said.
The daughter can be seen grieving in a quarantine room as family console her from a distance on Tuesday.
Education Minister Chris Hipkins has warned that nearly every New Zealand school and early childhood centre will have contact with covid-19 in the next few weeks.
He told students at Mana College in Porirua today that one in five schools were already managing cases among students or staff but they were well prepared.
“We’re now up to one in five schools [which] have covid-19 cases in them and that’s going to just continue to increase from here,” he said.
“We expect in the next few weeks that just about every school, every early childhood service potentially is going to end up coming into contact with covid-19 as it spreads more rapidly throughout the community. That is now going to happen,” he said.
In a statement, the Ministry of Health said 8223 of the positive results came from Rapid Antigen Tests (RATs), while 3807 were PCR tests.
There are currently 237 people in hospital with the coronavirus, including three in intensive care.
92% of students vaccinated
Hipkins said 92 percent of secondary students were fully vaccinated, the government had 42 million facemasks on order or in the country for schools, and it was expecting 5000 air purifiers for rooms with poor ventilation.
He also said schools might get easier access to rapid antigen tests after two large orders arrived in the next two weeks.
Currently the tests were a last resort for teachers who were isolating and whose schools could not find enough teachers to safely supervise children who could not be at home, such as the children of essential workers.
“In another week or two we will have a greater supply of rapid antigen tests in the country and at that point we may be able to say actually we can be a bit more generous than that and we can provide tests in a few more circumstances than that including for what we call surveillance which is just to give you reassurance that it’s not out there,” Hipkins said.
Education Minister Chris Hipkins … Image: Angus Dreaver/RNZ
Auckland Secondary Principals Association president Steve Hargreaves said that could make a big difference as the pandemic bites.
“That’ll help keep schools open.
“Schools are having to roster year levels home and children are having to learn remotely because so many staff are tied up as close contacts, family members have test positive but they’re still well, they’ve been able to isolate successfully at home and if we can keep those teachers in schools through the use of rapid antigen tests, that’ll be good for our children.”
After-school sport
Hipkins also promised to clarify the rules around unvaccinated children’s participation in after-school sport and cultural activities.
The Education Ministry’s website said there were no limits on curriculum-related activities like PE classes, but extra-curricular events like team training at schools must be limited to 25 people if any were unvaccinated and 100 if all were vaccinated.
Hipkins said that was not the government’s intention.
“Some schools are interpreting something like a kapa haka rehearsal after school hours or sports after school hours as being included in the guidance.
“We’d never intended for that to be the case so we’re clarifying that so to make it clear that if you’re participating in a school-organised activity, that includes sports, kapa haka, those other cultural events, the vaccine requirement will not apply,” he said.
The minister’s office and the ministry were unable to confirm details and Hargreaves said that was a shame, because he had unvaccinated students ready to play sport tomorrow.
“It’s really sad because we don’t want to exclude any children from these great extra-curricular opportunities but we’ve been following the guidelines around events, gatherings and those size limits and of course College Sport Auckland has its rule around needing to be vaccinated to comply with those rules and that’s blocked a few kids from playing and the sooner we can get this tidied up the better,” he said.
More detail needed
School Sport New Zealand chief executive Mike Summerell said he wanted to see more detail but allowing more unvaccinated children to play sport would be good.
“We welcome the news. It’s been a divisive and difficult time for sport and for schools in terms of inter-school activity but the announcement this morning means more kids are going to have access to sport where over the last few months they haven’t so that’s a real positive,” he said.
He said the change would not be enough to return big regional sports tournaments to the calendar because they involved more than 100 people.
This article is republished under a community partnership agreement with RNZ.
New Zealand will move to phase 3 of the omicron response at 11.59pm tonight, Covid-19 Response Minister Chris Hipkins has confirmed.
Director-General of Health Dr Ashley Bloomfield and Hipkins laid out what phase 3 includes.
While the ministry’s daily update of case numbers will come out later this afternoon, Hipkins confirmed today’s cases were “about 5000”. The actual figure was later confirmed as 6137 new cases and one death.
“This continued rise and also the number of hospitalisations we have which today sit at 205 means that we are now confirming our shift to phase 3 of our planned Omicron response. That’ll happen at 11.59pm tonight.”
He says most had been gearing up for this and it would not come as a surprise.
However, the move to phase three would not mean a “sudden lurch” in terms of additional restrictions or movements, because the traffic light system had been designed to smooth things out already.
“Our priorities now shift to isolating those with covid-19 and their household contacts to reduce the spread, while at the same time supporting supply chains and essential services to continue to operate.”
Only confirmed cases
Only confirmed cases and their household contacts – the people they lived with – would be required to isolate. All other contacts would be asked to monitor for symptoms but they would not have to isolate.
Hipkins said it was important to note that the legal requirement to isolate for cases and household contacts did not mean people who did not fit in those groups should not isolate.
“If you have a friend who has covid-19, you can make a judgment about whether you think you might be at risk … we are asking New Zealanders to accept a much greater degree of personal responsibility.”
Watch the announcement:
Today’s media briefing. Video: RNZ News
Dr Bloomfield said healthcare workforces who were essential and were household contacts were not allowed to go back to work for the first seven days but may return to work after that — three days early — if they returned a negative RAT on days five and six and were asymptomatic.
Hipkins said detailed information would be sent to schools but the principle remained the same — if you are not a household contact you are not required to isolate.
He said he acknowledged some parents were in a better situation than others.
Dr Bloomfield said people who did not respond to the text message would be followed up to confirm whether or not they needed clinical or social support to isolate.
RATs primary testing
Rapid antigen tests (RATs) will become the primary means of testing for covid-19, and will be available from thousands of sites. Millions more are expected to arrive over the coming days.
It is expected that businesses would be able to make the tests available to the public through retail outlets from March, he said.
Hipkins said RAT tests had been distributed throughout the health network.
“They’re available to people who need them … through the testing network,” he said.
“The last thing we want is people sitting on big stockpiles of them when there’s more demand elsewhere.”
Businesses have been able to import RATs since the beginning of December, but many “like ourselves, have had challenges in securing supplies because of global constraints”, Dr Bloomfield said.
He said clinics in Tāmaki Makaurau would begin rolling out supervised rapid antigen testing from today.
Testing locations
Locations where people can get a rapid antigen tests would be listed on the Healthpoint website.
He said there were 6.3 million unused tests in the country yesterday, another million arrived last night and another 10 million were expected to arrive in the coming week.
Hipkins said that because only household contacts were required to isolate, a self-assessment tool would help the government keep track of very high risk locations and the overall spread of the virus.
This included things like hospitals and aged care facilities.
Hospitalisations had become a major focus and daily case numbers would be a less important metric from now, Hipkins said.
“There’s no doubt the next few weeks are going to be pretty challenging… We just need to stick to the plan that we’ve set out as we manage a higher number of cases in our coming weeks before we reach a peak as other countries have,” he said.
Dr Bloomfield said hospitalisation rates were about 85 percent at the moment, which was “about what they usually are”, but an increase in cases would drive an increase.
Isolation plans needed
That said, “if you are unwell for any reason, you can and should seek care in our health system and that includes in our hospitals”.
Hipkins said omicron’s lower likelihood of severe illness, and high vaccination rates, were what allowed the self-management approach.
He suggested people should have an isolation plan, and talk to friends and whānau about how they would manage if they needed to isolate.
He also urged people to take up booster shots.
“You are far less likely to end up in hospital if you get covid-19 [and] if you’ve had a booster.”
He said modelling of the low-transmission scenario assumes high booster uptake.
Dr Bloomfield said two new studies confirmed the vaccine protected against getting infected in the first place and protected against severe illness.
“One of the studies, which was published in the Journal of the American Medical Association, showed that compared with being unvaccinated the odds of contracting omicron after receiving three doses dropped by 67 percent — two thirds — and for delta the risk declined by a stunning 93 percent.”
“So a highly-boosted population here will serve us all well.”
This article is republished under a community partnership agreement with RNZ.
The two-week old protest at New Zealand’s Parliament has been added to the Ministry of Health’s covid-19 locations of interest website as new omicron cases soar in the country.
At least two positive covid-19 test results have been reported among the anti-mandate protesters in Wellington.
The protest site is listed as a close contact event on Saturday, February 20, from 11.55am to 11pm and Sunday, February 21, from 11am to 11.59pm.
However, it would not say if the cases were among those who had been arrested in the past few days.
Police Commissioner Andrew Coster said earlier a team of staff working at the protest had caught covid-19 and while it had not been linked to protesters, it “stands to reason” the coronavirus is there.
He told Morning Report even if the virus had not been at the protest “it will be soon”.
If the Wellington protest camp is now a Covid LOI then everyone not leaving to isolate is breaking the law, right? Those people *choosing* to keep children in that environment will face some sort of legal consequences hopefully.
Protest area ‘unsafe for families’
Assistant Commissioner Richard Chambers said today: “Movements to shrink the protest footprint will continue in the coming days as our focus remains on returning the city back to normal as quickly as possible.”
He added: “The protest area is not safe for families, and it is still far from being operated lawfully.
“We will not hesitate to take enforcement action against any unlawful activity that is reported to us.
“This has been a difficult and disruptive time for many local residents and businesses.”
He said there would be a high police presence throughout the city this weekend.
“Police encourage everyone to enjoy Wellington for the right reasons this weekend.”
This article is republished under a community partnership agreement with RNZ.
Each day 40,000 New Zealander’s on average quietly make their way to vaccination centres to do their bit. There are currently only 150-300 people in attendance at the Wellington protests. Don’t be fooled by a loud minority…. We are not a nation divided.
Reporters Without Borders (RSF) has condemned the threats and violence against news media by protesters during the 16-day anti-covid-19 vaccine mandates occupation of Parliament grounds, and called for prosecutions of those responsible.
The media are among favourite targets of some of the 500 or so protesters still camped in front of the Parliament building, known as the Beehive, after arriving from various parts of the country in “freedom convoys” akin to those causing chaos in parts of Canada for the past month, reports the Paris-based media freedom watchdog in a statement tonight.
The violence against journalists trying to cover the protest had included being regularly pelted with tennis balls with such not-very-subtle insults as “terrorists” and “paedophiles” written on them, said RSF.
“Media = Fake News” and “Media is the virus” are typical of the slogans on the countless signs outside protesters’ tents.
Journalists who approach have also been greeted with drawings of gallows and nooses, as well as insults and threats of violence – to the point that most of them now have bodyguards, says Mark Stevens, head of news at Stuff, New Zealand’s leading news website.
“They’ve had gear smashed, been punched and belted with umbrellas,” he wrote. “Many reporters have been harassed […], including one threatened with their home being burned down.”
The violence has not been limited to Wellington.
In New Plymouth, an angry crowd tried to storm the offices of the local newspaper, Stuff’s Taranaki Daily News, two weeks ago, as reported by Mediawatch. Some of the protesters even managed to breach the newspaper’s secured doors and attack members of the staff.
