A protest at New Zealand’s Parliament has stretched into a third day with a group camped out on the grounds and nearby streets.
Authorities have told the group protesting at covid-19 vaccine mandates to leave, but there have been no signs of that so far.
Police are continuing to advance slowly into the protest on the parliamentary precinct, with lines of officers gradually moving into the crowd and making arrests.
Well over a dozen people have been arrested so far today in the efforts to clear the protest.
Some protesters have responded with abuse, haka and hurling objects at officers.
The Speaker has authorised the closure of the Parliamentary precinct, if the police deem it necessary to clear the lawn.
Live: The anti-mandate protest today. Video: RNZ News
‘Move on’, Ardern tells protesters
Prime Minister Jacinda Ardern today told anti-vaccine mandate protesters outside Parliament to ‘move on’.
She spoke after visiting a covid-19 vaccination centre in Albany, Auckland.
Ardern said it was ultimately an operational matter for police about handling the protest.
“Obviously every New Zealander has a right to protest, but there are also rules around what is able to happen on Parliament’s forecourt and of course we would expect that people have behaviours that don’t disrupt the ability of others to go on with their lives as well,” she said.
Ardern said she thought the majority of New Zealanders shared a similar sentiment, to keep one another safe and live their lives and do as much as they could do to ensure they could continue to live our lives as they did before the pandemic.
This article is republished under a community partnership agreement with RNZ.
Police lead away a protester from the Parliament grounds. Image: Angus Dreaver/RNZ
COMMENTARY:By Dr Mark Craig in defence of New Zealand’s dedicated managed isolation and quarantine team and facilities as the country braces for omicron.
As workers on the ground running ourselves into the ground, it’s quite disheartening to read all the reactionary criticism of MIQ, the managed isolation and quarantine system which has saved thousands of lives in New Zealand.
It’s easy not to appreciate what it has achieved, given it has prevented something awful from happening, and only see the restrictions and disadvantages it has necessarily caused by its existence.
Also, most of the people who have been spared from severe illness are not the ones who are complaining.
I am so impressed with the small and dedicated MIQ teams I have worked with — a throw-together of excellent nurses, health care assistants, well-being coordinators, security, hotel staff, police and the impressive NZ Defence Force.
These people are gold and the cornerstone of preventing a certain healthcare system crisis.
They have retained great professionalism in the face of numerous extremely challenging guests and logistics around dealing with covid positive cases while keeping them as happy as can be in a confined space.
Currently we are full of overseas border returnees from all over the world, many angry at being in isolation and taking it out on our staff, to the point where absenteeism is common and job satisfaction has dipped hugely.
Staggering towards MIQ end
We are all staggering towards the end of the MIQ system, rather punch drunk and weary.
Our staff currently receive relentless angry calls from guests who don’t get what they want immediately, currently often the investigation of potential historical covid status (of which there are dozens presently), more than one expressing “there will be blood on the walls” if their immediate demands are not met.
I can understand why to a degree — they are stuck in a room and can’t see the huge amount of work going on behind the scenes, with teams putting in long tiring days, well over their paid hours, but unfortunately it also brings out the worst in some people of certain personality types and those with mental health issues.
Dr Mark Craig … “The small and dedicated MIQ teams I have worked with are gold and the cornerstone of preventing a certain healthcare system crisis.” Image: Jason Oxenham/NZH
Also I must add that a majority of people are able to “just get on with it” and do the time, something most of us would find tedious.
There is a financial cost to saving lives in any area of healthcare and now it has been deemed the harms of MIQ outweigh the benefits, rightly in my and most people’s opinion, as covid spreads in the community and borders open up.
If only we could have the same political will and public acceptance that we have had for lockdown and vaccination programme to put preventative health measures and laws to address the two other huge elephants in the room, our chronic disease epidemic and environmental crises.
Firm beneficial health laws
We could reduce our health spending by orders of magnitude while greatly improving health if we had some firm laws for clearly beneficial proposals such as sugar and fat taxes, and the marketing of harmful, processed foods and alcohol, especially at our children.
We could equally slash our carbon emissions whilst raising health outcomes with the promotion of a plant based type of diet, as per the current international public health consensus.
We just need to be brave, follow the science and not give in to the numerous interest group detractors. Our world beating covid response has shown we can do it.
Let’s keep the momentum up and not go back to our pre-covid slumber.
Dr Mark Craig is an Auckland-based lifestyle medicine doctor working in managed isolation and quarantine facilities. This article was first published in the New Zealand Herald and is republished here with the author’s permission.
Police handcuffed three people after protesters today tried to push through a barrier on the grounds of New Zealand’s Parliament — known as the Beehive.
The group is part of a convoy which travelled to the capital Wellington yesterday to protest against covid-19 vaccine mandates.
After trying to push through the blockade this afternoon, three people were handcuffed and led away.
About 100 police formed a ring around the front of Parliament edging up to a line of protesters who had linked arms lining up in front of the Cenotaph war memorial.
In a statement, the ministry said the new community cases were in Northland (8), Auckland (135), Waikato (35), Rotorua (1), Taupō (1), Bay of Plenty (11),Taranaki (1), Palmerston North (2) Wellington (3), Hutt Valley (3), Nelson Marlborough (1), Canterbury (3)
There are 16 cases in hospital, although none are in ICU.
The ministry said there were 46 cases in MIQ reported yesterday, with travellers arriving from India, Sri Lanka, Egypt, Pakistan, UK, Australia, Fiji, Bangladesh, Saudi Arabia, France, USA and the Philippines.
More than 50 police have formed a ring around the front of New Zealand’s Parliament today edging up to a line of protesters who have linked arms lining up in front of the Cenotaph.
One person speaking said he would walk up the Parliament steps at 3pm and get arrested, inviting others in the crowd to join, saying “see you at 3pm” to cheers from the crowd.
The group is part of a convoy which travelled to the capital Wellington yesterday to protest against covid-19 vaccine mandates.
Trucks and other vehicles are blocking Molesworth Street.
Police issued a statement late last night saying they were monitoring the situation and were talking with the Speaker of the House Trevor Mallard.
The protest scene today outside Parliament. Video: RNZ News
This article is republished under a community partnership agreement with RNZ.
Protesters have been given a letter from the Speaker setting out Parliament’s rules, which prohibit staying overnight on the grounds and ban tents or other structures.
Specific policies mentioned in the letter include leaving the grounds in an orderly manner and not interfering with traffic.
“Participants must assemble within and disperse from the grounds in an orderly manner, and so as to not interfere with the flow of vehicular traffic.”
Police forming a ring around the front of Parliament today. Image: Jane Patterson/RNZ
It also mentions that tents and structures are banned from the grounds.
“No erection of tents or any structure is permitted other than hand held signs … structures including tents as mentioned above are not permitted and if not removed when requested, are liable for confiscation.”
Protesters outside Parliament. Image: Jane Patterson/RNZ
It said if the rules were breached people could be trespassed and their equipment confiscated.
“In line with these existing policies, please disassemble any tents or structures and remove them from the grounds. Do not continue protests or demonstrations on the grounds after dark. The breach of the above policies and failure to carry out the actions may result in trespass notices being issued.”
A truck and vans from the convoy covered in protest messages. Image: Hamish Cardwell/RNZ
There are also campervans parked in nearby streets and the police say Molesworth Street in front of Parliament is not accessible to traffic, and drivers should avoid the area this morning.
It is not clear how long the protesters will be allowed to stay.
Tents set up in the grounds of the law school over the road from Parliament. Image: Hamish Cardwell/RNZ
Wellington City Council is talking with police about their options to deal with cars illegally blocking the roads and footpath near Parliament.
Council spokesperson Richard MacLean said if cars were to be removed there would be resources needed.
He said the council wants to avoid confrontation but are planning for if it were to arise.
Motorists are still being advised to avoid the area if possible.
The scene from the front lawn of Parliament. The media are no longer allowed on the grounds. Image: Hamish Cardwell/RNZ
This article is republished under a community partnership agreement with RNZ.
Several hundred more cases of covid in Solomon Islands … Kiribati records first covid death …nearly 12,000 in isolation in New Caledonia … French Polynesia records first covid death in nearly four months … Federated States of Micronesia calls a halt to flights from neighbouring Guam … a partial border re-opening in the Northern Marianas … and Papua New Guinea’s Prime Minister James Marape says he is “doing well” while self-isolating at home from a covid-19 infection.
One death has been recorded — the first since October, taking the death toll to 637.
More than a third of the covid-19 cases are the omicron variant.
Four people are in hospital and one person in ICU.
The proportion of the population vaccinated is 78.6 percent.
FSM halts incoming repatriation flights The Federated States of Micronesia has indefinitely stopped all incoming repatriation flights from Guam.
FSM’s Covid-19 Taskforce said the move was in response to the high number of coronavirus infections in the US Territory.
In a statement, the taskforce said it was essential for FSM to improve its vaccination rates before restarting flights to bring back citizens stranded in its neighbouring Guam.
The government said it would provide assistance for citizens who are stuck in Guam, but not provide further details at this stage.
Covid-19 vaccines are mandatory on the islands of FSM — meaning all citizens residing in the FSM must be vaccinated.
FSM’s public health emergency has been extended until the end of May.
Partial border reopening in the CNMI The Northern Marianas has reopened its borders for fully vaccinated people.
The changes to the border protocols were made possible with 99 percent of CNMI’s eligible population now fully vaccinated, and 53 percent having had booster shots.
CNMI’s Covid-19 Taskforce said all travellers entering the territory by air or sea would no longer be tested on arrival.
Unvaccinated travellers, however, will be required to quarantine at home and get tested at a community based testing site five days after arrival.
All visitors to the Northern Mariana Islands will also need to complete a mandatory health declaration and upload their vaccination status.
Authorities say the health and safety of residents remain the top priority of the government.
The CNMI has recorded more than 6300 cases and 23 deaths.
Marape had to cut short his visit to China after he tested positive for coronavirus in Beijing last week.
In a statement yesterday, Marape said “there is nothing seriously wrong with me” and that “vaccination has really helped”.
He said he would be taking a second covid-19 test tomorrow and depending on results would provide an update on Friday on when he would resume his responsibilities.
His deputy Sam Basil is acting prime minister while Marape recovers.
The prime minister is urging fellow PNG citizens to get vaccinated.
PNG has one of the lowest vaccination rates in the world, with less than 3 percent of the population covered.
This article is republished under a community partnership agreement with RNZ.
After a record number of covid-19 cases were reported on Saturday, New Zealand’s prime minister believes the country’s omicron peak may be in late March.
The number of omicron cases in New Zealand has not yet reached the number predicted by modellers.
However, New Zealand recorded its largest ever one-day case number with 243 cases on Saturday. On Sunday the cases dropped to 208 and on Monday, there were 188 new cases.
But with the long weekend came lower testing rates. Fewer than 13,000 people were swabbed for covid-19 on Sunday, at least 5000 down on the most recent weekdays.
Epidemiologist Professor Michael Baker believed the daily case numbers may not reflect the true extent of community spread.
Omicron only became a variant of concern at the end of November 2021, it was still very difficult to predict its behaviour, Prime Minister Jacinda Ardern told RNZ Morning Report.
“While there’s uncertainty in case numbers, if you looked at low case profiles in a place like say South Australia and you applied that to New Zealand, you would have something like 10,000 cases a day at its peak.”
High scenario
A high scenario like in New York would mean 30,000 cases a day, she said.
“It’s widely variable and ultimately the defining feature of where we will peak will be booster uptake. The more people who take a booster, the lower the likelihood of our peak.”
Ardern believes New Zealand’s omicron peak may be in late March.
Asked if she regretted not prioritising Māori in the vaccine rollout, Ardern said everything they learnt in the first rollout, they were applying to every vaccine rollout since.
She said the government has worked really closely with Māori on the rollout of paediatric and booster campaigns.
“On the first rollout, we didn’t have the supply to rollout to everyone and so we took an approach that said a whānau-based approach but also one based on those who were at the highest risk.
“And look, I stand by that, but again, as I say, every stage we’ve learnt lessons.”
90% Māori vaccinated Ninety percent of Māori have now have at least one dose of a covid-19 vaccine.
Labour is on 44.3 percent, up 1.6 percentage points and National on 31.3 percent, up 4.4 percentage points.
Ardern said she would not pin Labour’s results on any one thing.
“Ultimately this is again, support for the plan we have and that has been a plan always based on making decisions that are in the best interest for New Zealanders, their health, their wellbeing and our economy,” she said.
“We are in a phase now of shifting up the way that we’re approaching the pandemic, moving to reopen, greater freedoms … and I think we see people are generally supportive of that plan.”
Anti-vaccine convoy to Parliament A convoy of people protesting against the government’s covid-19 protection measures was expected to arrive in Wellington today.
Ardern told Morning Report she would not be meeting protesters at Parliament.
Lockdowns meant people sacrificed some of their usual rights and abilities to keep others safe, she said.
“Of course New Zealanders all through this pandemic have given up something but in order to gain the health and wellbeing of all communities and it’s worked.”
She said now people were living with fewer restrictions than earlier in the pandemic.
The protest came at a time when the government was changing the way it was doing things because of the extra protection vaccines provide, she said.
This article is republished under a community partnership agreement with RNZ.
As COVID-19 continues to rage, another health crisis persists — one that is decades long. In the first year of the pandemic, the United States hit the devastating milestone of 100,000 overdose deaths, a nearly 28.5 percent surge from the record numbers we saw the previous year. Now, fentanyl is the leading cause of death in Americans ages 18-45. The reaction from many of our leaders has been to call for more arrests and criminalization, but this response is rooted in fear, not science. We have spent the last 50 years trying to treat a public health issue with a criminalization response, yet people are dying of overdose at record rates. This response is clearly not working.