“After the police intervened, [conspiracy theorist] Brett Power urged the protesters to return in order to hold the editor ‘accountable for crimes’ — meaning the newspaper’s failure to report their protests in the way they wanted,” the RSF statement said.
“The verbal and physical violence against journalists is accompanied by extremely shocking online hate messages.”
Stuff’s chief political reporter Henry Cooke tweeted an example of the threats he had received on social media:
i prefer the old “sleep with one eye open” thing personally, one has to get SOME sleep pic.twitter.com/wxh5x83Dsx
Daniel Bastard, the head of RSF’s Asia-Pacific desk, said: “The virulence of the threats against journalists by demonstrators, and the constant violence to which they have been subjected since the start of these protests are not acceptable in a democracy.”
He called on authorities to “not allow these disgraceful acts to go unpunished. There is a danger that journalists will no longer be able to calmly cover these protests, opening the way to a flood of misinformation.”
In a recent article, Kristin Hall, a reporter for 1News, described her dismay at discovering the level of “distaste for the press” among protesters who regarded the mainstream media as nothing more than “a bunch of liars”.
“People have asked me why I’m not covering the protests while I’m in the middle of interviewing them,” she wrote.
A Wellington Facebook page publisher attacked at the protest, as reported by 1News. Image: 1News screenshot APR
‘Headlocks, punches’ Protester mistrust is no longer limited to mainstream media regarded as accomplices of a system imposing pandemic-related restrictions, as Graham Bloxham — a Wellington resident who runs the Wellington Live Community local news page on Facebook – found to his cost when he went to interview one of the protest organisers on February 18.
“We just wanted to show people that it is peaceful … then bang. They just yelled and whacked. They were just all on me and they basically beat me and my cameraman to a pulp,” he told 1News.
“Headlocks, punches… they were really violent.”
Protesters have been asking me all week for “evidence” of volatility towards the Wellington public so here it is. https://t.co/mhJNcXlMrF
A photo of a dozen Nazi war criminals being hanged at the end of the Second World War has been circulating on social media popular with the protesters for the past few days, accompanied by the comment: “Photograph of hangings at Nuremberg, Germany. Members of the media, who lied and misled the German people, were executed.” Definitely not subtle.
Attacks against journalists have rarely or never been as virulent as this in New Zealand, which is ranked 8th out of 180 countries in RSF’s 2021 World Press Freedom Index.
Henry Cooke reported an apology from some of the protesters over the “treatment” of some journalists, but incidents have continued to be reported.
Group of protest groups apologise for denying media access to Parliament grounds – but now ask we go through a liaison officer before turning up. pic.twitter.com/MIgksDJ50O
Epidemiologist Professor Rod Jackson is urging New Zealanders to take omicron seriously, and certainly not to think of it as similar to the flu.
The warning comes as new modelling shows omicron could peak by mid next month with about 4000 daily cases.
Professor Jackson, professor of epidemiology at Auckland University, told RNZ Morning Report there was “no doubt” New Zealanders were not taking omicron seriously.
“The standard thing I hear these days is, ‘Oh, this is just a mild condition, it’s like a mild flu’ — and it’s just not true,” he said.
“In the [United] States, for example, more people have died from omicron, than died from delta. It’s also worth noting that I mean if you ever had a bad flu, you feel like you want to die.
“It’s not a particularly good comparison. The flu kills 500 people a year. Normally that’s almost double the road crash death rate. It’s about the same as suicide, just a bit less.
“This is a serious disease that people need to take seriously.”
High omicron death rate
The high omicron death rate in the US was because the variant was so contagious, Dr Jackson said.
“It spreads like wildfire, and I guess that’s the other important issue when we’re thinking about the comparison between the flu and and Omicron is that the R value, the number of people that one infected person with the flu is going to infect, is less than two.
“With omicron, we don’t even know how big it is. It’s certainly much bigger than delta, which was about six (people infected per person), so this is a very different disease from the flu and we need to take it seriously.
“We need to go out and get maximally vaccinated.”
On that point, Dr Jackson said there were a likely a lot of reasons more people had not got a booster shot.
“One is, we’re all a little over it, aren’t we? Everyone is tired. Everyone wants to go back to normal.
“Secondly there is this general view is that I hear — ‘Oh, but isn’t omicron, you know, just like a cold?’
‘People die of this’
“For some people, it’s very mild. For some people it’s asymptomatic, but people die of this.
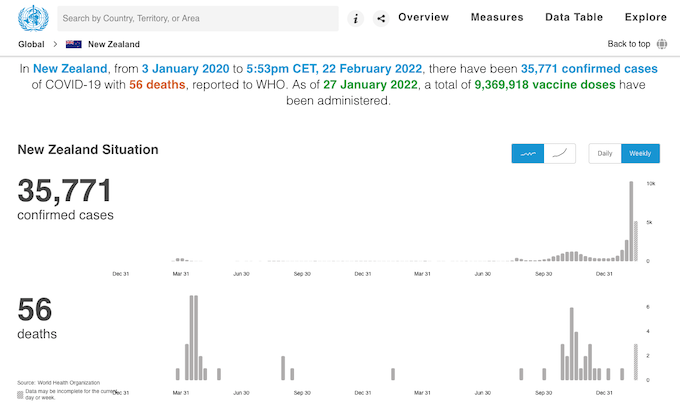
“Look at the hospital rates. Every New Zealander should have a look at the graph of the number of hospitalisations, and if you look at it in the last week or two, it’s going almost vertically.
New Zealand and covid-19 progress as at today. Graph: WHO
“There’s a couple of things we really need to do – get maximally vaccinated and wear a good mask.”
He said while they could not link transmission to the protest, with people coming far and wide for the demonstration, he would be surprised if there was no covid among protesters.
This article is republished under a community partnership agreement with RNZ.
The early morning action on Monday to cordon off the occupation of Parliament grounds and prevent it growing might go some way to restoring public confidence in the police, which has appeared to be eroding since the protests began a fortnight ago.
So far, police have pursued a de-escalation strategy, but there have been calls for firmer action.
The whole event has raised important questions about the relationship between the police and government, and about police independence and accountability.
With local businesses unable to trade, and the neighbouring university closing its campus for eight weeks, the political consequences are potentially serious.
From the government’s perspective, there is a direct relationship between its own public support and public confidence in the police. The political and legal impasse between the rightful independence of the police and public accountability is not a simple issue to resolve.
Constabulary independence The relationship between the government and the police has come a long way since government minister John Bryce — armed and on horseback — led the police invasion of Parihaka in 1881. Bryce decided who would be arrested and personally ordered the destruction of property.
Supporting the political objectives of the government of the day was a function of the police. But New Zealand was not a developed liberal democracy 140 years ago.
The Wellington protest is testing police independence and public tolerance – are there lessons from Canada’s crackdown?
By 2018, that relationship had evolved enough for the solicitor-general to advise the prime minister that “constabulary independence [had become] a core constitutional principle in New Zealand”.
As Police Commissioner Andrew Coster faces calls to resign over his handling of the protests, he says using force could come at a significant cost. https://t.co/CcHepTMRZN
The solicitor-general explained the constitutional subtleties of the Policing Act thus:
The Police are an instrument of the Crown […] but in the two principal roles of detecting and preventing crime and keeping the Queen’s peace they act independently of the Crown and serve only the law.
This is reinforced in the oath police officers swear to perform their duties “without favour or affection, malice or ill-will”.
Who is accountable? Constabulary independence means governments can’t control the police for political advantage. At the same time, police accountability to the public is as important as for any department of state.
Independence should not mean the police can do whatever they like.
However, the lines of accountability are complex. Constabulary independence means the ordinary process of accountability to Parliament through the relevant minister, and through Parliament to the people, does not fully apply to the police.
The police commissioner is accountable to the minister for “carrying out the functions and duties of the Police”, but explicitly not for “the enforcement of the law” and “the investigation and prosecution of offences”.
As well as “keeping the peace”, “maintaining public safety”, “law enforcement”, “crime prevention” and “national security”, the Policing Act requires “community support and reassurance”.
This might help explain why, for security and tactical reasons, the police won’t fully explain their tolerance of the occupation, beyond the police commissioner saying the public would not accept the inevitable violence and injury a harder line would entail.
Despite clear public concern, the police are not required to give further explanation of why they haven’t prosecuted people for intimidation and harassment, for threatening MPs, public servants and journalists, or for failing to remove illegally parked vehicles.
Canadian comparisons The situation in Canada may be instructive. There, the police have seemingly abandoned a de-escalation strategy that had lasted three weeks, with the protest in Ottawa cleared in the last few days.
As in New Zealand, public tolerance was low. Rejecting a claim that the repeated sounding of 105-decibel truck horns was “part of the democratic process”, a Canadian judge said: “Tooting a horn is not an expression of any great thought.”
In both countries, the protests are being viewed less as expressions of political thought than as simple acts of public nuisance. The difference lies in the Canadian federal government invoking special powers under its Emergencies Act.
The first time it has been invoked since it was passed in 1988, the law allows the government to use “special temporary measures that may not be appropriate in normal times” to respond to “threats to the security of Canada”.
Banks can freeze accounts being used to support the protest. Private citizens and businesses may be compelled to provide essential services to assist the state — tow trucks, for example.
Canadian journalist @mariekewalsh says the “softer approach” being used by NZ police against Parliament protesters didn’t work in Ottawa with the trucker protest. #NZQandA#nzpolhttps://t.co/9ZHyxqOJqI…
Political calculation Such significant constraints on freedom can be justified only if they are proportionate to the emergency. But on Friday, the Canadian Parliament was prevented from scrutinising the decision to declare an emergency because protesters had prevented access to the debating chambers.
Ironically, the debate began on Saturday when police cleared the obstruction (without needing emergency powers) — suggesting “freedom” is a wider concept than the one protesters claimed they were defending.
The ability of people to go to work, to study, shop, drive on a public road — and (as in Ottawa) the ability of Parliament to function — are democratic freedoms the protesters are curtailing.
Whether Wellington goes the way of Ottawa remains to be seen, but the New Zealand police commissioner says a state of emergency is among the “reasonable options” being considered to stop more protesters entering Parliament grounds.
For now, the political question is what happens if the evolution from protest to public nuisance to crisis of confidence in the police continues.
Given the constraints of constabulary independence, and the democratic need for accountability, what political responses are available to the government to ensure any crisis of confidence in the police does not become a crisis of confidence in the government itself?
For both police and government, there is much at stake in the de-escalation strategy.
We remember the life and legacy of Dr. Paul Farmer, a public health icon who spent decades building community health networks helping millions of poor people in Haiti, Rwanda, Sierra Leone and beyond. He died unexpectedly Monday at the age of 62. We feature Farmer’s past interviews with Democracy Now! and speak with his longtime colleague, Dr. Joia Mukherjee. Farmer leaves behind a remarkable legacy and an “enormous community of people that he brought to this large table that is now global health,” says Mukherjee, chief medical officer for Partners In Health, where she worked with Farmer for 23 years.
But protesters in the camp insist their stand remains peaceful, reiterating they will be going nowhere until covid-19 vaccine mandates are dropped.
Despite the claim the protest is “peaceful”, Wellington Free Ambulance announced it has made the “difficult decision” to no longer enter the protest area at Parliament.
It said the decision was made to prioritise the safety of paramedics, after the white Honda drove at police.
“The behaviour of a certain group within the protests community is absolutely disgraceful,” said Police Assistant Commissioner Richard Chambers.
Faeces thrown at police
In a repeat of Monday’s conflict, officers had faeces thrown at them. The stinging substance that was thrown at police has not been identified.
“We are working very, very hard to reduce the impact of the protest on the community here in Wellington, and to be met with the resistance we saw this morning is very disappointing for everybody,” Chambers said.
However, many still camped at Parliament on the 15th day of the protest are insisting they come in peace.
“This is a lovely community,” one woman told Checkpoint. “I’ve heard children say ‘I want to live here’.”
Flax hats at a gazebo
Leslie was weaving flax hats at a gazebo on the outskirts of the occupation. She said she felt the pull to go to Wellington after watching the protest on TV and after losing her job of seven years as a cook.
“I didn’t only lose my job, I lost my house… the house was part of my job.”
Another protester, Jacob, said the mandates meant he could not keep his job, and he was facing losing his house.
“I’ve been a caregiver working with men living with disabilities. And now since mandates, I haven’t been able to work with these clients, even though it’s one on one and they would actually want to have that continuity.”
Aucklander Bryan told Checkpoint he had been at the protest since day one and had been at the front of the line with his son in clashes with police, which he described as “amazing”.
Year 10 student Libby was also at the protest, off school and with her family.
“My brother can’t play sports. I can’t play sports. All my friends — one of my friends, she’s a really good football player and she’s been denied, she can’t play in her club teams and she’s like, really good, like she could go nationals, worldwide if she wanted to.”
The fact is that the government has not mandated that children must be vaccinated to participate in school or extracurricular activities. They are decisions made independently by schools and clubs.
Underbelly of undesirable, illegal, activity
While the atmosphere appears friendly on the ground at the protest, police say they are seeing something quite different.
Assistant Commissioner Chambers said there was an underbelly of undesirable, illegal, activity.
“There has been a suggestion that within the protest area down there, there may be sexual assaults.
“We are the only agency who can investigate sexual assaults and if anyone would like to come forward to us to talk about what might have occurred to them then please do come forward and we will work with you as best we can.”
Some protesters agree there are small, negative elements that need cleaning up, while others say the protest message must be refined.
“We need to be able to put our egos aside and be able to put our agendas aside and come together,” one protester told Checkpoint.
Mayor in high level talks
Wellington Mayor Andy Foster told Checkpoint he was in high level talks regarding the Parliament protest but would not detail who he was talking to.
Foster said he was also talking with government and police regularly.
“We are looking to achieve the same thing which is trying to get as quick as possible, as safe as possible, resolution of this protest so that we can get our streets back and people can go about doing their normal daily business.”
He said police had made “good progress” today with containing the spread of the protest, but things at the protest were not in an “acceptable position” yet.
On people losing their jobs because of the mandate, Foster said “there had to be a way through this”.
“I think the government has been fairly clear that it won’t remove mandates at this stage, but I think at least if there can be a clear pathway that might be enough for some people.
“And maybe the kind of thing you might want to think about is if … people are on sick leave, that kind of thing, just allow that to be extended so that the job is not actually lost.”
Foster said Wellington City Council was putting together a pandemic response package for local businesses, including rates deferral, reduced parking costs, and reducing council fees and charges for businesses particularly in hospitality.
Mixed messages aside, one thing that appeared consistent among the masses — with a pre-school, a vegetable garden and even a tattoo parlour — they are in it for the long haul.
This article is republished under a community partnership agreement with RNZ.
The Fiji government has warned that unvaccinated people in the vaccine-eligible population are 17 times more likely to die if they contract covid-19 than those that are vaccinated.
Health Secretary Dr James Fong said this strongly indicated that many of the unvaccinated deaths were preventable.
He is urging Fijians to get vaccinated against covid-19, including the booster shot, amid a third wave which began last November.
“I strongly urge anyone who hasn’t been vaccinated to get vaccinated now because covid-19 is here to stay, and omicron will not be the last variant,” Dr Fong said.
“And if you are vaccinated, but know someone who isn’t, please also encourage them to protect themselves by getting vaccinated.”
The vaccine rollout for children aged 12 to 17 is also underway, with 43,241 of them already having had both doses.
Meanwhile, Fijians who are unvaccinated against covid-19 are still being refused entry to a number of public spaces.
Health Minister Dr Ifereimi Waqainabete said this included houses of worship, sporting venues and high-risk businesses.
“Those who are in charge of these venues, businesses and houses of worship must ensure that they check the vaccine status of all those who enter their premises,” Dr Waqainabete said.
As of 18 February 2022, 93.1 percent of Fiji’s adult population of 844,000 were fully vaccinated against covid-19.
More than 800 deaths attributable to covid-19 have been recorded in Fiji.
This article is republished under a community partnership agreement with RNZ.
One of the people funding New Zealand’s two-week-old Parliament grounds occupation says it makes no sense to maintain a quarantine system at the border now that covid-19 cases are rife in the community.
Red Stag, which has business interests in forestry, timber, property development, and tourism, is helping to fund the protesters’ efforts.
Early today one person was arrested at the Parliament grounds protest after attempting to drive a car into a group of police officers. Two others were also arrested for obstruction as police described the protesters antics as “disgraceful”.
Police, some with shields, have been moving the concrete barriers to reduce the protesters’ ground around Parliament.
At least three officers needed medical attention after being sprayed with an unknown substance by protesters as they resisted the police actions.
‘Not happy with antics’
Verry told RNZ Morning Report he did not support the protesters sending death threats to politicians and government workers.
“Of course I’m not happy with some of the antics – nobody is.”
However, at the same time the government had “restricted the movement and the ability for thousands of businesses to do business for the last few years”.
Verry would not say how much money he had donated to the protesters or how long he had been giving them money.
“For me the protest is a way to get the government to listen and to make changes earlier than it otherwise would,” he said.
“So for me the major axe to grind I’ve got is with regards to what I’m seeing as to whether there is any justification now to maintain a quarantine system at the border for international tourism.”
He said it had previously been an $18 billion earner for the country.
Supports protest to help economy
He supported protest if it could help resurrect a vital part of the economy, especially when rapid antigen tests could be used so readily to detect the virus among international travellers.
By his calculations one positive case would have got through the border using rapid antigen tests on Friday — the same day the country had 1929 community cases.
“So what’s one extra person coming in across the border to constrain an $18 billion sector…
“There is no justification for keeping the borders closed because we’ve got one extra person with a cold.”
Verry was contributing a sum of money that he said was “not a significant” amount to a website that was collecting donations to pay for the infrastructure at the Parliament grounds.
He expected his donation would pay for “food, toilets, shelter, whatever they want to put it to”.
This article is republished under a community partnership agreement with RNZ.
There is a dangerous anger on rapid boil at the protest in Wellington. It is a stew of dispossession and unrest alongside various delusional beliefs and violent threats.
Two weeks into the protest and the police have had to endure human waste and acid thrown at them; a car driven into them; threats of violence; chants of “shame on you”; accusations of police brutality; physical attacks and injuries.
Meanwhile, the illegal occupiers (who refused to move their cars to a free car park) claim peace and love as the Ministry of Health reported today a record 2846 new community cases of covid-19 with 143 people in hospital with the virus.
It was joined by “everyday people” annoyed with mandates they don’t want to live with.
Well, if these “everyday people” can lower their standards to stand shoulder to shoulder with violent extremists all I can say is, “shame on you”.
Deputy Leader of the House, Labour’s Michael Wood recently spoke of these threats at Parliament: “There is a river of violence and menace. There is a river of anti-Semitism. There is a river of Islamophobia. There is a river of threats to people who work in this place and our staff.”
Michael Wood: “There is a river of filth, there is a river of violence and menace, there is a river of antisemitism, there is a river of Islamophobia…there is a river of genuine fascism in parts of the event that we see out the front of this parliament today” pic.twitter.com/h5zJRXA5TL
Deputy Speaker Michael Wood speaking in Parliament on February 17. Video: NZ Parliament
These underlying threads of violence give the protest its bite, if not its bark. The protest in Wellington was inspired by the truckers’ convoy in Canada and the occupation of Ottawa.
Conspiracy far right media platform Counterspin in New Zealand was central in the formation and viral spread of the Aotearoa convoy,
It is also, astoundingly, a protest that is preaching aroha (love) and peace. This is at odds with the Trump-loving, QAnon inspired cesspit of violence. QAnon believes that the government is full of elite Satan-worshipping paedophiles in government, business and media.
They believe that politicians and journalists will be executed in a day of reckoning.
That is why “hang ‘em high” was chalked on the steps to Parliament in the first days of the protest. Many people at this protest want to see politicians and media people executed.
This protest also has the support of white supremacists with swastikas chalked on a statue in the early days.
This disgusting far-right, anti-establishment hatred has no place in Aotearoa. Yet here it is at a protest supported by thousands on the Parliament lawn.
I have protested at many events over the years in Aotearoa in the name of animal rights. Never would I stand alongside people who preach violence. And in all cases police behaviour toward myself and my fellow protestors has been exemplary and respectful.
The protest was ill-thought out in direction, leaderless, and doomed to failure. Their demands cannot possibly be met in a time of global pandemic that has brought the world quite literally to its knees.
And yet as the days tick by, yoga classes spring up alongside gardens. Food stalls and dancing, a concert, love and freedom grow like fairy tales.
It’s all a fairy tale. Make no mistake. This protest may preach peace, but its bones are evil.
— Lynley Tulloch
It’s all a fairy tale. Make no mistake. This protest may preach peace, but its bones are evil.
So where to go from here? There is no end in sight for this drama. The protesters are revelling.
The government can’t move them. Police can’t move them. The army can’t move them.
Ironically, as suggested by ex-Labour party president Mike Williams, it will be the covid virus itself that will bring them down. And that is one little virus that doesn’t care about threats of violence.
The only thing it will take notice of is a vaccine and a mask, and those are in short supply on Parliament grounds right now.
The virus doesn’t care if you are a child, or elderly, or immune-compromised or dangerously deluded. It doesn’t give a care in the world about your rights. It just goes and sticks its spikes right into you joyfully.
And so, Mike Williams is probably right. And therein lies the biggest irony of this whole protest.
Dr Lynley Tulloch is an educational academic and also writes on animal rights, veganism, early childhood, feminist issues, environmentalism, and sustainable development.
Prime Minister Jacinda Ardern says the omicron outbreak is likely to peak in Aotearoa New Zealand in three to six weeks.
At that point, she says, the country will move down the traffic light settings, easing off gathering limits.
“We are predicting cases will continue to double every three to four days … it’s likely then that very soon we will all know people who have covid, or we will potentially get it ourselves,” Ardern says.
She says there are three reasons that is no longer as scary a prospect as it used to be.