The evidence is clear: Criminalization worsens public health outcomes. From making the drug supply more dangerous, to deterring people from getting help out of fear and stigma, to denial of economic opportunities and supports for people with drug arrests, the associated consequences have been dire. Besides, sending someone to jail or prison doesn’t keep people from using drugs. In fact, deaths due to drug and alcohol intoxication have increased more than 600 percent in state prisons between 2001 and 2018.
It’s time for a new approach. Oregon has taken the bold step that we should adopt across the U.S.: Decriminalize drug possession and increase access to health services. In the year since the state decriminalized drugs through a ballot initiative (Measure 110), and with only about 10 percent of the allotted funding distributed to 70 community-based organizations so far, Oregon has already been able to provide peer support, harm reduction, evidence-based treatment, housing and job assistance to more than 16,000 people.
Prior to this measure passing, Oregon ranked last in access to treatment and recovery services.
And yet, since the passage of decriminalization, many local media outlets in Oregon have fixated on a lack of citations from police for drug possession. (Under Measure 110, people found in possession of small amounts of all drugs receive a citation and $100 fine instead of being arrested.) This is a distraction, and the wrong way to measure the program’s success.
In fact, decriminalization efforts shouldn’t involve police. Police involvement often harms people who use drugs. Addressing drug use through the criminal legal system has contributed to mass incarceration and family separation, and has saddled people with criminal records that affect their ability to get housing, employment and live full lives. It has allowed public officials to neglect their responsibility to support people, and instead inflate police departments to become military-style operations while continually divesting from health and support services that people desperately need. Even some police will tell you that their options for response are limited and that a different set of tools are needed. Since decriminalization has taken effect in Oregon, thousands of harmful drug arrests have been avoided.
Some call Oregon’s efforts an “experiment,” but they are already grounded in evidence: They’re largely based on the successful model adopted in Portugal over 20 years ago. Within a few years of implementing decriminalization in Portugal, the number of people voluntarily entering treatment increased significantly, while overdose deaths, HIV infections, problematic drug use and incarceration for drug-related offenses plummeted. And Portugal is not an anomaly. Many other countries, including Switzerland and the Czech Republic have implemented varying degrees of decriminalization with similar success.
The logic is simple. When people are given access to health services and no longer fear being criminalized if they seek them out, they are more likely to do so. And if we address the full range of people’s needs — including harm reduction services, housing and even job assistance — versus just mandating abstinence, we are able to actually get people on solid footing and better address the underlying factors that contribute to chaotic drug use. We’ve seen this in Portugal and are getting a glimpse of it in Oregon.
Even though Oregon’s move is a huge step forward, there remains more work to do, such as removing quantity thresholds and police altogether, inclusion of expungement and resentencing for past drug arrests and convictions, and ensuring access to things like overdose prevention centers and safe supply. As we work to decriminalize drugs in other states and federally, these additional provisions, such as increasing the amount of drugs that would qualify as personal possession — should be strongly considered, in order to truly embrace the public health alternative this is meant to be.
Decriminalization is a shift a majority of people want to see. According to the latest polling, 66 percent of Americans support removing criminal penalties for drug possession and investing in health services. While Oregon may be the first in the U.S., it certainly won’t be the last. Since this measure passed, we have seen over half a dozen other states and Congress introduce legislation that would decriminalize drug possession.
Amid the twin crises of overdose and criminalization, we owe ourselves and our communities a different approach — one that empowers people to live healthy and free lives. Decriminalizing drugs and creating access to care are necessary steps in that direction.
A public health expert is urging New Zealanders to keep up the testing momentum, as testing rates take a dive over the long weekend.
Fewer than 13,000 people were swabbed for covid-19 in the past day, at least 5000 down on the most recent week days.
University of Otago senior lecturer Dr Lesley Gray is encouraging anyone with cold or flu-like symptoms, no matter how mild, to get tested for covid-19.
“We know that for those people that will get symptoms, it may start as simple as sneezing, a scratchy throat, a bit of a runny nose as if it were a run-of-the-mill cold,” she said.
“So, if you do get any of those symptoms, especially a scratchy throat, please do go forward and see if you can get tested.”
Gray said anyone who is feeling well should make a habit of regularly checking the Ministry of Health’s locations of interest, to see if they have been exposed to the virus
“It could be that if people are acquiring omicron, assuming there are more cases in the community, then we’ve got to accept that some people will not actually have any symptoms.
“So unless they identify that they may have been at a location of interest, or that they may be a close contact, they may be completely oblivious to the fact that they may also have covid-19.”
Several new locations of interests have been added to the Ministry of Health’s website, including Air New Zealand flights, a Wellington restaurant, a Taupō cafe and a mosque in Hamilton.
Gray said it was important New Zealanders kept up the public health measures that had served the country well throughout the outbreak, such as masking, physical distancing, keeping a record of movements and staying home if unwell.
“If people identify their symptoms early, then take the steps to see if they’re a positive case, it makes a huge difference. We’ve all got families and nobody wants to be transmitting this to other family members, especially our young tamariki.”
This article is republished under a community partnership agreement with RNZ.
About 67 percent of the total population of 272,000 is fully vaccinated.
Last week, Paris declared a health emergency in New Caledonia but the French High Commission in Noumea decided against imposing another lockdown.
Some restrictions were introduced after last month’s detection of the omicron variant, limiting the size of meetings and upholding mask wearing obligation.
Protest over masks in schools
Defying the policy, hundreds of people demonstrated on Saturday to show their opposition to mask wearing obligations in schools.
Since last Tuesday, antigen tests are no longer free but cost a minimum $US27.
The change upset some traditional leaders in the Loyalty Islands, who then demanded the suspension of the health pass, needed to board flights.
The dispute briefly closed the airport on Lifou, and tests for flights to and from Noumea are now free again.
In September, the territory’s Congress passed a law making vaccinations mandatory, but its application has been repeatedly deferred and is now not expected to be enforced before the end of the month.
This article is republished under a community partnership agreement with RNZ.
A team of four experts from China have arrived in Honiara for on-site feasibility studies on two projects amid the surging case of covid-19 in the Solomon Islands.
The experts are here at the invitation of the government for studies on the upgrading of the national referral hospital and a new water plant.
Sogavare said this was within 20 days of the country’s first case of domestic transmission of the virus, reports RNZ Pacific.
He said that on Friday alone, health officials had identified 430 cases.
Sogavare put the official death toll at 32 but other deaths are believed to have occurred at home.
The prime minister said all but three provinces have reported cases, and transmission was now widespread in the capital, Honiara.
Many of the local lockdowns that had been in place has been lifted but a curfew from 6pm to 6am will still be enforced.
Movement out of Honiara is not allowed.
The prime minister has repreated calls for people to get vaccinated.
Boost for bilateral relationship
The arriving Chinese expert team said in a statement: “Hopefully our arrival can help Solomon Islands strengthen infrastructure construction, improve medical conditions and livelihood, and boost development of bilateral relationship.”
The team, which has strictly complied with Solomon Islands’ quarantine procedures, said its arrival, work and persistence would promote the country’s anti-pandemic work and improve the public medical environment and infrastructure.
In the spirit of “Umi togeta against covid-19”, the team vowed to deliver its best in the fight against the pandemic in Solomon Islands.
“Our team will stand firmly with our friends in Solomon Islands, defy difficulties and dangers, work hard, and build a modern diagnosis and treatment place with advanced technologies for Solomon Islands with the latest construction technologies in the foreseeable future,” the team added.
Robert Iroga is editor of SB Online. Republished with permission.
New Zealand has recorded its highest number of community cases in one day, with 243 new cases reported today.
The previous highest number of cases reported in one day was 222 during the delta outbreak in November.
In a statement, the Health Ministry said the continued increase in cases today was “a reminder that, as expected, the omicron variant is spreading in our communities as we have seen in other countries”.
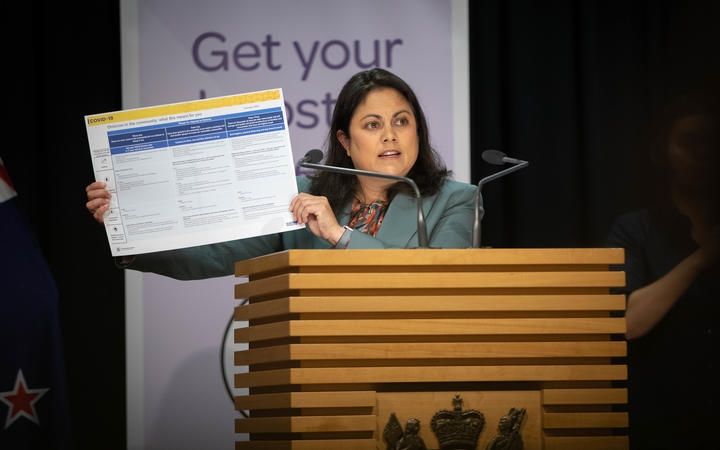
The ministry said getting a booster dose as soon as it was due was one of the best steps to take.
“Boosters lower your chances of getting very sick and being hospitalised. Being boosted also helps slow the spread of the virus. If you’re over 18 and your booster is due, please get it now.”
Covid-19 Response Minister Chris Hipkins said today’s record numbers were expected and would continue to grow in the coming days and weeks
“I urge people not to panic but to plan for that,” he said.
‘Get your booster’
“The best thing you can do to prevent illness is to get vaccinated, and get your booster. Wear a mask when you’re around others, cough into your elbow and wash your hands regularly.”
It was a record day for boosters yesterday, with 66,864 booster doses given. There were also 876 first doses, 1780 second doses and 4440 paediatric doses given.
There are 10 people in hospital with covid-19, including one in ICU. Two are in Rotorua and one in Christchurch, with the rest in Auckland hospitals.
Today’s new community cases were in Northland (21), Auckland (165), Waikato (34), Rotorua (1), Bay of Plenty (8), Tairāwhiti (2), Hawke’s Bay (6), Nelson/Marlborough (3), Whanganui (1), and Wellington (2).
The 21 new cases in Northland include 14 cases in Kerikeri, two cases in Kaeo, one case in Kaikohe, three cases in Whangārei, and one case in Taipa Bay-Mangōnui.
Less than half of the 34 cases in Waikato today are linked to previously reported cases. Nineteen of the cases are in Hamilton, five in Ohaupo, two in Te Kuiti, two in Ngāruawāhia, one in Tirau, and the remaining with locations under investigation.
Both of the Wellington cases are under investigation for links to previous cases, but a JetStar flight between Wellington and Auckland on January 29 has been added as a location of interest. More details are available on the ministry’s location of interest page.
There were also 26 cases reported at the border today, with travellers arriving from Singapore, Australia, UK, India, Egypt, Lebanon, UAE and Ireland.
Air travellers were left stranded and fuming country-wide as airlines Air Niugini and PNG Air hit a rough patch in operations due to wet weather and a large number of their key staff falling sick and unable to be at work.
Flight cancellations were the order of the day yesterday at many airports with passenger backlogs and frustrations growing.
Air Niugini, especially, has had flight cancellations since last November.
The airline has issued an apology saying wet weather conditions and staff absenteeism had caused the situation.
In a media release, both airlines apologised for a number of flights in recent days which have been disrupted due to a much higher number of crew than usual falling sick, as well as the current bad weather conditions across the country impacting on the airlines’ operations.
Both airlines say they are doing everything they can to manage the situation, but will not compromise safety operations.
Stranded passengers had to rebook flights and spend extra money for accommodation and transport.
Backlog mostly tertiary students
Most on the backlog of passengers are tertiary students and parents who have been asked to rebook flights for four to five days as of last Wednesday.
While the airlines have not publicly stated if staff were infected with covid-19, reliable sources from within companies have informed the Post-Courier that a majority of those sick and absent from work were infected with the virus.
They included aircraft engineers, high-end ground staff, pilots, cabin crews and protocol staff.
One of the stranded passengers from Lae, former EMTV senior journalist Scott Waide took to social media to comment on the crisis, which attracted a lot of responses and complaints from passengers who were in a similar situation.
They describing the customer service by the airlines as poor.
Waide was asked to rebook his flight more than once and finally made it into Port Moresby late yesterday evening.
An unfortunate incident happened at Nadzab Airport in Lae yesterday when an airline staff member allegedly insulted a female passenger.
Staff member ‘tears up’ boarding passes
Josephine Kawage claimed the staff member tore up her and her child’s boarding passes.
Kawage said in a video recording that they had been stranded for four days and were finally put on the flight yesterday. However, the check-in officer was only able to produce two boarding passes for Kawage and her son.
She said that she was humiliated when she asked for the boarding passes for her other family members.
A disappointed husband, Captain Henry Nilkare from the North Coast Aviation, condemned the alleged actions of the airline staff member when he spoke to Post-Courier last night.
He said he would take the matter up with Air Niugini to have the officer penalised.
“I do work in the airline industry and understand the nature of his job at situations like this, but his actions were uncalled for and no passenger, or any woman with an infant, should be treated as such in front of many people,” he said.
“That is a bad image for Air Niugini and I do not wish to see this happen to any other passengers.
“If he can do this to my wife and child, who knows how many people he may have treated badly.”
Captain Nilkare said he would be flying to Lae himself to pick up his family today.
Melisha Yafoiis a PNG Post-Courier reporter. Republished with permission.
With the arrival of the omicron variant on our shores, it is hard to believe, judging by the media coverage — particularly on MIQ, that the Aotearoa New Zealand government has got anything right in its pandemic response.
One important feature that has been missed in the debate on New Zealand’s pandemic response to date, however, is our very low death rate. At under 60, it is 0.5 percent of the rate in the United Kingdom – approximately 10 per million, compared with more than 2000 per million in the United Kingdom.
This is a very important metric that has been given too little regard here and overseas. The number of people dying of covid-19 in the UK is well over 150,000. This figure is confirmed by the data on excess deaths estimated against the long-run average; the two numbers closely correspond.
In other words, the deaths wrought by covid are on a scale comparable with a major outbreak of warfare. And yet too many commentators and decision-makers have become inured to this death toll, concentrating instead on the performance of the health system and the enjoyment of individual freedoms.
If we had suffered the same rate of covid deaths as the UK has, that would make the number of deaths not 50-60 but 10,000, not far short of the number of New Zealanders dying in World War II (just under 12,000).
The scale of death — or the potential for death — therefore needs to feature more prominently in the coverage of the politics of the pandemic.
‘Let the bodies pile high’
For example, British Prime Minister Boris Johnson is said to have stated that he would prefer to “let the bodies pile high” rather than pursue another lockdown.
True or not, that reported statement had almost no impact on his popularity compared to stories of his attending parties at Downing Street when the UK was under firm restrictions on gatherings.
This blind spot in the media coverage and cultural resonance of the pandemic came home to me when a columnist in the left-of-centre publication New Statesman pointed out that, pre-omicron, her friends in Australia didn’t know a single person with the virus, and yet their state and federal governments at that time were pursuing far stronger public health measures than were being applied the UK.
The same could have been said of New Zealand since the two countries have followed similar policies.
Yes, most Australians — and New Zealanders — pre-Omicron were unlikely to know anybody with the virus; but neither were they likely to know anybody who had died of it, which is in many respects a far more important metric both ethically and politically.
Arguably, New Zealand — like Australia — is a more communitarian country, with “two degrees of separation” and all that. Thus, it might matter that bit more to us whether or not our neighbour, friend, or relative dies of a pandemic disease.
In larger, more anonymous societies there is less proximity to death.
Pictures of morgues
At present anyway, pictures of morgues piled high with the dead from the pandemic would be socially unacceptable in our culture. Added to this is the special place of Māori, who could suffer disproportionately with a premature opening of our borders.
This is something that Grounded Kiwis, the expatriate New Zealanders’ group pushing the legal case against the government, may have missed. If it forces the hand of the government to open our borders before we have been able to achieve acceptable levels of both vaccination and infection protection — such as masking, ventilation, distancing, and self-testing against the onslaught of omicron – then the consequences may also be an increase in the likely death rate in New Zealand.
For example, New South Wales at the peak of its omicron outbreak recorded rather more deaths in a single day than New Zealand had recorded over the near-two years of the pandemic, despite the supposedly milder and less impactful character of this variant.
Is that really what we want?
It is also as well to remember our responsibility to all vulnerable populations, including the elderly, Māori and Pasifika, and all those with relevant underlying health conditions. These groups have suffered disproportionately in the pandemic so far.
Few of us have experienced over a short time and in a proximate way significant numbers of deaths in our circles. Half a century ago, it was more common for people to die at home, often surrounded by family, but this has become much less so.
These days it is more likely to be professionally and medically managed, with much of our experience of death otherwise coming packaged via mass and social media.
The government — and New Zealanders — have done well to keep pandemic death at bay. This is not to justify draconian measures without considered trade-offs against wider societal costs and benefits.
But it is to argue for a more balanced discussion of our pandemic response, and to show greater respect for the more communitarian style of it.
Peter Davis is an elected member of the Auckland District Health Board, and emeritus professor in population health and social science at the University of Auckland. His article was first published at Stuff and is republished on Asia Pacific Report with permission.
As of early December 2021, nearly 70.4% of Indonesians had received one dose of an approved COVID-19 vaccine. Particularly considering the arrival of the Omicron variant in Indonesia, this is certainly cause for celebration. But this figure obscures important sources of discrepancies: while nearly all eligible adults in Jakarta are reported to have received at least one dose, less than a quarter of those in Papua have done so, for instance.
Geography is only one axis of inequality, however: other sources of vaccination inequity are less easy to measure. Part of the problem may stem from inequality in access, as some people may simply continue to have a better chance to get the jab than others, owing to connections or willingness to pay. Over the last year, governments across the world were embroiled in scandal as they offered differential access to vaccines to wealthy individuals. Looking at Indonesia, in particular, Lila Sari has documented how political parties in Indonesia have played a crucial role in vaccine delivery—doling out jabs to supporters as a means of shoring up votes. [related article]
Data availability is a major difficulty in adjudicating the extent of these problems: while publicly reported data indicates the overall uptake of vaccines according to region and occupation, we know very little about the sorts of individuals receiving these jabs. More concerningly, we know even less about those individuals who do not wish to receive a vaccination. Identifying and reaching these uninoculated populations is particularly crucial as the pandemic continues to drag on, and vaccination remains the best tool for combatting serious illness.
To fill in these gaps, we analyzed data from two nationally representative surveys of Indonesian adults conducted in March (N = 1,064) and October 2021 (N = 981). These data offer a unique window into how Indonesia’s vaccination campaign is being received by the individuals it intends to reach. We seek to answer several related questions. Firstly, which groups are getting vaccinated? Secondly, which groups are expressing an interest in getting the vaccine, but not able to do so? And finally, why is it that some people do not want the vaccine? We take up these questions and consider the implications for the equitable roll-out of vaccines in Indonesia.
We home in on one particularly concerning finding: as of October 2021, older Indonesians, the most vulnerable segment of society, are the least likely to be vaccinated and the least interested in seeking out the jab. The role of misinformation looms large in this finding, as it appears the tendency for older Indonesians to resist inoculation is a function of their lower levels of education than younger cohorts. Developing strategies to reach this population is particularly crucial for stemming the tide of the pandemic.
Who is getting vaccinated in Indonesia?
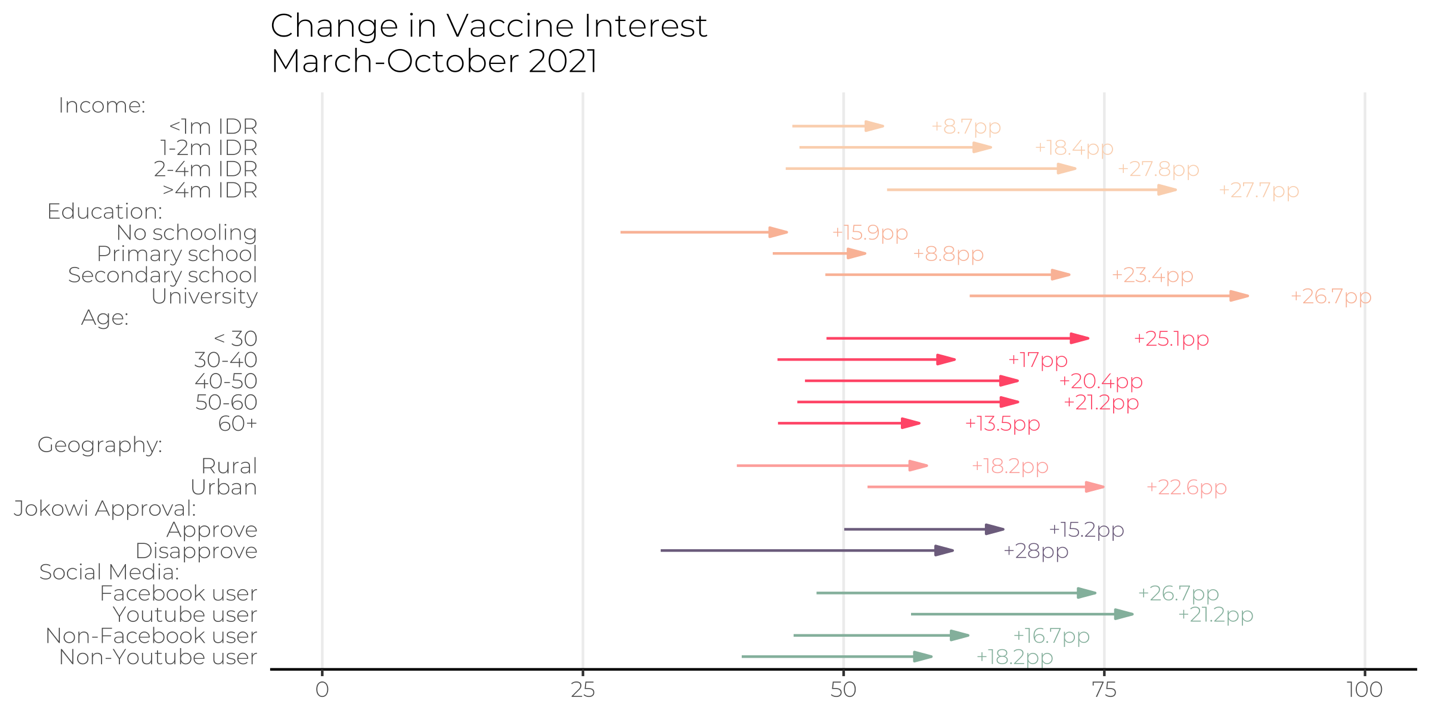
Our survey finds that in early October 2021, 42.1% of adult Indonesian had received at least one dose of a vaccination—slightly higher than officially reported statistics. In Figure 1, we show the percentage point increases for individuals in different subgroups—according to income, education level, age, and geography. In March 2021, no subgroup reported more than 5% vaccination rates. As the roll-out of vaccines took place of the past 6 months, however, stark differences in vaccination rates have emerged: richer and better educated Indonesians have outstripped their poorer and less educated counterparts in the rush to obtain vaccinations. By October 2021, for instance, 71.2% of college graduates had received at least one jab, compared to 15.4% of those with no formal education.
In surprising contrast with other countries—where vaccine rollouts targeted older citizens first—Indonesians under 30 are significantly more likely to be vaccinated (51.6%) than their older counterparts. Given that COVID-19 is more likely to result in severe illness or death for the elderly, it is particularly concerning that only 33.6% of Indonesians older than 60 had received a dose of the vaccine by the fielding of the survey.
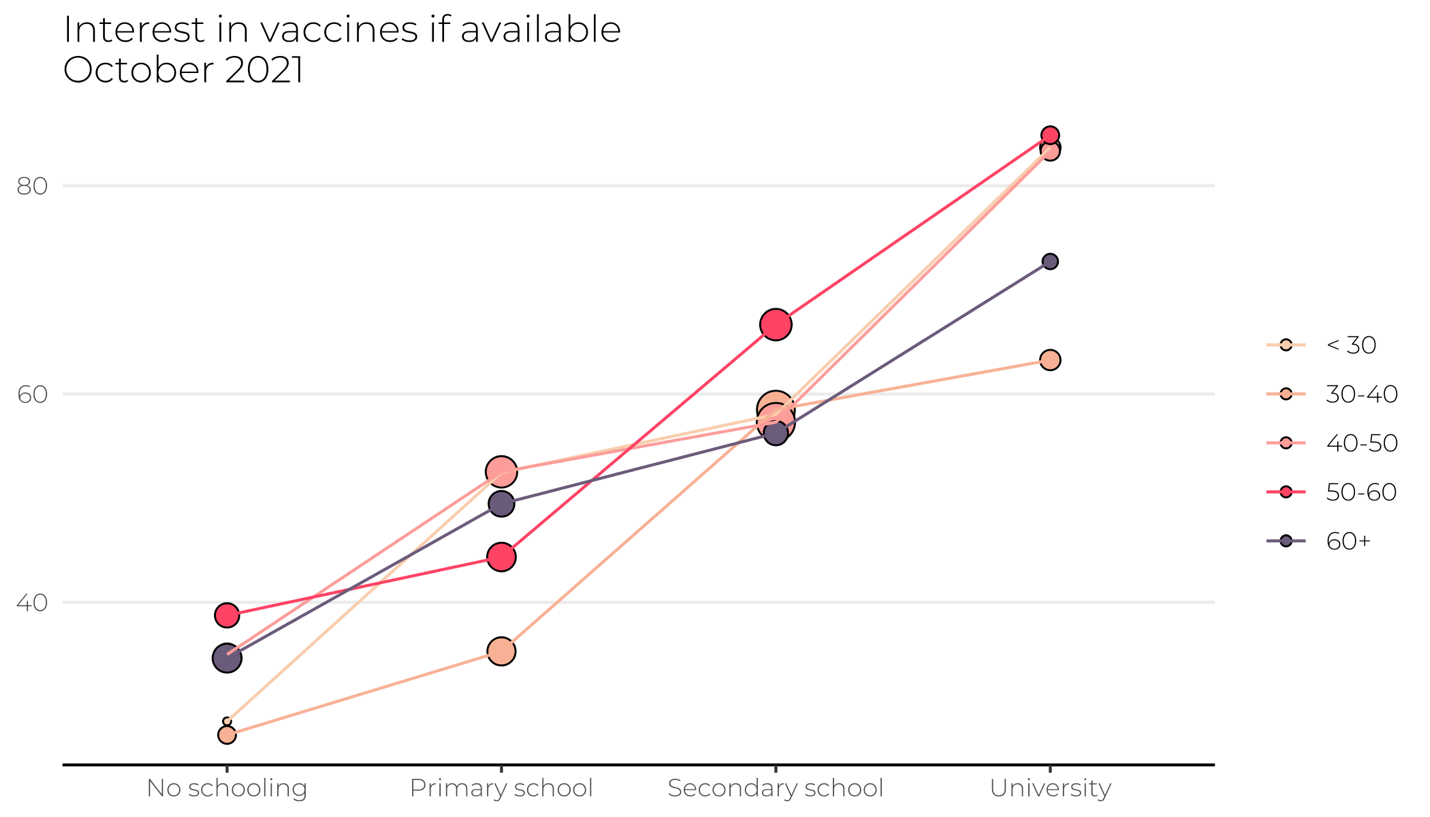
To get a better grip on whether these differential rates of vaccination reflect access or interest, in Figure 2, we also look at the share of respondents in each subgroup who expressed interest in getting a vaccine if offered. Here, we see the same trends observed in which respondents are getting vaccinated. A full 88.8% of university graduates, for instance, expressed an interest in getting vaccinated in October 2021 if it was made available—approximately twice as high as the percentage of respondents with no formal schooling (44.5%). Worryingly, the largest upticks in vaccination interest between March and October 2021 were among those who were, from the outset, more interest in getting vaccinated. Among individuals who make more than 4m IDR/month, interest in getting vaccinated increase by 51% over the seven months, compared to an 19.2% uptick in interest among individuals who make less than 1m IDR a month.