“Firstly, we are highly vaccinated, and that happened before omicron set in.”
Secondly she said that meant omicron would be a mild to moderate illness, and boosters made hospitalisation 10 times less likely.
Third, public health measures like masks, gathering limits and vaccine passes were helping slow down the spread to ensure everyone who needed a hospital bed can get it.
The plan is working
“So far, that plan is working. We have 46 cases per 100,000 people, compared to 367 in New South Wales and 664 in Victoria at the same point in the outbreak. Our hospitalisations too are well below Australian states at a similar time.”
Ardern said cases were likely to peak in mid- to late March, some three to six weeks away.
At that point a rapid decline, followed by cases stabilising at a lower level was likely.
Ardern said at that point the traffic light system could change, because it meant public health measures used to protect the health system could be eased off.
She said vaccine passes had been necessary as the “least bad option” but they had always been temporary.
After we come through a wave and a peak of omicron, many unvaccinated people would have been exposed to covid-19.
She says coming through the peak would allow the government to ease mandates in places where they were less likely to impact on vulnerable people.
“They will remain important in some areas though, for some time.”
Beyond omicron … the easing of covid restrictions. Video: RNZ News
Mandates to remain in some areas
Mandates were likely to remain for some areas — particularly sections of the healthcare workforce — but there would be a narrowing of where they were required, she said.
She said it was hard to set a date, but the government needed to ensure the country was “well beyond the peak” and that the pressure on the health system was manageable.
She said the reasons not to do away with the traffic light system entirely was so the country was prepared for new variants and potential future waves, and the coming of winter at the same time as flu returns.
“To summarise then, the coming weeks. Covid will increase, and rapidly. There will be disruption and pressure from omicron. We must brace through the next six weeks, but we can do so knowing the future with fewer restrictions is near because that has always been the course we have chartered,” Ardern said.
She said that as the country reached the peak and started to come down New Zealanders could all move towards a “new normal” they can all live with.
Finance Minister Grant Robertson has outlined new financial supports to help businesses impacted by the red settings.
In a statement, the Ministry of Health said there had also been two covid-19 related deaths as well as 2365 new community cases.
“Sadly, we are today reporting the death of a patient at Middlemore Hospital.”
A patient in their 70s at Auckland City Hospital also died following a diagnosis of Covid-19, the ministry said.
“Our thoughts and condolences are with both patients’ family and friends.”
There are 116 people in hospital today – one in Northland, 20 in North Shore, 34 in Middlemore, 47 in Auckland, one in Tauranga, 12 in Waikato and one in Tairāwhiti.
There is one case in ICU or HDU.
The average age of the current hospitalisations is 58.
Ardern’s message to protesters Ardern said she had a final message for those occupying the lawns of Parliament: “Everyone is over covid. No one wants to live with rules or restrictions, but had we not been willing to work together to protect one another then we would have all been worse off as individuals, including losing people we love.
“That hasn’t happened here for the most part and that is a fact worth celebrating, rather than protesting.
“We all want to go back to the way life was, and we will, I suspect sooner than you think. But when that happens it will be because easing restrictions won’t compromise the life of thousands of people — not because you demand it.
“Now is not the time to dismantle our hard work and preparation, to remove our armour just as the battle begins.”
Ardern said she still had confidence in the police commissioner and “the enormous job” he and all police did every day, including on the forecourt of Parliament right now.
Asked when protesters would be gone, she said enforcement of the law was a decision that lay with police, she said.
She said her speech today was “absolutely not” in response to the demands of the protesters.
‘Bullying’ and ‘harassment’
She said the protesters had been engaging in illegal activity that bordered on and demonstrated “bullying” and “harassment” of Wellingtonians, and she found the opposition calls for more details on lowering restrictions “quite upsetting to see they now seem to be responding and sympathising with the protesters”.
She said no one should have to put up with having human waste thrown at them, as police say happened this morning.
Police early today moved to contain the convoy protest — which has now been at Parliament for two weeks — by installing concrete barriers to prevent more vehicles from entering the area.
Ardern has maintained there will be no engagement with the protesters, and although ACT leader David Seymour spoke to some of their representatives last week, all parties have since signed a letter from the Speaker saying there would be no dialogue from politicians until disruptive and threatening behaviour was brought to an end.
This article is republished under a community partnership agreement with RNZ.
Two weeks in and New Zealand’s anti-mandates occupation of Parliament grounds remains a total stalemate with no sign protesters are going anywhere. So where to from here?
About 800 vehicles continue to clog streets around the precinct and protester numbers swelled to more than 1000 this weekend.
Music blasted from the performance stage — just some of the new infrastructure brought in during the second weekend of the occupation of Parliament.
Early this morning, police installed concrete blocks in a bid to contain the protest and free up Wellington streets. They made a handful of arrests.
But there is still no sign of a police crackdown, or of protesters leaving, and Otago University Law professor Andrew Geddis said it looked like they were trying to wait each other out.
He said it was now a battle for public approval — but there was nothing legally preventing police from breaking the occupation up.
“If that was spraying them with pepper and hitting with batons, the law would allow for that,” he said.
“The problem is, of course, that it would look terrible, and it also, it just would be terrible.
“The idea of the police batoning people even if the law allows it … it is just something that in New Zealand we haven’t really seen for years and hopefully you never have to see again.”
Police likely attempting to divide and conquer Security analyst Dr Paul Buchanan said the police should employ a divide and conquer strategy to separate and eject protesters at Parliament with violent ideologies.
He said the intelligence services should be using camera and drone imagery and facial recognition technology to identify the far-right elements and racist extremists.
“Those people have to be dealt [with] separately and I would say a little more harshly than the majority of the crowd, which are a bunch of hippies and circle dancers, wellness folk who are well intentioned — albeit in my mind misguided.”
Dr Buchanan said there were more options than total appeasement or violent crackdown.
Advocate Simon Oosterman advises non-violent social justice activists here and abroad on how to manage interactions with police.
He said the police strategy seemed to be attempting to deescalate, avoid radicalising people by being heavy-handed, and keeping a lid on bad optics.
For now, he expected towing and ticketing vehicles at the fringes while police worked to create a split between the minority of protesters who are harassing the public and police — and the rest.
Public anger, and towing resources crucial The Parliament protest is a copycat of one in Canada which brought the downtown of the capital Ottawa to a standstill for three weeks, but which has largely been cleared out with little bloodshed.
Freelance journalist Justin Ling, who has been on the ground in the city, said an increasingly furious public, massive resources from emergency powers and the bitter cold finally brought about the breakthrough.
“Maybe the most crucial part was just the fact that the federal government was able to conscript a whole bunch of tow trucks into helping out police clear the street – just a game changer,” he said.
“You’ve seen this the city clear in just 24 hours – incredibly quickly – there were fears that could have taken weeks.”
Whānau need to ask protesters to come home – health research Tairāwhiti activist and health researcher Tina Ngata said whānau need to reach out to those who have gone to Parliament and ask them to come home.
“Even if one or two does listen, and then that’s important.
“But also I think Wellingtonians need to hear that we stand in solidarity with them. And the mana whenua of Ngāti Toa Rangatira – Taranaki Whānui in particular … they need to know we stand in solidarity with them.”
Wellington iwi leaders have called for an end to the protest at Parliament.
Ngata said those who did return home need to be tested so they do not bring covid back into vulnerable communities.
Meanwhile, both Buchanan and Ngata said even if the Parliament occupation is broken up, they expect the protest to keep spreading around the country.
This article is republished under a community partnership agreement with RNZ.
COMMENTARY:Open letter by Nick Rockel to the Parliament protesters.
So the Parliament protest goes on, the first protest I can recall having absolutely no sympathy for. I’ve been on marches protesting lack of education funding, nuclear testing, abuse of GCSB [Government Communications Security Bureau] powers, the TPP [Trans-Pacific Partnership] etc.
All of which I cared about, but this protesting against health measures – yeah nah.
People have been through a lot during this covid-19 pandemic; some have lost loved ones, and some have endured serious illness. We’ve all missed events or time with family and friends by following restrictions for the greater good.
But these people? No they don’t want to comply with mandate restrictions to help others, no they don’t want to do their bit for herd immunity like the other 95 percent
Sure a small number have suffered as a direct result of mandates although unless there is a genuine medical reason you can’t be vaccinated I have no sympathy, choices have consequences.
You’re entitled to not get vaccinated, despite your placards this isn’t a fascist state. But if you want to be able to do certain jobs then get vaccinated, it isn’t hard, it is well tested, the science is out on this one.
There is a false equivalence between “no jab no job” restrictions put in place to reduce the spread of a virus with the persecution of people based on race or sexual orientation. How ridiculous.
Heavy machinery regulations comparison
A better comparison is of someone being outraged at regulations where because you work with heavy machinery you have to pass a drug test to check you’re safe to do so for the benefit of others around you.
Even that falls down, you’re not a danger to others if you turn up to work on Monday having smoked a joint on Friday evening, but if you refuse to get vaccinated to perform a role where you come in to contact with vulnerable people, for example in a retirement village or on a hospital ward, you present an additional risk to others.
It may be a small risk but it is an additional risk that you are happy to impose on others for your “freedom”.
There is also the additional, and unnecessary, cost to the health system of people not being vaccinated — the hospitalisation rate of the unvaccinated versus those with at least two doses is many many times higher. If our health system becomes overwelmed leading to the need to increase restrictions ironically it will be disproportionately down to people who want to remain unrestricted by regulations.
Some suggest we could run parallel systems for the unvaccinated so the odd nurse or teacher who doesn’t want to get vaccinated can continue working. Our public services have limited resources, they are already under pressure, to think that we should run a parallel system for the 5 percent of people who choose not to be vaccinated is absurd.
In addition to those opposed to health measures there are people at the protest for many different causes. According to their placards they oppose Jeffrey Epstein — which seems a reasonable thing to do if a little weird to include in this protest, fluoridation, 1080, Three Waters, and support Groundswell, Trump etc
Some refer to “Jewcinda”, paint swastikas on statues and carry placards of the PM as “Dictator of the year” with a toothbrush mustache, or talking about Nuremburg trials. But those are just a few bad eggs, like the ones that threw, err eggs, at a child for wearing a mask.
Not wanting others to wear masks
Apparently their desire for freedom extends to not wanting others to be allowed to wear masks.
Yes many people are there simply to oppose health measures rather than support these other causes, but the nutjob quotient, the thug element, even allowing for media sensationalism, seems incredibly high. I note the local Iwi have called for an end to the abuse and the threats at the protest.
If Philip Arps or Kyle Chapman turned up at many protests they would be made very unwelcome to say the least. Seemingly this group is quite tolerant of them, tolerant of white supremacists. Nah — you’re supposed to be intolerant of fascists. Not protest alongside them and pretend you can’t see them.
I don’t know if the other protesters are intimidated by the far right elements that are there with them, or happy that they have a common enemy in the government and content to co-exist.
What is not plausible is any claim that says they are not aware of them, of the abuse and the death threats by those around them. I call BS.