Why don’t some people want the vaccine in Indonesia?
What explains the lack of interest in getting vaccinated on the part of those respondents who indicated no intention of seeking out the jab? Recent accounts have placed considerable weight on the role of misinformation that has been circulating on social media. Looking at ten countries across the Global South, a team of researchers found widespread evidence of vaccine hesitancy motivated in part by false information held by respondents about the vaccines. Indonesia is no different: rumors have swirled on social media that the Chinese Sinovac vaccine is not halal, despite official statements to the contrary.
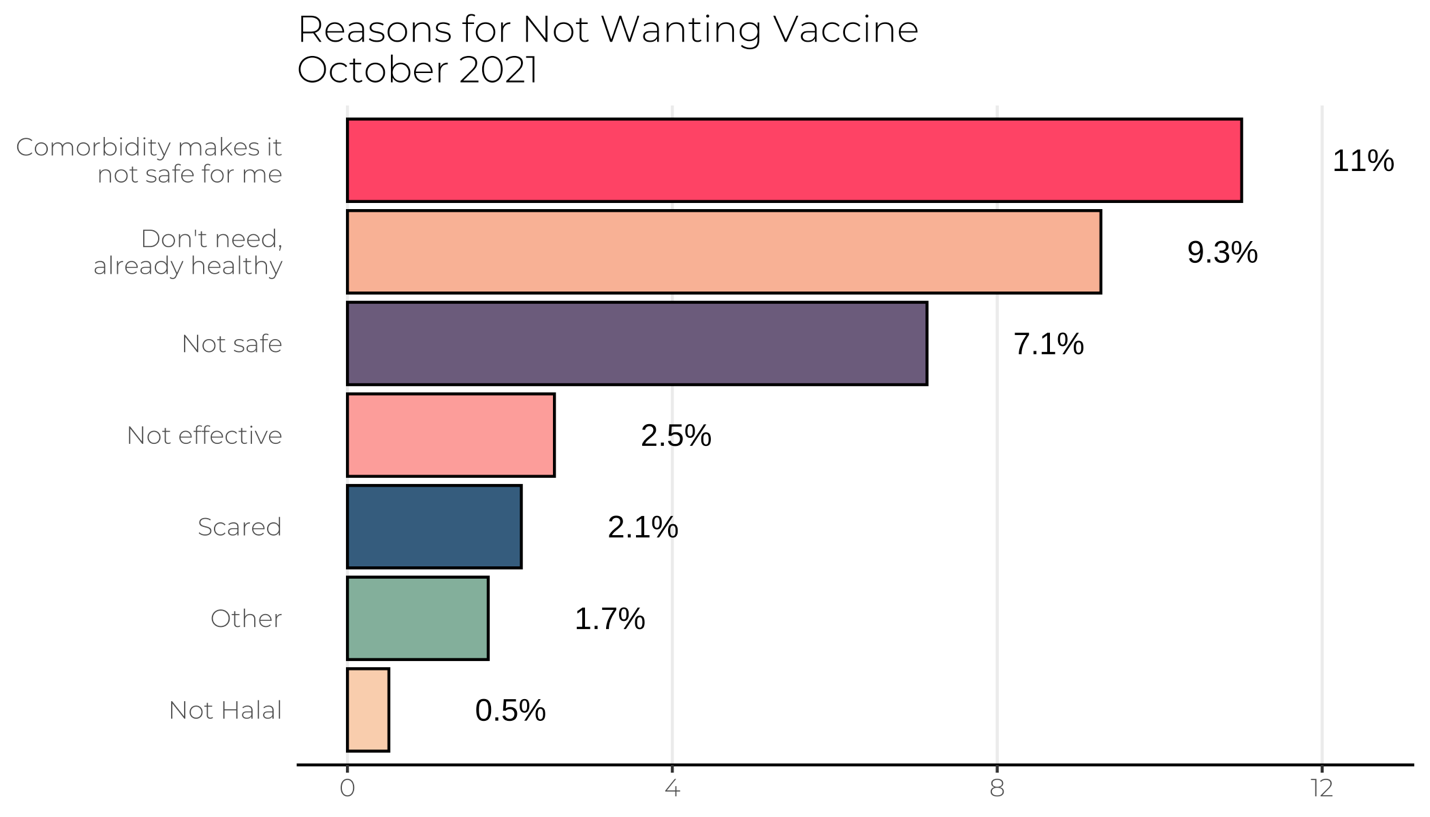
We therefore quizzed respondents who indicated no interest in getting vaccinated about their reason for opting against the jab. Respondents were able to choose from one of several reasons. In Figure 3, we show the percentage of the population indicating any one of the reasons listed. First, we find little evidence that a concern over vaccines not being halal is driving vaccine hesitancy: only 0.5% of respondents in our sample indicated this reason. Instead, the most common reason cited for not having an interest in getting vaccinated is respondents stating that their underlying comorbidity’s make vaccination unsafe—a concern likely motivated by concerns over side effects of the jab. In one sense, this is a line of misinformation that should be easily targeted with educational campaigns—as compared with more malevolent forms of misinformation regarding the providence and intention of vaccines.
Finally, we consider why it might be the case that older respondents indicate the lowest interest in vaccination in Indonesia. This is particularly puzzling: it is well documented that the older individuals are at greater risk of severe illness if infected with COVID-19. In theory, risk ought to be an important motivator to seek out vaccination. Indeed, it is precisely this tendency that has undermined the vaccine rollout in the United States, where many young people have opted to not get vaccinated, wagering that they are at lower risk to experience serious illness in the event they contract COVID-19.
We examine the possibility that Indonesia’s geriatric bias in vaccination reflects the tendency for young people to be, on average, more educated than their seniors. It is well-documented that access to education has expanded over the past half century in Indonesia, and it may be that this expanded access has led to greater confidence and literacy in the recommendations of medical and scientific experts.
Indeed, consistent with this expectation, we find that education is the strongest predictor of interest in vaccination—above and beyond the role of age. Individuals who obtained at least a university degree—including those older than 60—are significantly more likely to express a desire to receive the jab than their less educated peers.
These findings provide important cues for policymakers looking to boost the overall rate of vaccination in Indonesia: for one, concerns over misinformation suggesting that vaccines are not halal appear to be overstated, and health authorities should instead focus their attention on remedying the notion that vaccine side effects are more dangerous than COVID-19 itself. Of course, this analysis is also subject to certain limitations. For one, the data are collected from a specific temporal point in the pandemic and vaccine rollout. Although we anticipate that many of the trends continue to hold, our research attests to the importance of conducting routine studies of the sources of vaccine inequity in Indonesia
New Zealanders in Australia will be able to return home by the end of the month under a five-stage reopening plan announced by the government today.
The first stages of the plan would see returning vaccinated New Zealanders able to go into self-isolation and taking a test on arrival, rather than going into managed isolation and quarantine (MIQ).
Prime Minister Jacinda Ardern revealed the plan in a speech to Business New Zealand this morning, in which she defended the government’s use of MIQ and pledged there would be “life after covid”.
“It’s easy to hear the word MIQ and immediately associate it with heartache. There is no question that for New Zealand it has been one of the hardest parts of the pandemic,” she said.
“But the choice to use it undeniably saved lives … MIQ meant not everyone could come home when they wanted to but it also meant that covid could not come in when it wanted to, either.”
The five stages:
11.59pm 27 February: Self-isolation opens for New Zealanders and eligible travellers coming from Australia
11.59pm 13 March: Open to New Zealanders and eligible travellers from the rest of the world; skilled workers earning at least 1.5x median wage; working holiday visas
11.59pm 12 April: Offshore temporary visa holders who still meet visa requirements; 5000 international students; consideration of further class exemptions for critical workforces that do not meet the 1.5x median wage test
By July: Anyone from Australia; visa-waiver travel; a new Accredited Employer Work Visa opens and skilled worker exemption is phased out
In October: Border reopens to the rest of the world, all visa categories fully reopen
Unvaccinated travellers would still go into MIQ, but with less demand the Defence Force would begin withdrawing and some facilities would return to being hotels. A core quarantine capacity would be maintained and scaled up, to become a National Quarantine Service.
Self-isolation period
The self-isolation period for returning travellers would match that for close contacts under the government’s phased approach to Omicron: 10 days under phase one, seven days under phase two and three.
Today’s media briefing at Business New Zealand. Video: RNZ News
All arrivals will be given three rapid antigen tests, returning results on day 0/1 and on day 5/6, with one extra test. Positive results will be confirmed with a PCR test.
Ardern said the tools used to help battle the health crisis had not stayed the same, and while some may feel anxious about the reopening plan, the isolation, testing and high vaccination rates would help keep the virus from spreading too quickly.
Ardern said the government would be continually monitoring the value of self-isolation, and it was possible it may not be needed in the “not too distant future”.
She also confirmed she would lead trade delegations this year to Australia, Asia, the United States and Europe.
“New Zealand is in demand.” … How the New Zealand Herald reported the border opening policy today before the formal announcement. Image: APR screenshot
‘New Zealand is in demand’
“New Zealand is in demand. Our exports are at record highs, people want to live and work here, international students want to study here, our friends and whānau want to return,” she said.
“Covid laid bare our unsustainable reliance on temporary migrant labour. Immigration will continue to be a part of our economic story, but we have the opportunity now to build resilience into our workforces while also attracting the skills and talent we need.
“We have a chance to do things differently.”
“I hear much talk of a return to business as usual but we are better than business as usual … we must now carve our own recovery. On our terms.”
“We are vaccinated, increasingly boosted, and continue to prepare ourselves at home and work with a plan – and so now it is time to move forward together, safely.”
The critical worker border exemptions under Step 1 of the border reopening would cover:
Critical health workers
Dairy farm managers and assistants
Shearers and wool handlers
Deepwater fishing crew
Rural contractors
Veterinarians
Teachers
International students
Major infrastructure projects
Tech sector workers
External auditors
Government-approved events and programmes
Other short- and long-term ‘critical workers’
147 new community cases – 13 in hospital
The Ministry of Health reported today there were 147 new cases of covid-19 in the community and 44 at the border. Omicron is already the dominant strain.
In a statement, the ministry said the new community cases were in Northland (14), Auckland (90), Waikato (15), Rotorua (8), Taupō (1), Bay of Plenty (8), Hawke’s Bay (7) and Wellington (4).
A person admitted to Wellington Hospital has tested positive for covid-19, Capital and Coast DHB confirmed this morning. The ministry said there were another 12 people in hospital in Auckland, Rotorua and Hawke’s Bay.
There are no people in intensive care.
This article is republished under a community partnership agreement with RNZ.
Three new covid-19 cases have been confirmed in the kingdom of Tonga bringing the total number to five as the country went into a five-day lockdown.
In a press conference in Nuku’alofa yesterday afternoon, Tonga’s Prime Minister Hu’akavameiliku said that a woman and her two children had tested positive for the virus.
The two men were port workers and are currently now confined in isolation at Taliai Camp, a Tongan military base.
The pair had been collecting emergency supplies from foreign aid ships arriving in Tonga and were among 50 frontline workers who had been tested for the virus.
The prime minister did not reveal which ships the men had collected supplies from, leaving the source of the transmission open to speculation.
Nuku’alofa harbour is reportedly full of supply ships laden with aid, including the Australian ship HMAS Adelaide, which had confirmed before arriving in Tonga that 29 of its crew were in isolation on board after testing positive for covid-19.
Source of virus unclear
Tonga’s Parliamentary Speaker, Lord Fakafanua, told RNZ Pacific today that it was not clear how the two men contracted the virus.
Tongan Prime Minister Hu’akavameiliku … Image: Koro Vaka’uta/RNZ Pacific
He said that the covid-19 outbreak could not have happened at a worse time with covid-19 restrictions interfering with much needed aid deliveries.
The kingdom is still in the early stages of recovery from the devastating Hunga Tonga-Hunga Ha’apai volcanic eruption and tsunami, that left hundreds of Tongans homeless and properties damaged last month.
“The Prime Minister has reassured me this morning that the aid that is currently being distributed in Tonga will continue, the work that His Majesty’s Armed Forces is doing on the ground will continue under the lockdown because they are an essential service,” Lord Fakafanua said.
Tonga’s Speaker Lord Fakafanua … “The aid that is currently being distributed in Tonga will continue.” Image: Koro Vaka’uta/RNZ Pacific
The country is polluted with volcanic ash that has fouled water supplies and carpeted the land with dust.
Two weeks after the disaster, telecommunications are yet to be re-established in most of Tonga, with no outsiders being able to make mobile or phone calls into the Vava’u and Ha’apai group of islands.
Lord Fakafanua also said there were worries about a potential covid-19 outbreak in Vava’u, as a close contact of one of the new covid-19 cases in Tonga had visited Vava’u over the week.
Contact tracing stepped up
The government has stepped up contact tracing measures in order to ring fence community transmission of covid-19.
Lockdown rules in Tonga will require everyone to remain at home, to practise social distancing, and to wear face masks in public.
Essential workers are exempted from restrictions of movement, such as Red Cross and aid distribution personnel, who would be allowed to operate freely.
According to Tonga’s Ministry of Health, more than 83 percent of the population of the eligible population (over the age of 12) have been fully vaccinated.
Exactly 73,938 people (over the age of 12) have been vaccinated at least once, representing 96 percent of those eligible for testing.
The Tongan government said at last night’s press conference that the lockdown would be reassessed 48 hours after its enforcement.
This article is republished under a community partnership agreement with RNZ.
New Zealand is shortening the gap between second and third doses of the covid-19 vaccine from four months to three, the government has announced.
Prime Minister Jacinda Ardern, Covid-19 Response Minister Chris Hipkins and Director-General of Health Dr Ashley Bloomfield made the announcement this afternoon.
Ardern said Cabinet made the decision on the advice of the Vaccine Technical Advisory Group, and it would mean a million more New Zealanders would be eligible for their booster shot.
The shorter interval, which only applies to the Pfizer vaccine, will take effect on Friday, February 4.
“It now means a total of 3,063,823 people aged 18 and over — two thirds of our population — will be eligible for their booster from this weekend. Over 1.3 million people have already got theirs,” Hipkins said.
The change would mean more people, especially Māori, would be able to receive a booster before omicron took hold, he said, urging anyone who was eligible to get their booster as soon as possible.
Ardern said an extra 100,000 Māori will be eligible for a booster, representing a 59 percent increase in Māori eligibility from Friday, while an additional 52,000 Pacific people will be eligible, representing a 47 percent increase.
Ardern said the reason for getting the booster was clear — Omicron was usually more mild, but it could be severe for some.
“So don’t think getting a booster is just about keeping yourself safe, it’s about ensuring our hospital and health system is not overwhelmed so those you love and everyone in our community who needs our hospitals can get the care they need,” she said.
Watch the government announcement:
Today’s media conference.Video: RNZ News
Hipkins said New Zealand was one of the top-10 most vaccinated countries in the OECD, and the earlier booster would also help reduce the impacts of omicron on workforces and supply chains.
“We have given ourselves a head start that we cannot afford to give up,” he said.
People can check their eligibility on MyCovidRecord, by referring to their vaccine appointment card, or calling 0800 28 29 26 between 8am and 8pm seven days a week.
Ardern said today that 94 percent of New Zealanders over the age of 12 were fully vaccinated.
“A year ago, achieving that level of community immunity would have been considered incredibly ambitious, but the overwhelming majority of the team of five million have done what they’ve done best this entire pandemic, banded together and turned out to get vaccinated not just for themselves but to keep their loved ones and communities safe.”
The high rates had helped stop a delta outbreak and given New Zealand a head start against omicron, but now the number boosted needed to get as high as possible, she said.
The government would create a big booster campaign during February, with details to be provided by the Ministry of Health next week, Ardern said.
Significant boost in funding
Dr Bloomfield acknowledged the work put in by vaccination teams across the country in achieving 94 percent vaccination. Māori vaccination rates were now up to 90 percent first dose and 85 percent second dose, he said.
Ardern said there had been a significant boost in funding for community organisations which was helping support the efforts to help vaccinate Māori around the country.
“What we’ve had to do is make sure that we’ve stood up a system that worked for delta, now we need to make sure that we are able to expand to deal with what will be a larger number of cases but actually the majority of cases won’t need the level of care that delta may have required. So that has been an ongoing programme of work with our Māori providers,” she said.
Dr Bloomfield said the impact of waning protection over time from the vaccine had been seen.
“The good news is that there is clear evidence with that booster dose of the Pfizer vaccine, that people’s protection goes back up to a similar level to what it was for delta with two doses, and that is well over 90 percent protection against hospitalisation or serious illness.”
He urged everyone to make a plan, and said there was excellent capacity for vaccinations across the system.
“While we can’t administer boosters to everyone in that one million this Friday, I can assure you we have excellent capacity across our system and we certainly have a good supply of vaccine.”
Important for vulnerable people
It was even more important for vulnerable people and those working in higher-risk settings to get the booster, and considerable work was under way to make boosters as available as possible to those people, Dr Bloomfield said.
New Zealand data so far was similar to that overseas — we had not seen an increase in side effects, and overall adverse events after each additional vaccination had declined, he said.
He had asked for advice on when 12 to 17-year-olds would be able to get booster doses.
Ardern said the reason behind the delay until Friday was the government needed to make sure all the infrastructure was stood up.
New Zealand was still relatively early on in its omicron outbreak compared to other countries, and there was still time for people to get their booster in the coming week and have the benefit of it before the variant spread widely, she said.
Dr Bloomfield said New Zealand was an early mover in reducing the booster interval from six months to four, and was moving to reduce the interval again to three months before the omicron outbreak, which was something many other countries did not have the opportunity to do.
Ministry of Health Chief Science Adviser Ian Town said bringing it forward to three months, which had been done in the UK and in many Australian states, meant New Zealand could get the level of antibodies at a peak before it was facing widespread transmission.
No downside
There did not appear to be any downside to reducing the interval to three months, he said.
Dr Bloomfield said he wanted to emphasise that the evidence was clear that while two doses was great for delta, that was not the case with omicron, “so we will be pushing really hard to vaccinate”.
This morning, Deputy Prime Minister Grant Robertson defended the government’s approach to pregnant journalist Charlotte Bellis’ emergency MIQ requests, and its acquisition of rapid antigen tests (RATs) ahead of an expected rapid increase in Omicron variant cases across New Zealand.
Cabinet yesterday discussed its plans for reopening the borders, and Prime Minister Ardern is expected to make announcements about that tomorrow. A staged timeline was outlined late last year, but was quickly delayed because of the risks posed by omicron.
The government this morning announced it would adding $70.7 million to its Events Support Scheme, and extending coverage to events scheduled for before 31 January next year that were planned before being cancelled by the red traffic light setting.
This article is republished under a community partnership agreement with RNZ.
Within a month of the first community exposure to omicron in Aotearoa New Zealand, the variant has already become the dominant strain of covid-19.
We are yet to see the rapid and steep rise in new omicron cases that has been predicted. This could be because of asymptomatic transmission, but it is equally likely because public health measures included in the first phase of the “stamp it out strategy” have been effective.
For now, managed isolation and quarantine (MIQ) at the border is successfully stopping hundreds of cases from entering the community.
The best way forward is to limit widespread transmission for as long as possible. This reduces opportunities for the virus to replicate, which is when mutations occur, potentially extending the pandemic.
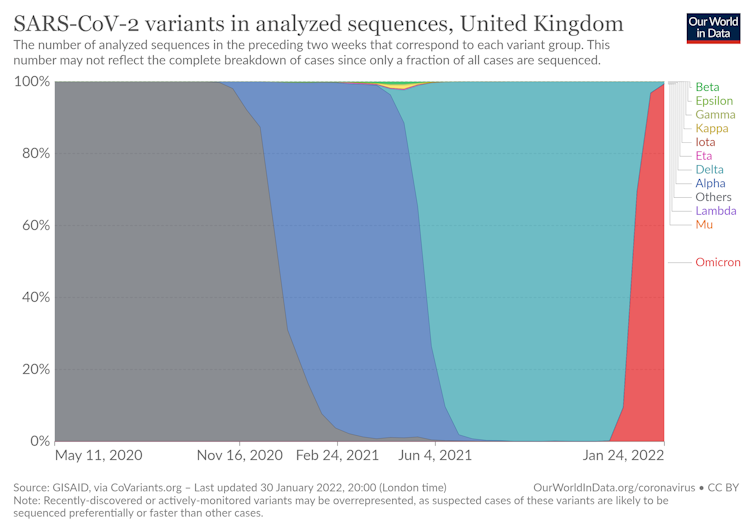
As shown below, omicron quickly replaces earlier variants.
The graph shows the rise of Omicron (red) in the UK, displacing earlier covid-19 variants. Our World in Data, GISAID, CC BY-ND
Omicron’s transmission advantage is thought to be due to its ability to evade immunity (acquired through infection or vaccination) and quickly infect the upper respiratory tract.
The risk of reinfection also appears higher than for delta, particularly in the unvaccinated and those with lower viral loads during previous infections.
Symptoms to watch out for Omicron symptoms include a runny nose, headache, fatigue, sneezing and a sore throat.
However, New Zealand’s high vaccination rates mean some people may not have any symptoms at all. The danger here is that they will still be able to pass on the virus to others, unaware they have omicron.
Given a choice, would you rather enter a room with Delta or Omicron?
Modeller, Professor @MichaelPlankNZ uses this scenario to explain differences between the #Covid-19 variants, while UC Health’s Dr @hobbs_PA reminds us Omicron isn’t ‘mild’. @UCNZMathshttps://t.co/4dgnOSZUJC
It is best to assume that any symptoms, especially a sore throat, are covid-19 until proven otherwise through a test.
For omicron, this may require saliva swab tests as recent evidence suggests they are more sensitive than nasal swabs because the viral load peaks earlier in saliva than nasal mucus.
Compared to delta, omicron has caused lower hospitalisation and death rates in many countries. This may be because it reproduces in the upper respiratory tract instead of the lungs.
Omicron is also meeting populations with immunity acquired through previous infection or vaccination.
Vaccination is especially important in New Zealand as we have had minimal prior exposure to covid-19 in the community.
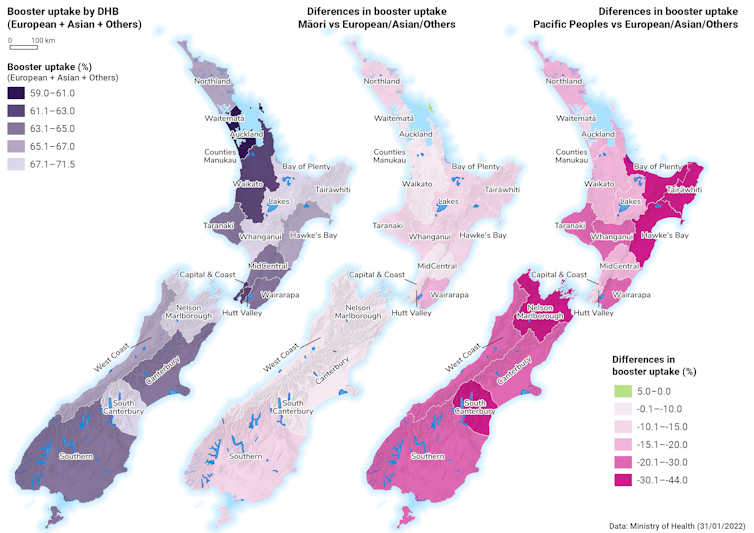
This graph shows the geographical and ethnic difference in the uptake of booster vaccinations. Author provided, CC BY-ND
Where to from here
Omicron is a “double-edged sword”. It is vastly more transmissible but less severe. However, it is not a mild infection and there is no guarantee the next variant will be less severe.
This should still be true even now (with the right measures)
The kicker is that with omicron, lots of HCW sickness will drop the capacity line lower. This will be much more pronounced for the fast red surge than the slow blue wave so in fact the red surge is worse than modelled pic.twitter.com/5hfk4uSMCt
Healthcare workers are already over-burdened and exhausted from previous outbreaks, which have distracted from other services and exacerbated entrenched inequities.
There are several things each of us can do:
Anybody eligible should prioritise getting boosted
we should all continue using the COVID-19 tracer app
we should keep indoor spaces well ventilated by opening windows and doors
mask wearing remains important, especially where physical distancing is difficult.
and anybody who feels unwell, should get tested and isolate.
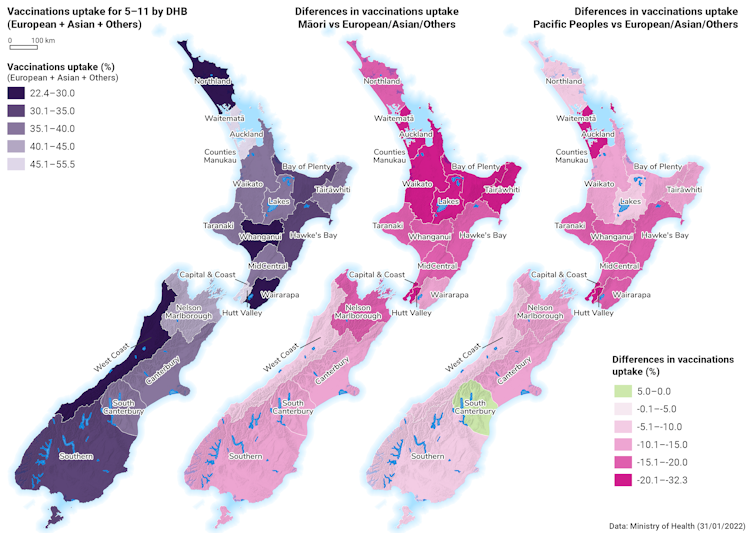
Data out of Australia indicate children aged five to 11 tolerated the vaccine well, with fewer side effects than adults.