The Speaker of the house, Trevor Mallard, playing repetitive songs and covid health messages to the protesters, has outraged some people — many of us think it is rather funny.
New Zealand has seen protests where people have really endured hardship for causes, be it Ihumātao, Bastion Point, the Springbok marches. Honestly the people outside Parliament have been there in the middle of summer, had some rain, probably don’t have enough toilets, and listened to some annoying music — its not much compared to getting battoned on Molesworth Street by the Red Squad.
No return to Red Squad
I would certainly not want to see a return to the approach of the Red Squad, but the police, as they have at other protests against covid health measures, have really lost credibility with the lack of action, at least against those intimidating people. The failure to tow, or at least clamp, illegally parked vehicles has become a joke.
The mandates will eventually be gone of course; the government has already acknowledged this. When they go it will be based upon health information, one would hope, and not a relatively small group of people protesting.
Not protesting, it should be noted, when these health measures were introduced a year ago when border workers became the first workers who had to be vaccinated in order to stop more spread into Aotearoa, but when the end is likely already in sight.
Barring of course the unforeseen, the unknowable, that protesters demands would have ignored.
I’ve been on protests of 10,000 people, and boy that feels like a big protest when you’re on it. These people though look to have maybe 400-500. Let’s give them the benefit of the doubt and say there are a thousand protesters. That is still a very small number to be getting this level of media coverage, making demands the majority are opposed to, or to be claiming to speak on behalf of others.
Don’t claim to be standing up for my rights, put down the placard and stop holding the good folks of Wellington — who would like their city back — to ransom. As one old fellow interviewed on the news said: “Go home — and take a bath.”
These people do of course have the right to protest, not erect tents or park illegally mind you, but certainly to protest. I also have the right to think and say they’re a bunch of selfish idiots, a view I suspect is shared by a very large number of people.
Nick Rockel is a “Westie Leftie with five children, two dogs, and a wonderful wife”. He is the author of the Daily Read where this article was first published. It is republished here with the author’s permission.
Some residents of the area around New Zealand’s Parliament in the capital Wellington are worried about leaving their houses with protesters outside, while police say they will clamp down on any abusive behaviour.
Protesters have been occupying Parliament’s lawn and surrounding areas for close to two weeks.
In 2020’s first covid-19 outbreak, the highest number of people in hospital at one time was 89.
None of the 100 hospital cases announced today were in intensive care units. The hospital cases are mostly in Auckland, but there are also cases in Waikato, Tauranga, Rotorua and Tairāwhiti.
Number in hospital grows
The number of people in hospital has been growing steadily all week as new cases rose, and has tripled since 32 people were in hospital on February 13.
According to the Ministry of Health’s website, as of February 19 a total of 836 people had been hospitalised during the pandemic, and 69 people were in ICU care.
A Hill St resident who asked not to be named said the protest had spread further so he was now living in the middle of it.
During the occupation, he said protesters had tried to remove his housemate’s mask, and other residents had been verbally abused for wearing one, including himself.
The protest appeared to be “anti-everything covid”, not just anti-mandate, he said.
“If it was a more nuanced protest around mandates, you’d see people wearing masks. The reality is there’s nobody wearing masks there.
“It’s a complete denial of the risk of covid whatsoever, which is really concerning. I’d feel a lot more comfortable if people were wearing masks.”
The resident has been going to his work every day to avoid being around the protest and said his neighbours had also gone away.
A graffiti-covered car parked at the protest camp at Parliament. Image: Craig McCulloch/RNZ
He didn’t feel entirely safe having to walk past and through hundreds of unmasked people to get home, he said.
Policing being strengthened
In a statement tonight, New Zealand police said that they were strengthening the policing of abusive behaviour around the protest, as well as traffic management and road traffic controls.
“Regular reassurance patrols of local businesses have been increased,” police said.
“Staff have also been instructed to take a zero-tolerance approach to any abuse, intimidation or violence against members of the public.”
Police said there would be an increased presence around the start and end of each day.
“Anyone abusing or intimidating members of the public can expect to be arrested, removed and face charges,” they said.
The Wellington Hill St resident wanted protesters to wear a mask, for the streets to be cleared so people could walk freely without harassment, and for protesters to stick to the lawns of Parliament.
“I am furious about the occupation of the bus exchange, I mean it’s a parking lot campsite now.
Standstill of public infrastructure
“That doesn’t affect the politicians. It’s not going to change anyone’s view on mandates, all it creates is a complete standstill of public infrastructure in Wellington. It’s nothing but disruptive.”
While he wanted to see the streets cleared, he was concerned that he could end up in the middle of a riot if the police stepped in.
“If we see the break out of a riot — which I think if police do eventually move in is a real possibility — it will be instigated by those more extreme people, but the reality of mob rule and people who feel pissed off is that they will join in.
“And all of a sudden, we will be right in the middle of a riot.”
Residents were contacted by the protesters about a week ago to see if they’d allow a medical tent to be set up in garages or a back garden who they told to contact the public health service, he said.
“If we were having a party on the street, A – it would get shut down, and B – it wouldn’t be masking over that more like dangerous underbelly of the whole thing whereby people are still being abused.”
Police said that parked vehicles around the protest area had swelled to approximately 2000 on Saturday, with about 800 of those illegally parked. A small number of vehicles were towed.
‘Positive’ engagement
Police said engagement with protest leaders had been “positive” over the weekend.
“Security and safety” were the focus of talks, police said in their statement.
Meanwhile, a counter protest is being launched in response to the Parliament occupation.
Matthew Tukaki from the National Māori Authority said an overwhelming number of people had been in touch with him saying they had had enough.
He said the vast number of Wellingtonians were fed up with the disruption to their lives, the abuse and the desecration of the memories of servicemen and women.
Tukaki said it would be an online protest without confrontation, intimidation, abuse or threatening behaviour.
This article is republished under a community partnership agreement with RNZ.
New Zealand police have moved to start clearing up the roads near Parliament in the capital Wellington, where protesters have clogged the roads with vehicles for more than a week.
But there has also been a significant increase in illegally parked vehicles in the area.
Some streets around Parliament could not be used since people protesting against covid-19 vaccine mandates clogged the roads with their vehicles, with public transport in the capital also having to be re-routed.
On Thursday, police estimated more than 400 cars, vans and campervans were ensconced in several streets alongside Parliament and today that estimate grew to 800.
The protest, which began on February 8, drew a crowd of more than 1000 people today.
Yesterday, Police Commissioner Andrew Coster said they were expecting more people to turn up to the protest over the weekend, and that they would implement a traffic management plan.
Despite police previously warning protesters to move their vehicles or face towing, they did not end up acting on the ultimatum, fearing an escalation.
Tow trucks relocating vehicles
But on Saturday afternoon, tow trucks were seen relocating illegally parked cars near Wellington railway station.
In a statement, police said there was an increase of people attending the protest today, as was anticipated.
“Police cleared illegally parked vehicles on Thorndon Quay today — 15 were moved by protesters after police spoke with them and two were towed.
“Police are also noting the registration of vehicles currently impeding traffic for follow up enforcement action, and structures such as tents and marquees are being removed from any site that does not form part of the main protest area.”
The cars were parked in the median strip in the middle of the road, and appear to be relocated to the side of the road.
Over a dozen police cleared traffic in the area and directed pedestrians to move away, when a small crowd began to gather.
Further up the road, traffic cones with “no parking” signs have been laid down on the curb of Bowen Street, where many cars remain illegally parked.
Sky Stadium at capacity
Police said the parking facility at Sky Stadium was at capacity, after they had previously encouraged protesters to move their vehicles there.
But they said they had “serious concerns” about health and safety as a concert at the protest site has been planned.
“We continue to maintain a highly visible, reassurance presence on site, and staff are engaging with the public and protesters to provide advice and, where necessary, take enforcement action.”
Police said they have attended at least six medical events within the protest and continued to urge anyone parked unlawfully to remove their vehicle to allow emergency services access.
Meanwhile, Marlborough Mayor John Leggett said protesters in Picton had made it clear they would not be moving until their counterparts in Wellington do.
Leggett said the council had been in contact with leaders of the action in Nelson Square, who had made their position clear.
He said the Picton occupiers were linked to the Wellington anti-mandate protest.
“To put it the other way, if Wellington [protest] is resolved, we will get a resolution here, a peaceful resolution, and they’ve made it very clear that their occupation is linked entirely to what’s happening in Wellington so there needs to be some way of resolving the Wellington situation.”
Police today said they were also maintaining a presence at that protest, as well as another one in Christchurch.
The ministry said 1240 of the new cases were in Auckland, with the rest in the Northland (33), Waikato (249), Bay of Plenty (66), Lakes (11), Hawke’s Bay (22), MidCentral (12), Whanganui (10), Taranaki (10), Tairāwhiti (12), Wairarapa (17), Capital and Coast (38), Hutt Valley (31), Nelson Marlborough (40), Canterbury (40), South Canterbury (2), West Coast (1) and Southern (65) DHBs.
There were also 14 cases identified at the border, including five historical cases.
Due to one of the longest and strictest lockdowns in the world, limited in-person teaching in the Philippines only resumed in late 2021, 20 months since the start of pandemic restrictions in March 2020. More than 27 million children have been out of school. The country’s Department of Education (DepEd) was only able to allow 100 public schools to take part in its pilot run of face-to-face classes in November 2021. Only five thousand students went back to the physical classroom. However, with the current wave of COVID-19 cases due to the Omicron variant still being managed, in-person classes have been disrupted again. The Philippine national government has no choice but to continue to rely on remote learning. This has set the Philippines back in attaining UN Sustainable Development Goal (SDG) 4: Quality Education which aims to achieve inclusive and equitable quality education and to promote lifelong educational opportunities for all.
In her 24 January 2022 message for International Day of Education (IDE), UNESCO Director-General Audrey Azoulay called for a new “social contract” for education. Her message asked for past injustices be repaired and for digital inclusion and equity in response to an educational crisis exacerbated by the COVID-19 pandemic.
The Basic Educational-Learning Continuity Plan (BE-LCP) has been the DepEd’s flagship response since the beginning of the pandemic. Aiming to deliver quality education in the “new normal” setting, the BE-LCP involves the distribution of self-learning modules integrated with alternative learning modalities such as online, blended, television-based, and radio-based instructions. This programme has safeguarded not just students, but also teachers and staff, from contracting COVID-19.
Nonetheless, the national government’s earnest efforts to deliver inclusive quality education were met with challenges. We found evidence of these challenges in a series of 38 interviews with public servants, NGO workers, and community leaders in urban poor areas in Metro Manila and Bulacan. Our respondents reported on both the observable impacts of COVID-19, and the government and community responses to the pandemic. The key concerns our informants pointed out regarding basic education included: interrelated issues of accessing the internet, availability of gadgets, and proficiency in using technology; low quality instruction and supervision from guardians, most often stay-at-home mothers, due to their own limited educational attainment; and lack of physical and psychological space conducive to learning. However, the pandemic did not trigger these issues for those living in urban poor communities; it just made them worse.