Unfortunately, our analysis, along with other evidence, documents a concerning trend with lower childhood vaccination rates for Māori and Pasifika, as well as large variation between regions.
This graph shows the geographical and ethnic difference in the uptake of childhood (five-11-year-olds) vaccinations. Image: Author provided, CC BY-ND
This is concerning as some countries, including the US, have seen increases in childhood hospitalisation rates for covid-19. In the UK, one in eight pupils have missed school as covid-related absences rise.
The success story of the delta outbreak Unfortunately, there’s been little time to celebrate the rather remarkable demise of delta. Even as Auckland opened up, hospitalisations and case numbers dropped.
Summer will have helped as people spent more time outdoors. However, public health measures such as border closures, managed isolation and quarantine and contact tracing have no doubt helped stamp out much of delta, allowing a relatively normal summer holiday period for many.
Continuing to keep delta low also means we should not have to deal with a “double epidemic”.
This success may also fill us with some hope that, just perhaps, we might be able to avoid the worst of omicron during this next phase of the pandemic response, with robust and continually refined public health measures in place.
The kingdom of Tonga will go into nationwide lockdown from 6pm tonight.
Speaking via Tongan radio, Prime Minister Hu’akavameiliku Siaosi Sovaleni and Minister of Health Dr Saia Piukala held a media conference last night to announce the news.
They confirmed that two cases of covid-19 had been detected through routine testing at the wharf in Nuku’alofa.
Prime Minister Hu’akavameiliku ordered the lockdown.
Dr Saia Piukala said 50 people were tested as part of routine surveillance and the two positive cases were found.
Tonga’s Speaker of the House, Lord Fakafanua — who is currently in Auckland waiting to return to Tonga — told RNZ Pacific the positive cases and their families were now in isolation at an army base.
Tonga reported its first positive covid case last year after an Air New Zealand flight arrived from Christchurch.
Recovering from volcano eruption
Tonga is currently recovering from the Hunga Tonga-Hunga Ha’apai volcano eruption on January 15 which triggered a tsunami that destroyed villages and resorts and knocked out communications for the nation of about 105,000 people.
Three people died as a result of the disaster.
Several countries, including New Zealand, have sent aid but have observed strict covid-19 protocols such as contactless delivery.
According to media reports, more than 300 nurses are leaving their jobs citing poor employment conditions including suffering from stress, fatigue and lack of compensation.
Fiji Women’s Crisis Centre coordinator Shamima Ali said those who were resigning amid the covid-19 crisis were not speaking out because they feared victimisation by the health ministry and the government.
The latest figures have pushed the number of cases since the September 2021 delta outbreak to more than 20,000 with 21 people in hospital, including one in intensive care.
The seven-day average has neared 500 cases after being under 20 a month ago.
The virus has spread to all three provinces and most communes.
This article is republished under a community partnership agreement with RNZ.
South Seas Healthcare Trust chief executive Lemalu Silao Vaisola says people are tired of covid-19 rather than complacent after two years of the pandemic.
He said he had seen fatigue set in which could explain the low uptake of the booster shot in the Pacific community.
“People are just covid-fatigued where everything is all about self-isolation, traffic lights and the lockdowns.
“I think it is just fatigue, people are just tired. So I don’t know if it is complacency, but it’s been ongoing and two years is a long time to go through changes.”
Lemalu said the South Seas Healthcare team were preparing now for omicron to hit communities just like they had done in the past two years of covid-19.
He said the team intended to use the Manukau Insititute of Technology campus for a booster vaccination drive to get rates up.
“We’ve still got the MIT sites that’s during vaccinations and we’ve got a drive through vaccination for increasing the boosters and five to 11 [year olds] and on top of that we’ve been training our staff in terms of outreach into the homes.”
Front and centre
Lemalu said his organisation was front and centre fighting the delta strain and the experience stood them in good stead.
“We’ve got a good template to respond, but again every variant so far provides its own set of challenges,” he said.
“I’m happy that we’ve sort of almost had two years experience that will position us to hopefully be ready for this, but like I said before it’s different from what we are seeing overseas.
“We plan for the worst and hope for the best.”
He is encouraging Pacific families to get a booster shot.
This article is republished under a community partnership agreement with RNZ.
This month, the Biden administration launched aprogramto deliver four COVID-19 rapid tests per household to people with an address across the country. While the program will deliver 500 million tests, advocates say it innately disadvantages houseless people, multigenerational households, and those who live in apartment buildings that may be subject toa glitch in the systemthat only allows one set per building. Ultimately, the program is most helpful for those who fulfill the traditional American nuclear family, leaving out the populations most at risk of contracting the virus because of their inability to afford living on their own. The demand for testing comes when community spread is rampant, and the country is stillaveragingclose to 700,000 new cases a day. The Biden administration’s first direct testing response leaves a lot to be desired two years into the pandemic.
“There’s clearly a very myopic view of how to handle this rollout, which has consistently been a problem this entire pandemic,” said Dr. Imani E. McElroy, a physician at Massachusetts General Hospital. “[The rollout] directly benefits those who have the privilege of high-quality access.”
McElroy lives in an apartment building in East Boston with about six units in a neighborhood with aLatinx populationof 52.9%, which she says has been severely impacted by COVID-19. Soon after the program was announced, she read that people who lived in apartment complexes could not order their quota if someone else in the building had already placed an order. She has held off on ordering her own until she confirms that her neighbors, including a multi-generational family, can apply for their tests. As a physician, she has access to COVID-19 tests through her department.
“I didn’t want to affect their ability to get their test,” McElroy said.
According toGenerations United, an estimated 66.7 million adults, or one in four people in the U.S., live in a multigenerational household. While some live in multigenerational households for cultural reasons, many people have been forced into them because of the rising cost of living across the nation. In October last year, theFederal Register reportedthat the cost of living for 2022 would increase 5.9%. InBoston, where McElroy lives, the cost of living is 51% higher than the national average. In a 2016Pew Research study, Black, Latinx, and Asian families were more likely to live in multigenerational households than white families. For these households, quarantining and self-isolating during a pandemic is much more precarious than usual. According to apublic health studyon multigenerational households in New York City, overcrowded homes and multigenerational housing are independent risk factors for COVID-19.
“The largest affected populations by COVID have been populations that can’t afford to live on their own and can’t self-quarantine,” McElroy said. “You’re getting rapid transmission throughout these communities.”
McElroy suggests that the federal government use census data to send more tests to households that may need more, and have an efficient way of requesting more tests as required. She also suggested having the option to send them to a P.O. box if needed. The U.S. Postal Service has not responded to a request for more information on any future distribution programs.
“There has to be a way to petition to be able to get more tests,” McElroy said. “There’s a lot of stopgaps that could have been used to prevent the issues that we’re consistently seeing in this response.”
Houseless people, who do not have a permanent address to include on the form, have also been left out of the current program.Referred to as “the invisible victims”of COVID-19, few resources keep track of the number of infections and deaths among the houseless community.
Even if houseless people were to have access to at-home rapid tests, David Peery, the founder of Miami Coalition to Advance Racial Equality, says it would be difficult to keep them in their possession. Many houseless people who live in encampments are subject to frequent street sweepings that trash and destroy all of their possessions.
“[The government] can give out a testing kit on a Monday, and the City can come and do a sweep the very next day and destroy everything and throw all your stuff away,” Peery said. “It’s very hard to keep possessions when you don’t have a home.”
According to Peery, a more comprehensive solution would be to expand non-congregated emergency shelters by contracting and renting hotel and motel rooms. He says that more private rooms used in cities across the country since the start of the pandemic for isolation purposes,including Atlanta, should be expanded as emergency shelter alternatives as opposed to the traditional emergency congregate shelters that pack people into a dorm room. Apublic health studysupports Peery’s idea, suggesting that isolation hotels help mitigate the spread of Covid-19 among houseless populations.
“Non-congregate settings have proven to be much more effective in getting people off the streets. Now you have a roof over your head, you have a door you can lock, and you can store your possessions, including these at-home testing kits,” Peery said. “They’ll also be protected from infections and it will provide a path to permanent housing.”
Before the government launches another program to distribute tests or personal protective equipment, people across the country say considerations should be made to reach the communities most vulnerable with the least amount of access to these mitigating measures.
Prismis an independent and nonprofit newsroom led by journalists of color. We report from the ground up and at the intersections of injustice.
Omicron has ripped through the Australian states of New South Wales and Victoria, exposing testing regimes, decimating supply chains and causing the country’s deadliest days of the pandemic despite high vaccination rates.
So is that New Zealand’s fate as well?
RNZ News spoke to a trio of experts in Australia who say Aotearoa can and should do better.
When omicron arrived in Australia in late November, governments followed through on plans to relax restrictions.
University of Sydney epidemiologist Professor Alexandra Martiniuk said that was the first mistake.
“If we had gone a bit lower and slower on our curve we would’ve put the pressure on our systems over a longer period of time — yes, but it would’ve been slower so we probably would’ve experienced less of the crises we did experience and importantly, this is hypothetical I suppose, more people might have been saved.”
As the pressure built on the health system due to the number of cases, it affected the quality of care across the system.
It also removed vast numbers out of the workforce as they isolated awaiting test results or from infection itself.
The key to suppressing the curve was:
getting vaccinated and a booster as soon as possible
wearing a quality mask
thinking about physical distancing and preferably meeting people outdoors
scanning in
getting tested and isolating if symptomatic.
New Zealand epidemiologist Professor Tony Blakely, from the University of Melbourne, agreed, saying the elderly and at-risk needed to exercise extra caution over the coming weeks and months.
University of Melbourne epidemiologist Professor Tony Blakely … Image: Billy Wong/University of Auckland
About half of New Zealand’s population was likely to contract omicron during the outbreak and that was okay, Professor Blakely said.
The key to minimising death and disruption was about who caught it and when.
“The two tricks are: having accepted that burden of infection coming through, to squash it and spread it out over time so it doesn’t overwhelm health services.
“And the second is to try to tip away the infections from the people who have the highest risk of morbidity and mortality. So people who have comorbidities, are immunocompromised, or who are elderly,” he said.
In essence, the pair believed New Zealand should look to prolong the outbreak, which might sound counter-intuitive, but a steady stream of cases over months was going to be better than a flood over weeks.
Much in the same way the tide coming in over six hours did not cause a problem, but a tsunami did.
Another thing on Aotearoa’s side was the rate of Delta.
Australia was still dealing with 1300 cases a day of the far deadlier variant when Omicron arrived.
Professor Blakely said as a result Australia had been fighting two epidemics.
“It’s utterly clear – omicron is less severe than delta. The vast majority of people who get omicron don’t even know they’ve had it – they’re asymptomatic.
“Yes there will be deaths – that’s unfortunate. But it’s a lot less than had it been delta with this amount of infectiousness.
“Data is patchy — but in New South Wales two-thirds of people in ICU were omicron, which means one-third were delta and probably half of all deaths two weeks ago in New South Wales were among people with delta.
“So what’s happened? Delta is perhaps only 2-5 percent of all infections out in the community but because it’s that much more serious at every step — converting you from asymptomatic to symptomatic, symptomatic to quite sick, quite sick to going to hospital, hospital to ICU, ICU to death — at every point along the way it means even though delta is a tiny proportion of infections out in the community it’s causing a reasonably large fraction of all the hospitalisations and deaths.”
So what does that mean for New Zealand? “The lesson here for New Zealand is keep delta squashed down,” Professor Blakely said.
As omicron spiralled in the community, contact tracing should focus on delta cases, he said.
He described the New Zealand government’s plan to deal with omicron, released earlier this week, as brilliant.
“I really like the way that they’ve laid out what’s going to happen and how close contacts are going to change, the number of days will get less as you go through before you can go back to work — it’s exactly like I would’ve designed it if I’d been asked to design it. It’s very good.”
However, a degree of flexibility was needed as the pandemic had shown it could throw a curveball even at the best-laid plans.
Stock up on supplies, meet loved ones Australasian Epidemiological Association president Associate Professor Brigid Lynch said it appeared omicron was potentially as severe as the wild variant identified in Wuhan in late 2019, but far more contagious.
However, unlike in early 2020, there were effective vaccines that drastically curbed serious illness and death.
Far more was also known about the virus’ transmission.
Disposable KN95 mask pictured above a surgical mask. Image: RNZ/123rf
To that end high-quality masks, especially inside, and quality ventilation could reduce transmission, Associate Professor Lynch said.
“Workplaces and settings like education and aged care, we really should have had good ventilation measures – HEPA filters and things that will improve the air quality. Those are things that will be important going forward over the next few years.”
A large and readily available supply of rapid antigen tests could also help in reducing transmission in high-risk or high-density settings, like schools, aged care and health facilities.
Professor Martiniuk said another thing for people to consider now ahead of widespread infection and while time was still on your side was to get ready at home.
Putting some pre-prepared meals into the freezer, stashing some electrolyte drinks and having enough paracetamol and ibuprofen for a week might make the difference between a testing or a terrible time at home with the virus — especially if people had children to care for and consider as well.
Now was also the time to do some last-minute things for self-care, she said.