To respond to these perennial challenges, DepEd Secretary Leonor Briones encouraged education experts and stakeholders to a collective effort in designing future learning spaces in her speech during the DepEd’s celebration of the IDE this year. DepEd took its cue from UNESCO’s Futures of Education project which aimed “to rethink education and shape the future”. The UNESCO initiative proposed to view education as “a new social contract” – a shared global effort to broaden the horizon of learning so that knowledge can genuinely shape humanity and the environment in an increasingly complex and fast-changing world.
In line with this call to create new opportunities, one inspiring and innovative community response to the pandemic which an interviewee reported to us stood out: a tutoring programme in an urban poor mission station in the Diocese of Caloocan. A community organiser related how their chapel initiated a program to help young children by providing free one-on-one tutorial classes handled by the community’s own scholars. This project has been running for two years. Elementary students are paired with senior high school and college students. These student-tutors guide their respective tutees during two-hour sessions twice a week, with focus on English, Maths, and Science. They also cover other subjects if there is time. This school year, the programme is catering for around 70 pupils with more than 30 volunteers.
Many Filipino students don’t have computers or internet access for online learning during COVID-19. On “subaltern social media strategies” for demanding equitable access.
As an incentive for the student-tutors, they can join another community project called “Laptop for Work”. As part of the programme, the tutors themselves have to render community service so that they can keep the laptop provided to them to guide their tutees. Thus far the mission station has provided 29 laptops for their scholars. Other tutors are still working towards ownership of their device. The tutors have the option to community service, such as helping with the liturgy or volunteering in the feeding program or community pantries. Most tutors, however, opted to conduct tutorial classes.
This simple yet ingenious example addresses all three challenges to the remote learning plan of the national government: technology access, knowledge expertise, and a conducive learning environment. The model community-tutoring programme has provided the electronic devices and Internet access that pupils need to access their online modules. They also receive personalised academic guidance from a competent student tutor, and a space conducive to study within the chapel. More importantly, this mentorship programme involves the entire community: not just the pupil-tutor pair, but also their parents, other volunteers who prepare the study area and snacks, and the generous benefactors. Thus, this program has not only been an effective solution to persistent learning issues during the pandemic but also a concrete example of how education can in fact be a “social contract”.
Schemes such as the one outlined above may go some way to addressing the inequalities in educational access that have been worsened by the pandemic. However, there is also the danger that some students may lose educational aspiration or never return to education. Because of this, education departments need to future proof their policies by paying attention to SDG 4-related Targets 4.3 (Adult Education) and 4.4 (Skills for Work). To an extent, a “second chance” to learn has been addressed by DepEd’s adult-centred Alternative Learning System (ALS), though studies show that this program has also been impacted by the pandemic. Nevertheless, educational attainment is crucial, not just for the employment prospects of the individual but also for development prospects of the country as a whole.
More practical attention also needs to be given to digital inclusion, that is, affordable and accessible internet access and the availability of devices. Many of our interviewees told us that even when school children were able to access online lessons they had to share devices with siblings. For many families, the only way to access online learning resources was by using mobile phones. Some commendable efforts have been made by local government agencies, charities, and schools to distribute devices but inevitably they were limited.
These are some practical ways to respond to the crisis in education yet there is still a lot more reimagining and actual transformational work on learning that has to be done. In a globalised world, it takes not just a village but the whole world to raise every child. Only then can we celebrate an inclusive international day of quality education.
Police have pulled back on their plans to begin towing vehicles illegally parked around the anti-vaccine, anti-mandate protest on Aotearoa New Zealand’s Parliament grounds.
In a statement, police said they now had access to significantly more tow trucks to remove illegally parked vehicles but they were concentrating on engaging with protest leaders.
Police said they were exercising “careful judgement” about when to start the towing process.
“Having observed the response from protesters and noting the ongoing dynamics of similar situations overseas, police is continuing to exercise careful judgement about when to commence a towing phase,” the statement said.
“For the time being, police is continuing to focus on engagement with protest leaders with the aim of building on the initial positive responses we have seen so far.”
Police secure tow companies
Police had pulled back from an ultimatum to tow the vehicles but said they had secured commitments from companies outside the region to help if a decision was made to start the removal.
Meanwhile, Speaker of the House Trevor Mallard said, on behalf of all parties, there would be no dialogue with protestors currently occupying the Parliamentary precinct and surrounding areas until the protest returned to “one within the law, including the clearing of all illegally parked vehicles blocking streets, the removal of unauthorised structures, and the cessation of the intimidation of Wellingtonians”.
Police monitoring the Parliament protest in Wellington today. Image: Angus Dreaver/RNZ
National Recovery Alliance — a group of seven Auckland towing companies — spokesperson Chris Ratcliffe told RNZ Morning Report that if police contacted towing companies across the country it was possible they could get up to 20 tow trucks.
He said police would need every one of those tow trucks to clear the hundreds of vehicles in a timely manner.
“Broadly speaking, a good operator in a good truck in a towaway environment might be able to tow one car every 30 minutes.
“Assuming that they are able to operate unimpeded roughly 20 trucks could probably clear 400 vehicles within a day or so, and that doesn’t really take into account the heavy vehicles.
“It depends how many people they are able to get involved.”
No job on such large scale
Ratcliffe had not experienced a job of that sort of scale before.
Prime Minister Jacinda Ardern said it was not unusual for the group to meet, as they did today.
“To give context it’s agencies coming together, so that’s happened at an agency level at the request of the New Zealand police because there are multiple agencies that are affected by the protest — the courts for instance sit opposite Parliament and have been affected.”
Anti-Covid-19 vaccine mandate protesters have erected tents, gazebos, caravans and portaloos in the central park since Monday, but the square has been a regular meeting place of Destiny Church and the Freedom and Rights Coalition for months.
Despite residents’ efforts to notify the council of their concerns, Christchurch City Council and police said they were only monitoring the situation as of yet.
Due to safety concerns, the council said it would only send staff to the square if they were accompanied by a police presence.
A resident said a neighbour had rung them crying, distraught over the lack of local authority action.
Another resident believed the law had failed them.
They said they had talked to the council about the protesters in the past, without any success.
“The council said it has not been able to send staff to the park because they were concerned for their safety and said they would only attend with police protection.
“But the police are only monitoring the situation, so nothing happens.”
Picton protesters refuse to vacate park Today, a group of protesters entrenched in Picton’s Nelson Square Reserve — numbering in the hundreds — continued to camp out in the park, despite the Marlborough District Council’s request to vacate the area by 5pm yesterday.
“We have attempted a conciliatory approach, the occupiers have backtracked on that agreement. We have to move to a stage of serving trespass notices,” Leggett told Morning Report.
“The enforcement part of the process will rest with the police. We’ve been working very closely with them, they are aware of our position.”
Police said they would continue to monitor the situation.
This article is republished under a community partnership agreement with RNZ.
A group of church ministers in Fiji have resigned because they do not want to be vaccinated against covid-19.
There has been growing pressure on the clergy to get the injections since the Fiji government’s “No jab, no job” policy for public servants was announced last June.
The Methodist Church said this week 11 of its pastors had tendered their resignations.
The church’s secretary, Reverend Wilfred Regunamada, said the ministers were not forced to resign but had done so of their own free will.
“And in between that deadline, the church continued to call and ask them if they had changed their decision,” he said.
“Those who have not changed and made their decision, the church in the various circuits or the divisions that they were in, farewelled them very well. ”
Reverend Regunamada said the church respected their decision and the vacant positions would be filled by other lay preachers and theology students within the church.
Methodist Church the largest
The Methodist Church is the largest Christian denomination in Fiji, with 36.2 percent of the total population (300,000) including 66.6 percent of indigenous Fijians.
In October last year, 10 ministers of the Christian Mission Fellowship Church quit over their refusal to be vaccinated.
At the time, Reverend Regunamada, then the Methodist Church’s secretary for communications and overseas mission, said they had not laid off any of their ministers nor had anyone been forced to resign.
“Currently, we are carrying out awareness for our ministers and they are being given time, until November, to get their vaccines.
“The church’s stand is mainly to ensure the safety of its members which means that its ministers, who are servants of the people, need to be vaccinated first.
“At the moment, those that have not been vaccinated have been requested not to partake in any church services but have been advised to stay in their own homes and they are still being paid,” Reverend Regunamada said.
Reverend Wilfred Regunamada … Photo: Supplied
Remaining 8 percent tough to vax, says ministry
Meanwhile, Fiji’s Health Ministry is finding it hard to vaccinate the remaining eight percent of the adult population against covid-19.
Health Secretary Dr James Fong said they continued to receive requests for vaccine exemption from people with medical comorbidities, particularly non communicable diseases (NCDs).
He said the medical condition of these people required vaccination “and granting the exemption is not an option for any qualified medical person”.
“We have noted how difficult it is to increase our vaccination coverage for the last 8 percent of our adult population, despite the increased risk of severe outcomes in this group,” Dr Fong said.
He said community support was needed to sustain the impact of their efforts.
“While we will continue to do our part to promote and deploy vaccines, we need community support to sustain the impact of our efforts especially to the vulnerable within this 10 percent.
“It is a grave concern that we continue to receive requests for vaccine exemption from persons with medical comorbidities, especially NCDs.”
Booster dose programme
As of February 14, 574,700 of Fiji’s adult population had been fully vaccinated, the Health Ministry stated.
The booster dose programme began at the end of November 2021. As of February 14, 91,414 individuals had received booster doses of the Moderna vaccine and 60 people got the Pfizer dose.
Dr Fong said for the month of February, 175,558 more people had become eligible for booster doses.
“We are targeting to cover all these eligible individuals in the days ahead. Please come forward to get your booster (third dose) vaccine if you are aged 18 or over and it has been at least 5 months since your second dose.”
Fiji has 141 active cases of covid-19 in isolation while the death toll is at 820.
This article is republished under a community partnership agreement with RNZ.
Sir David, who is chair of the Strategic Covid-19 Public Health Advisory Group, said Aotearoa is much more ready than any other country he can think of to face an omicron outbreak on a large scale.
The experience of other countries has shown New Zealand that the country cannot beat omicron in the way it beat the original virus and to a large extent Delta, he said.
“I see this as a strategic withdrawal. It has been carefully planned. It shows that omicron is now getting the upper hand.”
He praised public health officials for their “Rolls-Royce” contact tracing but said there was now no choice except to move to phase two.
However, his greatest concern is the numbers who are still to get their booster shot, he told RNZ Morning Report.
Two doses ‘not adequate’
“I’m amazed that there’s more than a million New Zealanders who are eligible for the booster dose who have not yet taken up that opportunity. This is crazy.
“I think it’s time we stopped talking about people being fully vaccinated if they’ve only had two doses.”
The virus had mutated, Sir David said, and omicron was better at evading the vaccine immunity.
“So two doses of the vaccine doesn’t give adequate protection.”
He urged all those eligible to make an appointment or get it done today.
“No point having it in a few weeks after you’ve become sick.”
He referred to Denmark which has a similar population to New Zealand and is sometimes held up as a covid-19 success story.
He pointed out that it had seen 4000 deaths and was still having around 27 people die daily whereas Aotearoa’s total death toll in two years was 53.
Challenges face the country
“The next few months are going to be very challenging for this country. We are going to experience something of what those other countries had, so I think we all need to fasten our seat belts.
“It’s not just health although many of us will become sick and a considerable number will die. It’s also going to affect business, it’s going to affect social life and it’s going to affect education. The best thing people we can do right now is get boosted.”
He said people were tired of the pandemic but now was not the time to be considering removing restrictions.
While there was some fragmentation on the best way to deal with covid-19, there was also a consensus that New Zealanders did not want to see large numbers of people get seriously ill or die.
He said as an older person he would be doing his best to avoid getting the virus. He would be restricting his contact with other people while trying to live as normal a life as possible.
While there is some fragmentation on the best way to deal with covid-19, there is also a consensus that New Zealanders do not want to see large numbers of people get seriously ill or die. Image: Nate McKinnon/RNZ
Pragmatic managing of omicron
Te Pūnaha Matatini principal investigator Dr Dion O’Neale says phase two is a pragmatic way to manage the growing omicron outbreak.
He told Morning Report that the high numbers of the last couple of days were pulling the country back in line with what the modelling had been predicting for a while.
“So we’ve seen overseas and we’d expect to see in New Zealand doubling times every three days. So that’s your trend.
“On top of that there will be little ups and downs … from here they go up.”
Dr O’Neal said the country had been able to slow down the spread of omicron, due mainly to the work of contact tracers. Their efforts had “put the brakes on” a growth of cases.
However, once case numbers got high there was not enough capacity to contact trace for every case and the spread would speed up, leading to the inevitable decision to move to phase two.
New system more online focused
“It’s an acknowledgement that with these high case numbers systems and processes they won’t have the capacity to deal with the large numbers and we need to try and change how we respond to covid.”
Until now, the contact tracing system has been very personal with contact names identified and these people are then rung and given advice.
The new system will be more online focused, with a text message with a positive result sent, and then the person will be asked to fill in an online form and the information is passed on.
O’Neal said it would be important for people to pass on information on possible exposures as quickly as possible, not waiting for official processes which might be slower as systems became stretched.
Despite being trespassed from Parliament grounds a week ago, protesters remain on the Parliament lawn and show no sign of leaving in spite of a new record 981 community covid-19 cases yesterday.
This article is republished under a community partnership agreement with RNZ.
Where there wasn’t one before, a brand new White House Environmental Justice Advisory Council is up and running, with 26 members advising the administration on centering equity as it tackles disaster response, climate change and the energy transition. A handful of federal programs are at work channeling 40 percent of the benefits of federal investments to “disadvantaged communities,” though officials have yet to define just what that means. Environmental justice groups are demanding more action still, such as rapid progress on the now-overdue revamp of a climate and environmental justice mapping application, which will help ensure that this investment maximizes equity and social progress by identifying frontline and fenceline communities that have borne the brunt of pollution and climate risks.
But one existing environmental justice tool, which officials have let lie largely dormant across administrations, has particular potential to bring some form of justice to communities that have experienced environmental racism for generations.
Title VI of the Civil Rights Act of 1964 prevents any program that receives federal funding from discriminating on the basis of “race, color or national origin,” whether by denying benefits to or excluding certain groups from participation in public process. As the Department of Justice has emblazoned on its website, ahead of the passage of the landmark statute, President John F. Kennedy noted: “Simple justice requires that public funds, to which all taxpayers of all races … contribute, not be spent in any fashion which encourages, entrenches, subsidizes or results in racial … discrimination.”
The law empowers communities alleging they’ve been discriminated against by a group receiving federal funding — with environmental cases, typically state or local regulators that issue permits to industrial developers — to file complaints with whichever agency has provided the funds, or to bring a lawsuit in federal court against that entity. It also instructs federal agencies delivering funds, such as the Environmental Protection Agency (EPA), to stop funding programs found to have acted discriminatorily, or to refer the matter to the Department of Justice.
Nearly six decades later, whole bodies of research reveal that government agencies, often through inaction, have contributed to the formation of “sacrifice zones” — communities where residents die of illnesses more often and earlier than others due to the superfluous siting of polluting operations nearby. In 2021, for instance, ProPublica published the most detailed map to date revealing that census tracts where the majority of residents are people of color are exposed to 40 percent more cancer-causing air pollutants when compared with census tracts that are mostly white.
“Industries rely on having these sinks — these sacrifice zones — for polluting. That political calculus has kept in place a regulatory system that allows for the continued concentration of industry,” Ana Baptista, an environmental policy professor at The New School, told ProPublica, in reference to the organization’s investigation. “We sacrifice these low-income, African American, Indigenous communities for the economic benefit of the region or state or country.”
As numerous legal scholars told Truthout, Title VI provides remedy that could begin to address this flagrant legacy by steering agencies toward serving the communities they’re charged with protecting with equal rigor.
“It’s a very powerful tool — at least on paper — for addressing environmental justice issues,” Oren Sellstrom, the litigation director for Lawyers for Civil Rights told Truthout.
It’s also a tool that’s profoundly needed, but has yet to be fully embraced, advocates say. In addition to data made available by scholarly and journalistic efforts, the federal government’s own maps reveal enormous health and pollution disparities. But in spite of this documentation, and having received hundreds of complaints alleging discrimination, the EPA’s External Civil Rights Compliance Office (ECRCO) has only four times ever in its history issued a formal finding of discrimination.
The first case sat for nearly 25 years until in 2017, ECRCO determined a “finding of discriminatory treatment of African Americans” by Michigan’s leading environmental agency in considering and approving a 1994 permit for a wood-burning incinerator and power plant located in Flint, known as the Genesee Power Station. The findings included that the agency gave special accommodations to a white doctor wanting to testify early, but denied accommodations to two Black residents seeking the same option; and that the agency used armed guards — which it hadn’t done at hearings held further away in predominantly white areas — to intimidate Black residents. The siting of the facility was also noted.
“This area is predominantly black, low-income, with a disproportionate number of female-headed households,” C.S. Mott Community College professor Janice O’Neal said in 1995, according to reporting by the Detroit Free Press. “These people are at greater risk for all kinds of environmental exposures already. This ought to be taken into consideration in the siting process. If it’s not, the process is racist.”
As the complaint — originally filed in 1992 — collected dust, babies grew into adults and had their own children, all while the incinerator was allowed to pump pollutants like lead into the atmosphere and the lungs of its primarily Black neighbors. The Flint water crisis was allowed to occur. In 2015, an official from the same Michigan agency later found to have violated the Civil Rights Act said that anyone worried about Flint’s drinking water should “relax.”
Although it did find noncompliance with Title VI in 2017, EPA officials did not call on what Sellstrom refers to as its “ultimate lever”: the authority to pull funding from a group found to be discriminating. Nor have they ever.
One barrier is that U.S. Supreme Court decisions have found that Title VI requires evidence of “intentional discrimination,” which is logistically difficult, according to Albert Huang of the American Bar Association.
Yet the more troubling truth is that officials have chosen to prioritize certain laws, such as the Endangered Species Act, over Title VI. “The [EPA] has over decades internalized the idea that the Civil Rights Act is not worth enforcing,” Patrice Simms, vice president of litigation for healthy communities with Earthjustice and visiting professor of law at Harvard University, told Truthout. Simms points out that if other agencies were found not to be enforcing the laws they are specifically charged with overseeing, “it would be absolutely unacceptable.” Simms has himself worked for the EPA and the Department of Justice in a variety of posts.
Of 209 complaints alleging discrimination filed since 2014, 133 were rejected. Dozens of other complaints remained on a backlog for years, according to a September 2020 report by the Office of the Inspector General.
ECRCO’s ability to do its job is severely limited by a lack of resources, says Andrew Bashi, an attorney with the Great Lakes Environmental Law Center. ECRCO has a mere 12 staff members tackling complaints. By comparison, the equivalent office at the Department of Education has 500 people dedicated to enforcing the Civil Rights Act.
“The simultaneous unwillingness to fund the efforts of an office like ECRCO, work that could be so central to addressing some of the structural inequities impacting the very communities our system continues to imprison disproportionately, exposes the great paradox of America’s racial progress,” Bashi said.
The Title VI complaints alleging discrimination — 90 percent of which, up until 2013, were rejected or dismissed — are expansive: predominantly Latinx residents who say the state failed to protect their groundwater source when issuing a discharge permit to a facility in Eunice, New Mexico; a Black neighborhood in Beaumont, Texas, that was exposed to chemicals spewing from an ExxonMobil “sour crude” refinery for 17 years until the EPA settled its Title VI complaint, during which time the company dumped over 400 million pounds of pollution into the air; a rural community in Orange County, North Carolina, that waited over a decade after filing a Title VI complaint for the county to extend sewer and water services.
“I don’t feel anybody should fight as long as we’ve been fighting to get something that’s God-given,” Orange County resident David Caldwell Jr. told The New Yorker of his neighborhood’s sustained effort to get water and sewer services akin to others in the county.
Taylor Gillespie, strategic communications coordinator for the EPA, said over email that ECRCO’s consistent underfunding has limited the office to operating on a reactive rather than a proactive basis in response to allegations of discrimination. But the tides are turning within the agency, she noted, describing EPA Administrator Michael Regan as “committed to using EPA’s full authority under the federal civil rights laws.” In January, the EPA introduced an annual compliance review process to ensure recipients of its funding are not in violation of the Civil Rights Act. The administration has also outlined its commitment to strengthening civil rights enforcement as part of the EPA’s strategic plan for 2022-2026, which is set to be finalized later this month.
Advocates including Bashi and Simms remain hopeful. In the first few months of fiscal year 2022, U.S. residents filed nearly as many Title VI complaints as in all of 2020. The rise in volume of complaints is actually good news, says Bashi. “For the first time in a while, communities are optimistic that the environmental injustices facing them might be honestly examined and lead to the substantive changes they have been denied for generations,” he said. As of this writing, ECRCO has caught up with its backlog of complaints, according to Gillespie. Two of the four total Title VI violations have been issued by the Biden administration’s EPA.
But that number is still miniscule and an insult, advocates say. For communities in which the EPA’s historically weak approach to enforcing civil rights law has meant ongoing exposure to pollution while they wait for answers — and losing loved ones along the way — immediate action is the only adequate intervention, according to Tamara Toles O’Laughlin, a longtime climate strategist, and CEO and president of the Environmental Grantmakers Association.
“This would look like speedy settlements and reparations for failure to respond previously; fines, sanctions and an aggressive clawing back [of] funds from predatory polluters who have built their whole businesses targeting Black, Indigenous and [other] people of color,” O’Laughlin said.
Sellstrom, of Lawyers for Civil Rights, said the withholding of financial assistance from groups found to have violated Title VI — which would be a first if and when it occurs — would also send a strong message that a culture shift is afoot within the EPA, and that addressing systemic racism in the agency may be, at long last, a serious priority. “That would change the mindset and the way people act across the board,” Sellstrom said.