“It’s silly but it’s actually quite useful, but now is the time to go get your haircut, to go see your loved ones in aged care residences, to get your kids together with their friends – still outdoors preferably, to get a doctor’s appointment for your chronic illness that might need a prescription refill.
“Get it all done as if you’re going on a big vacation because in a month or two if cases are very high, those are the kind of things you won’t want to be doing.”
But all three epidemiologists agreed – while omicron was already here, New Zealand did not need to suffer its worst effects.
This article is republished under a community partnership agreement with RNZ.
We’ve been hearing a lot about masks this week, fabric, medical and N95. They’ve all got different layers of permeability.
Three more children have died from covid-19 in Fiji, taking the death toll since the pandemic hit the country in 2020 to 791.
The Fiji government also confirmed on Wednesday that a 10-day-old infant, 8-year-old girl and 13-year-old boy are among 12 covid-19 patients who have died.
There are 223 new cases in the community, with a total of 1980 patients in isolation.
Health Secretary Dr James Fong said all three children were from the Northern Division.
He said the baby had died at home before she could be taken to hospital.
He said the eight-year-old had a significant congenital medical condition that likely contributed to her death.
“The 13-year-old male was admitted for nine days at Nabouwalu Hospital in Bua before he passed away,” Dr Fong said.
“He had a significant congenital medical condition, and an assessment made by medical consultants confirmed that his pre-existing conditions contributed to his death. He was not vaccinated.”
Four-day intervals Dr Fong said that due to the time required by clinical teams to investigate, classify and report deaths, a four-day interval is given to calculate the seven days rolling average of deaths, “based on the date of death, to help ensure the data collected is complete before the average is reported”.
“Therefore, as of January 20 the national 7-day rolling average for covid-19 deaths per day is 4.1, with a case fatality rate of 1.32 percent.”
Dr Fong said there were 155 covid-19 patients in hospital.
The Health Ministry also recorded nine more covid-19 deaths between January 8-22.
Latest deaths
* A 70-year-old man from the Northern Division died at home on January 14. He was not vaccinated.
* A 98-year-old woman from the Western Division died on arrival at Lautoka Hospital on January 16. She was fully vaccinated.
* An 81-year-old woman, also from the west, died at home on January 16. She was fully vaccinated.
* A 74-year-old man from the west died on arrival at Tavua Hospital on January 18. He had pre-existing medical conditions and was not vaccinated.
* A 75-year-old woman from the west died at home on January 20. She was fully vaccinated.
* A 72-year-old woman from the Central Division had died at home on January 21. She had pre-existing medical conditions and was fully vaccinated.
* A 46-year-old woman from the Western Division died at home. She was not vaccinated.
* A 78-year-old man from the Eastern Division died at home on January 21. He was fully vaccinated.
* A 79-year-old man from the Central Division had died on arrival at the Colonial War Memorial Hospital in Suva on January 22. He was fully vaccinated.
This article is republished under a community partnership agreement with RNZ.
From the federal mask recommendations suspended in May to White House COVID coordinator Jeffrey Zients’s December pronouncement that the unvaccinated are to blame for “the hospitals you may soon overwhelm,” the Biden administration has organized its COVID response around an ethos of personal responsibility.
COVID is spun as a pandemic of the unvaccinated even as the vaccinated can also spread the virus. Vaccines and their boosters, importantly protecting the vaccinated from hospitalization and death, appear nothing of the public health silver bullet they’ve been positioned to be, presently offering only 10 weeks’ protection against symptomatic infection with the now circulating Omicron variant.
Such a campaign against the unvaccinated represents both bad politics and bad public health.
Many of the unvaccinated aren’t ideologically motivated. Skepticism and hesitancy mark as much a failure of vaccine access, including the absence of a national door-to-door campaign to convince the 84 million Americans walking around without a single COVID shot to get vaccinated or to physically transport them to an appointment. Winning their trust is critical in controlling the outbreak stateside.
Other patients may refrain from vaccination even when it puts them in great personal danger. Jesse Rouse, photographed here in November suffering his second bout of COVID in Minneapolis, was reported to be unvaccinated at the time after he previously underwent a double lung transplant. Researchers have proposed that lung transplantees are especially vulnerable to respiratory infection and should be vaccinated for COVID.
Some people may refrain from vaccination for medical reasons – including confusion or conflicting information about how vaccination might interact with their health conditions or treatments.
Regardless of why particular people remain unvaccinated, thrusting culpability fully onto individuals is a harmful move. Like Ronald Reagan’s campaign against “welfare queens,” presuming public health problems emerge primarily from bad actors and individual decision-making obfuscates the systemic and structural roots of the failure of the U.S.’s response to the pandemic.
Much like Trump, the Biden administration appears repeatedly intent on turning the COVID page, no matter the state of the pandemic itself. The May mask recommendations, which stated that vaccinated people could stop wearing masks in most indoor spaces, were textbook on that account. The administration later ignored an October report from public health experts recommending free testing at a pace of 732 million tests per month in preparation for a holiday COVID surge:
The plan, in effect, was a blueprint for how to avoid what is happening at this very moment — endless lines of desperate Americans clamoring for tests in order to safeguard holiday gatherings, just as COVID-19 is exploding again.
Yesterday, President Biden told David Muir of ABC News, “I wish I had thought about ordering” 500 million at-home tests “two months ago.” But the proposal shared at the meeting in October, disclosed here for the first time, included a “Bold Plan for Impact” and a provision for “Every American Household to Receive Free Rapid Tests for the Holidays/New Year.”
Early in December, Biden spokesperson Jen Psaki scoffed at reporter Mara Liasson’s query about why the U.S. doesn’t just pay for home COVID tests for every American household like other countries do instead of making Americans submit for reimbursement from insurance companies that have routinely failed to pick up the bill. “How much is that going to cost?” Psaki asked.
Should a government that had voted $768 billion for the Pentagon, $24 billion more than Biden requested, just pay for COVID tests? Yes, April Wallace replied in the Washington Post. Yes, it should:
I am a dual citizen of the United States and Britain, now living in Edinburgh, Scotland, and I am able get rapid antigen tests anytime I want to, at no cost and with no hoops to jump through. I know that Americans pay more than $20 for a package of two tests — if they’re in stock. Here you can walk into your local pharmacy, and they will just hand you packs of seven tests at no charge. In my neighborhood I can also go to the local recreational center and collect packs of tests free for my family, or swing by a coronavirus testing center.
It turns out the reimbursement for home tests wasn’t to start until mid-January anyway:
The administration has already said that the plan will not provide retroactive reimbursement for tests that have already been purchased, which means that any tests you buy for the holidays will not be covered.
The Biden no-plan, expanded to a whole four rapid tests per household and three masks for each American, appeared to be phase one of a campaign of further eroding American expectations. As self-described “shitposter” @fingerblaster tweeted about what’s missing:
Wild that the most unhinged republican president in history sent us $2000 checks back when we had like 12k cases a day and now we have 300k cases a day and a dem president who’s like “lol not my problem go to work jack”
The more august New York Times reported on the end of monthly child benefits millions of Americans were depending on:
The end of the extra assistance for parents is the latest in a long line of benefits “cliffs” that Americans have encountered as pandemic aid programs have expired. The Paycheck Protection Program, which supported hundreds of thousands of small businesses, ended in March. Expanded unemployment benefits ended in September, and earlier in some states. The federal eviction moratorium expired last summer. The last round of stimulus payments landed in Americans’ bank accounts last spring.
These benefit programs, as modest as they were, saved thousands of Americans from COVID deaths.
A March 2021 FamiliesUSA report summarized research showing a third of COVID deaths were tied to the lack of health insurance. The effect was multiplicative: “Each 10% increase in the proportion of a county’s residents who lacked health insurance was associated with a 70% increase in COVID-19 cases and a 48% increase in COVID-19 deaths.”
Controlling for stay-at-home orders, school closures and mask mandates, another study, first posted November 2020, estimated that lifting eviction moratoriums state-to-state resulted in between 365,200 and 502,200 excess coronavirus cases and between 8,900 and 12,500 excess deaths.
Omicron’s Delta Strain
So, public health clearly extends beyond necessary prophylaxes into necessary social interventions. But if there was any doubt about which constituency the political class serves instead, in December, the Centers for Disease Control and Prevention (CDC) cut down its recommendation for quarantine upon COVID exposure from 10 days to five. The act was decidedly in response to pressure from employers, notoriously Delta Air Lines’ CEO Ed Bastian in a letter that Delta proudly posted.
The Delta letter summarized the scientific literature in favor of its request in two sentences. The science is in reality more nuanced, marked by a variety of definitional complications.
Omicron, like new variants before it, is almost certain to evolve out from underneath the vaccine effectiveness that Delta Airlines cites as, full-stop, protection enough. Permitting COVID variants to circulate on Delta planes or elsewhere increases the chances they can evolve enough to circumvent medical and non-pharmaceutical controls.
Other drawbacks refute such summary boosterism. Omicron is already associated with increased reinfection. The variant’s other impacts on clinical courses and epidemiology are likely to be geographically specific, depending on a variety of local factors, including pre-existing immunity and the state of non-pharmaceutical interventions. What works as an intervention under one set of conditions does not necessarily hold under all.
More meta, the speed at which new variants are being allowed to evolve is outpacing even the frantic pace of the research conducted. “Flattening the curve” extends beyond our hospitals to research efforts aimed at discovering how to better control COVID.
In other words, under a more infectious Omicron, a variety of interventions, one layered atop another, is necessary, rather than stripping them back to serve criteria pretending to be scientific.
This isn’t the first time the airline industry tried to bend basic COVID science to its financial advantage. JetBlue CEO and reopen proponent David Neeleman funded and helped coordinate a Stanford University study that whistleblower complaints showed used a testing kit that erred on the side of false positives. By these tests, the study concluded the COVID virus was more widespread in the public and therefore, given the underlying number of deaths in the study population, was less dangerous of a pathogen.
National Institute of Allergy and Infectious Diseases Director Anthony Fauci, proving Lysenko on the Potomac, ran interference for Delta and other employers in the face of the twists and turns obvious in the COVID literature. Fauci parroted Bastian’s arguments nearly to the letter:
There is the danger that there will be so many people who are being isolated who are asymptomatic for the full ten days, that you could have a major negative impact on our ability to keep society running. So the decision was made of saying let’s get that cut in half.
CDC Director Rochelle Walensky once fought back tears over the likelihood of COVID mass deaths. Now, like a meat plant manager thinking only of the bottom line, she defends sending people back to work still infectious:
There are a lot of studies [from other variants] that show the maximum transmissibility is in those first five days. And [with Omicron] we are about to face hundreds of thousands more cases a day, and it was becoming very, very clear from the health care system that we would have people who were [positive but] asymptomatic and not able to work, and that was a harbinger of what was going to come in all other essential functions of society.
In short, the combination of economic compulsion and traumatic bonding that sent millions of workers into unprotected workplaces the pandemic’s first two years now represents state policy. The denialism for which liberals punch down on Trumpists is the labor law of the land. It is now a key part of the administration’s public health campaign.
“I’m not letting COVID-19 take my shifts,” one recent CDC ad declared. “My job puts me at high risk for COVID-19 exposure. I got vaccinated because it’s better to be protected than to be out sick.”
Another CDC post shamelessly used the U.S.’s privatized health care system as a cudgel of class discipline: “Hospital stays can be expensive, but COVID-19 vaccines are free. Help protect yourself from being hospitalized with #COVID19 by getting vaccinated.”
In that spirit, Biden economic advisor Jared Bernstein waxed optimistic on the economy. The depletion of personal savings would drive low-paid workers back into the labor market during a pandemic, Bernstein cheered.
“We are intent,” Jeff Zients declared mid-December, “on not letting Omicron disrupt work and school for the vaccinated. You’ve done the right thing, and we will get through this.” The vaccinated are presented as pure enough of soul to get back to working the gears of the economic machine. The unvaccinated are cast, to appropriate Hillary Clinton’s characterization, as a basket of eschatological deplorables.
Zients, a Biden campaign donor, was the CEO of investment firm Cranemere and director of Obama’s National Economic Council before becoming COVID czar with no public health experience. His primary portfolio of priorities was always apparent.
The quarantine switcheroo follows CDC’s changing recommendations for school distancing from six feet to three, which it now pretends is the virus’s limit. In reality, even six feet isn’t enough for the airborne virus. But in changing it to three, CDC could legally accommodate efforts to stuff students back in brick-and-mortar schools without changing day-to-day public health precautions.
Keeping kids out of school can have terrible impacts on learning outcomes and emotional well-being. Keeping kids in school, potentially leading to the deaths of other students or teachers in school, and older adults back home, can incur a different kind of emotional damage. Both risks serve as more the reason for bringing the outbreak under control with a full-spectrum intervention.
The CDC’s position, sending students back to school without controlling the outbreak, is geared toward other aims. It’s about putting the economic cart before the epidemiological horse. The kids need to go to school so that the parents can go to work.
Comedian Roy Wood Jr: CDC just said you only need to quarantine if you on a ventilator. But if ya ventilator got wheels and a battery pack you gotta take yo ass to work.
Author Alexander Chee: If you have to deploy the military to support hospitals you may have spent your budget on the wrong part of the system given the challenges we actually face.
Designer Char: CDC okays pull-out method as “eh, good enough.”
The administration is too full of itself to see it is losing the country. Its caustic claims about “the science” aren’t supported by the science, further undercutting research as a trusted source of both state strategy and public response.