Hundreds of anti-mandate protesters remained on the New Zealand Parliament lawn today as health officials reported a big increase in covid-19 cases nationally.
In a statement, the ministry said there were 32 new cases in hospital, with cases in Auckland, Tauranga, Rotorua, Wellington and Christchurch hospitals.
None are in ICU and the average age of current hospitalisations is 62.
Plastic mats being used to cover the mud at the protest occupation are being picked up by the wind and thrown across the precinct.
A man began speaking through a megaphone at lunchtime, but demonstrators do not have the full sound system setup of previous days.
Calling for PM Ardern
Some are calling out to Parliament and asking where Prime Minister Jacinda Ardern is.
Deputy Prime Minister Grant Robertson, who is also the local MP for Wellington Central, earlier warned that although people had a right to protest when “they threaten, harass and disrupt people and a whole city they lose that right”.
Parliament’s buildings are largely empty with politicans not returning to the capital until Tuesday.
The playlist booming through Parliament’s loudspeakers changed about 11am, and now includes an out of tune recorder rendition of “My Heart Will Go On”, the Titanic theme song by Celine Dion.
UK musician James Blunt earlier posted on Twitter telling the New Zealand police to contact him if the Barry Manilow music, which was playing, did not deter protestors.
His suggestion has been enacted, with his song ‘You’re Beautiful’ now on rotation.
Both songs and the government’s spoken message advising the crowd to leave the grounds are being met with loud booing and chants of “freedom”.
Streets blocked by cars
Molesworth Street remains blocked by cars, campervans and trucks and Metlink has stopped all buses using its Lambton Interchange until further notice because of the protest.
Retailers say disruption to surrounding streets has also affected their trade.
Superintendent Scott Fraser said police would continue to have a significant presence at Parliament grounds and are exploring options to resolve the disruption.
In its regular statement today, the Health Ministry noted that there had been a number of rumours circulating about possible cases of covid-19 linked to the protest.
However, the Regional Public Health Unit had confirmed that there were currently no notified positive cases linked to it.
The current cases are in the Northland (13), Auckland (623), Waikato (81), Bay of Plenty (11), Lakes (11), Hawke’s Bay (8), MidCentral (3), Whanganui (6), Taranaki (5), Tairawhiti (3), Wellington (15), Hutt Valley (10), Nelson Marlborough (2), Canterbury (3), South Canterbury (2) and Southern (14) district health boards (DHBs).
There were also 18 cases in managed isolation — five of them are historical.
Police say a protester who needed medical attention within New Zealand’s Parliament grounds last night had to wait for ambulance staff to get through the roads blocked by vehicles.
The protest against covid-19 protection measures is now entering its fifth day with police saying new tents and marquees were erected yesterday while police have strengthened protective barriers.
There are now three barriers between protesters and police in some places on Parliament grounds. This morning concrete blocks were placed before the orange and white plastic barriers.
A Ministry of Health statement said daily covid-19 cases in the community had reached a new high, up slightly to 454 today.
The new cases were in Northland (12), Auckland (294), Waikato (72), Bay of Plenty (23), Lakes (8), Hawke’s Bay (7), MidCentral (5), Taranaki (1), Wellington (5), Hutt Valley (12), Wairarapa (2) and Southern (13).
There are 27 people in hospital with the coronavirus, although none are in ICU.
There were just eight cases reported at the border today, with travellers from India (3), Australia (1), Saudi Arabia (1), United Arab Emirates (1) and the United Kingdom (1).
Ambulance for protester blocked on road
In a statement, Superintendent Scott Fraser said police remained at Parliament grounds overnight to monitor the activity of protesters.
Earlier in the evening, a protester within the grounds needed medical attention, but this was delayed because an ambulance was unable to drive directly to him due to the protesters’ vehicles blocking the surrounding roads.
Molesworth Street remains blocked by more than 100 vehicles including large trucks, campervans and cars.
Fraser said ambulance staff had to walk “some distance” to get to the man, who was waiting with officers.
‘Empathy and professionalism’
“Despite the very difficult environment, our staff, and our Wellington Free Ambulance colleagues, acted with empathy and professionalism, ensuring this man got the medical treatment he needed.”
Fraser said there was one arrest overnight for a breach of bail conditions, but there had been no arrests this morning.
A deluge from Cyclone Dovi is expected to drench anti-mandate protesters.
MetService has issued a heavy rain warning for Wellington which will be in place until 3pm Sunday and strong winds are forecast in the capital today.
This article is republished under a community partnership agreement with RNZ.
More barriers have been put up at the edge of the protest site on the lawn, and last night police installed floodlights on the forecourt.
They say it will take some time to remove everyone but Wellington District Commander Superintendent Corrie Parnell has promised the demonstrators will not be on the grounds for another week.
Watch what is happening outside Parliament:
Today’s protest happenings. Video: RNZ News
Wellington District Commander Superintendent Corrie Parnell said a number of vehicles parked illegally on Lambton Quay were moved.
He said police were repeating their order to the protesters to leave the area, as it was closed to the public and anyone remaining on the grounds was trespassing.
Expert warns protest may become ‘superspreader’ University of Otago professor of public health Dr Michael Baker told RNZ Morning Report the event had the potential to increase transmission of the virus, with protesters travelling from around the country and probably mixing with others outside their family group.
“That’s really the definition of a super spreading event and we know that’s how this virus gets around the world,” Professor Baker said.
“We’ve seen that already in New Zealand with the Soundsplash Festival in Hamilton. We’ve seen it a lot internationally at big gatherings.
“Even though it’s mainly outdoors, there will be a lot of indoor gatherings associated with it, you know, shared transport and accommodation, meals, the shouting and singing, which we know generates these aerosols,” he said.
“But the big extra problem here, of course, is that these groups, almost by definition, have low vaccine coverage low mask use. And they’re probably less likely to present for testing and self isolate if they’re sick.
“So all of those are really increasing the risks for this event.”
He said that after three days the point had certainly been made and any decision about whether to break the protest up would be a complex one, but it was currently presenting a risk.
This article is republished under a community partnership agreement with RNZ.
New Zealand’s leading daily newspaper today published an editorial exposing the “unfairness” of global media criticism of Australasian responses to covid-19, showing statistics that demonstrate how well the two countries have done.
While Australia has lost 4243 people to covid-19 out of a population of 26 million, New Zealand has lost just 53 people out of a population of 5 million.
The omicron variant outbreak that has devastated many other countries is only just taking a hold in New Zealand with a record 306 community cases reprted today — 216 of them in Auckland.
“Australia’s announced reopening of its borders to vaccinated tourists and other visa holders from February 21 drew the expected foreign media reaction,” said the New Zealand Herald in an editorial headlined “How hard has NZ really gone on covid-19?”
But the newspaper contrasted the saving of lives in Australasia with the global devastation caused by the covid-19 pandemic worldwide with 403 million cases and 5.79 million deaths.
“The BBC noted that ‘Australia has had some of the world’s strictest border controls throughout the coronavirus pandemic’ with the country ‘even banning its own people from leaving the country last year’.
“Reuters said the move ended ‘two years of misery for the tourism sector’ and AFP summarised it as “the rules have stranded nationals overseas, split families, hammered the country’s multibillion-dollar tourist industry, and prompted often bitter debates about Australia’s status as a modern, open and outward-looking nation’.”
Financial costs, not lives saved
The Herald said that coverage had focused far more on financial costs and Australians stranded overseas than lives saved.
The newspaper cited head of Tourism Australia Phillipa Harrison as saying that Australia had been “a little bit ridiculed” for its border closures and other rules and warning that it could have an impact on its tourism recovery.
“Australia, like New Zealand, has become synonymous with strictness in dealing with the coronavirus. It is a narrative that has taken hold, but is this image fair?” asked the Herald.
Both countries had certainly made the most of their island borders and geographical isolation.
“Australia has a death rate of 163 per million people from covid-19 and New Zealand’s is 11, according to the Worldometer website, The Herald reminded its readers.
“Japan (154), South Korea (134), and Singapore (147) have also done well. Major countries with death rates over 2000 include the US, Brazil, France, the UK, Russia, Italy, Spain, Belgium and Greece.”
Australia’s closures of state borders and Auckland’s lockdown fence had all drawn attention to covid measures in this part of the world, sid the newspaper.
Australasia ‘sticks out’ in pandemic
“It has made Australasia stick out in a pandemic that has been politicised around the world, even though other countries have also used tough requirements.”
The Herald said a time lag between when pandemic events such as variant surged and vaccine rollouts occurred overseas could give the impression other countries had not also been stringent.
“For instance, when New Zealand initially delayed reopening borders, omicron was setting record case numbers overseas and vanquishing delta. France, Ireland, the Netherlands, Norway and Denmark are just now starting to ease restrictions but their omicron waves began towards the end of last year.”
On the Oxford Stringency Index, which tracked governments’ coronavirus responses, neither Australia nor New Zealand’s ratings — 55.56 and 62.04 — were out of the ordinary.
“For instance, Canada, Italy, Greece, Germany and France are rated more stringent,” said The Herald.
New Zealand had had vaccination mandates in sectors such as health, education, emergency services, police, and defence.
“In Europe a variety of mandates target specific groups. Germany requires vaccination for the military, in Britain it is compulsory for nursing-home staff. Greece has ordered people aged 60-plus to have it and in Italy people over 50 can be fined if they aren’t vaccinated.
Extensive European border controls
“Austria requires most aged 18 and over to get vaccinated against covid-19.
“European countries have had extensive border and travel requirements. In December, France temporarily banned travellers from Britain and Germany imposed quarantine on them.
“There has also been extensive use of vaccine passports. Ireland had a night-time curfew in December.
“Several European countries have used outdoor mask mandates and required the wearing of specific types of high-quality masks. America’s most populous county of Los Angeles has had a mask mandate for large outdoor events as well as for outdoor spaces at schools and childcare places — on top of indoor mask requirements,” said the newspaper.
“Citizens in other countries have been confronted with huge death counts, infections and long covid. That’s family members and friends lost.
“Kiwi expats have drawn attention to the shortcomings of MIQ, but a new poll shows most voters steady in their views on how the government is performing.
“Once most countries are reconnecting and the pandemic eases, the figures remaining for posterity will show how countries fared in health and overall economic terms.”
Proud of Ardern’s leadership
Among letters to the editor supporting NZ’s MIQ border policies published by the newspaper today, one New Zealander living in Mansfield, Pennsylvania, wrote: “I am proud of the intelligent way [Prime Minister] Jacinda Ardern has dealt with border control during covid-19”.
She added: “Here in the US, the death toll has reached nearly a million. We have been in self-imposed lockdown for nearly two years …
“New Zealanders have never had to live under Trumpism, Hitlerism, PolPotism, or other despotic regimes. Please be worthy of the soldiers, such as the Anzacs, who fought to keep the world safe for democracy. Did they die in vain?
“Please give Jacinda Ardern the respect she deserves.”