The original 10-day quarantine that the CDC changed was grounded in the evidence-based realities of the virus itself, specifically its incubation time, generation time and serial interval. At the same time, the 10 days aren’t a matter of essentialist measures of central tendency.
Against CDC Director Walensky’s characterization, it’s about the variation in patients’ infectious periods. Some patients exit out of their infectiousness early, in the five days Walensky cited. Others can be infectious much longer. No one knows who’s a late bloomer in transmission. As a matter of practical public health intervention, it’s an unknown.
A public health campaign must therefore institute mask and quarantine policies that cover for the late transmissions, so that they don’t serve as the means by which the outbreak rolls on — particularly as Omicron’s infectiousness approaches that of measles and a 100% attack rate can still result from even a small group of infectious people walking around.
Instead, we have slashed public assistance, shortened quarantines, offered no-to-little remote schooling, hired few community health workers, conducted little genomic sequencing of the virus, and let hospitals get overrun. The CDC gave in upon the subsequent furor around the shortened quarantine by adding only a recommendation — not a requirement — of a negative rapid antigen test before workers returned to work.
Beyond trying to circumvent the rancor of partisan criticism, why did Trump and Biden alike aim at pretending the pandemic away? Biden’s trajectory is illustrative that capitalist realism has a way of eating away at even good faith efforts at addressing existential threats.
In October 2020, candidate Biden put the failings of his opposition in perspective: “We’re eight months into this pandemic, and Donald Trump still doesn’t have a plan to get this virus under control. I do.”
“This crisis,” President-elect Biden added, “demands a robust and immediate federal response.”
A year later, President Biden pivoted: “There is no federal solution. This gets solved at a state level,” months after many state governors had lost or abandoned their emergency powers to impose mask mandates and shelter-at-home orders.
Other countries see federal jurisdiction differently, as if the very health of their ostensible constituencies has something to do with governance.
While the U.S. daily breaks record COVID caseloads, some other countries appear to be of another world. COVID long-hauler Ravi Veriah Jacques reported these January 2 caseloads from abroad:
New Zealand – 51
China – 191
Taiwan – 20
Japan – 477
Hong Kong – 18
China’s reactions are both broader and triggered more quickly, with the public health results to show for it. Xi’an, a metropolis of 13 million people in Shaanxi Province, underwent an arguably arduous lockdown upon the emergence of 175 COVID cases. Western media has played on the difficulties in obtaining food in the city over the 12 days’ quarantine, but not the campaigns to alleviate those problems.
Some may argue the Biden administration’s reaction is better late than never, but that’s not how controlling COVID’s lightning strikes works.
As epidemiologist Rodrick Wallace models, whatever the intervention, there’s nothing worse than dithering. Given the insidious nature of the virus, we are routinely six weeks too late if spikes in cases, rather than anticipatory planning, are the trigger. Repeated delays mark U.S. COVID planning — among them, the spread of the original wave out of coastal cities to the rest of the country in spring 2020 and the arrivals since of Delta and Omicron stateside.
Rapid Confusion Test
It happens that the mass at-home testing the Biden administration passed over in October, setting up a program several months too late, is itself already a failure. Big picture, like vaccination, it represents yet another technicist intervention that, while necessary, is also insufficient. It’s more of a grand gesture that detracts from the administration’s refusal to pursue multilevel systemic public health programming.
The specifics of such a rollout and the tests themselves also get in the way. It’s much more than a matter of rapid tests permitting an exit out of the shots for the deplorable unvaccinated, as the Biden administration feared. It’s also not merely a matter of doctors defending their testing territory, as rapid test proponents argued.
Among several intrinsic errors that biotech consultant Dale Harrison explores around the rapid tests, there is the difficulty of self-administering them:
One important note is that at-home antigen tests will give VERY poor results (both high false-positives and high false-negatives) if you are sloppy or misuse them.
These are complex molecular assays and the EXACT usage is critical. You MUST read and follow every single detail in the instructions to get a reliable outcome….
The difficulties extend beyond administering the tests. Interpreting them is a difficult task; it is swayed by our hopes as well as by technical matter:
Now comes the tricky part… what happens if you get conflicting test results.
Let’s say you get a positive result on an at-home antigen test (like the BinaxNow) and decide to take it again “just to be sure”.
Then you get a negative result on the 2nd Binax test. Now you schedule an appointment to get a PCR test.
A couple of days later, it comes back negative.
ARE YOU INFECTED? Absolutely positively YES!
If you’re non-symptomatic and get a [Binax+ Binax- PCR-] set of results … a positive and two negatives in any order.
In that case, it is 56-times MORE likely that you’re infected than not infected … 5600% more likely!
And if you’re FULLY symptomatic and get a [Binax+ Binax- PCR-] set of results, it is 20-times MORE likely that you’re infected than not infected … 2000% more likely!
Even if you get ANOTHER PCR test and THAT test comes back negative as well [Binax+ Binax- PCR- PCR-] you are still 4-times more likely to be infected than not … 400% more likely!
And it does NOT matter the order of the test results … the math holds true regardless.
Even medical doctors conducting these tests in clinics stumble:
I know this seems VERY counter-intuitive and even most doctors who prescribe these tests (other than Infectious Disease specialists) tend to NOT understand this!
And when faced with multiple conflicting test results, most medical people will incorrectly select the LAST result as the “correct one”.
This is a DANGEROUS mistake! Again, outside of certain specialties, few medical staff are trained to think in terms of Bayesian statistics.
Vanity Fair’s palace intrigue set the COVID Collaborative of high-end epidemiologists recommending the holiday testing surge against the administration that ignored them. But that isn’t quite right. Both sides agree on turning public health into an individualistic (and commodifiable) option:
Once [ex-Harvard epidemiologist and now chief science officer at the eMed diagnostic company Michael] Mina began to advocate for rapid home tests, he encountered the same mindset: doctors “trying to guard their domain.” Some doctors had long opposed home testing, even for pregnancy and HIV, arguing that patients who learned on their own about a given condition would not be able to act on the information effectively. Testing, in this view, should be used only by doctors as a diagnostic instrument, not by individuals as a public-health tool for influencing decisions.
The U.S. approach sticks the American people with the job of administering and then interpreting the conflicting results of multiple tests. The false positives might be low in part because nearly 100 percent specificity aligns with peak viral load. But, as Harrison describes, even should the test be administered correctly, the false negatives are legion and the results of one test do not necessarily change the implications of previous ones.
Techno-utopianism offers another iteration of blaming the victim if the outcome goes south: “It’s your own fault you didn’t do the test right.” Don’t let the easy lines on the lateral flow ag card confuse matters. Against Mina’s insinuation, it’s decidedly unlike a pregnancy test.
There is also the matter of what happens when organizing society’s access to work and recreation around such tests collides with a run on the tests at local stores already suffering supply chain problems, making the tests both unavailable and priced beyond working people’s budgets.
If, on the other hand, the Biden administration hired and trained a million community health workers to go door-to-door across the country administering these tests for free — like really free — we wouldn’t be in such a free-for-all, if you’ll excuse the phrasing.
If such teams had been put in place from the beginning, they may have been able to build the trust necessary to successfully introduce a variety of time- and place-specific public health interventions that would likely have minimized the duration and impact of each wave of the pandemic.
Surprising the Supposedly Surprised
What’s interesting about Harrison’s direct and clearly written posts is that his recommendations are framed by the context of what the U.S. can, or is willing to, offer right now: not much.
Yes, everyone should be able to test themselves whenever they wish, all the time. But the U.S. chooses to position itself as unable to pursue such a public health program. Should the sensitivity and specificity reported on the test boxes match their actual outcomes? Yes, they should, however righteous the original testing went into bringing the products to market. Should the efficaciousness and effectiveness of vaccines match? Yes, that would be nice.
There are expectations that individual American consumers hold about solutions — cheap and immediately effective — that the market repeatedly promises but can’t deliver. In this case, the multifactorial virus doesn’t cater to such an ideal of a single packet solution. And the public health response we need, and the market treats as a rival, is starved to near-death.
The U.S. government, and governments around the world, treat the capitalism that helped spring the COVID virus out of commoditized forests as more real than the ecologies and epidemiologies upon which the global system depends. To protect that mirage of a difference, each new variant that has since emerged is strangely presented as the beginning of the pandemic’s end, resetting the next round of denialism, instead of alerting us that in reality, without a change in public health practice, we’re caught in a daisy chain of viral evolution.
Each “surprise” that the COVID virus refuses to cooperate with such an expectation, acting in its own interests instead of ours, also serves to protect the system from the implications of its refusal to act. Surprise — pretending we don’t know what we know — is itself an ideological project. The business of governing a system in decline, after all, is about managing expectations. All is well, get back to work, until, suddenly, it isn’t, as it always was.
From the virus’s vantage, the resulting public health dithering and half-measures serve the virus as both escape hatch out of our control efforts and selection pressure to evolve around those campaigns. A combo that leads to the worst of epidemiological outcomes.
If we wish to unplug out of this trap, we have to organize together against our rulers and their financers. We must deploy a full-spectrum intervention that drives the COVID virus under its rate of replacement.
That requires we reject not only Washington’s business bipartisanism, but also the core model of our economy around which our civilization is organized. That’s no small matter, of course, but with climate change and other pandemics also in the wings, likely our sole option out.
He said community transmission was now widespread in the capital Honiara and some provincial areas.
“For the Western Province, a surge in flu-like illness was noted in Rukutu village where we suspect a recent gathering involving those who travelled from Honiara and may have transmitted covid-19.
“Our team has reached the village, distributed face masks, advised on covid-19 safe measures and collected samples for testing in Gizo.”
He said health officials were still waiting on lab results from Australia to determine the variant they are dealing with in the current outbreak.
Loss of staff a challenge
Dr Togamana said loss of staff had added challenges to the already overwhelmed health system.
More than 100 frontline workers in Solomon Islands have been infected with covid-19 and are isolating.
“Our only national referral hospital [Honiara] is now compromised. Many staff from the Ministry of Health also tested positive and continue to work from isolation,” he said.
“Guadalcanal health teams have also reported six of its workers isolated at Good Samaritan — four have tested positive while the remaining two await the results.”
Dr Togamana said 24 Honiara City Council health workers had also tested positive with covid-19.
This article is republished under a community partnership agreement with RNZ.
The Kiribati Health Ministry has confirmed that the atoll island nation has surpassed 100 covid-19 cases after it recorded 37 new positive infections yesterday.
There are 116 people infected on Tarawa – 36 imported and 80 local cases.
Nine new cases have been found in Butaritari Island, prompting the government to advise local authorities to enforce a lockdown.
Several other islands have been placed under strict restrictions — including South Tarawa, Betio, and Buota — to stop the virus from spiralling out of control.
Meanwhile, the government said that from today, fishermen in South Tarawa and Betio would only be allowed to go fishing between 6am and 2pm.
Only four people would be allowed to be on a boat or part of a group fishing near shore, it said.
The government has declared a state of disaster and the entire nation — of 120,000 — is on lockdown under a strict 24-hour curfew.
‘Real fear’ in community
Speaking to RNZ Pacific from Tarawa, freelance journalist Rimon Rimon said the increase in positive cases had caused “real fear in the community”.
“That’s the initial reaction that people have, when their life is in danger, they panic you know. That’s certainly the situation in Kiribati,” he said.
Kiribati Fisheries Minister Ribanataake Tiwau (left) and Health Minister Tinte Itinteang who are part of the country’s Covid-19 Response Taskforce. Image: Kiribati Govt/RNZ Pacific
Kiribati was among a handful of countries that were covid-19-free, mainly because it kept its borders shut to the outside world for almost two years.
More than 93 percent of its eligible population has been vaccinated, while just over 50 percent are fully vaccinated.
But the nation is well short of its target of inoculating 80 percent of its target population, even though the government announced in September 2021 that it had enough vaccines to immunise more than 70,000 people over 18 years old.
Rimon said while the vaccination programme was rolled out smoothly, it was not adequate for Kiribati to open its borders freely — as in the case of other countries.
“Once the government opened up its borders and brought in its flights that’s when things changed completely,” he said.
Change ‘pretty sudden’
“The change was pretty sudden on the people and also the government, and we can see on the ground the response is not as efficient as people would want it to be.”
It was still unclear how the virus spread into the community after a flight carrying 36 covid-19 positive people arrived from Fiji on January 14, he said.
“At the moment our Ministry of Health is on top of things but as I understand they are overwhelmed at the moment with resources and manpower.”
Meanwhile, the authorities are advising people to strictly follow the covid-19 protocols to minimise the risks and spreading the virus in the community.
This article is republished under a community partnership agreement with RNZ.
New Zealand could be facing 50,000 daily omicron infections by Waitangi weekend, according to modelling by US-based health research organisation, peaking at about 80,000 each day just a few weeks later.
There are also warnings this country’s ICU capacity will come under “extreme stress” through February and March.
These are of course predictions and should be viewed as such, however they have been given credence by New Zealand’s leading experts, including University of Otago professors Nick Wilson and Michael Baker: “Our impression is that this work is of high quality and should be considered by NZ policy-makers … [it’s] an organisation with a very strong track record for analysing health data (with some of the best epidemiologists, health data scientists and computer scientists in the world).”
The modelling by the IHME at the University of Washington shows the “most likely” scenarios are based on vaccinations carrying on at the expected pace, mask use staying about the same, and 80 percent of those already vaccinated getting a booster within six months — the numbers do drop if 100 percent get their booster and then again with 80 percent of people using masks whenever they’re out in public.
Under the ‘most likely’ scenario, daily infections start to rapidly take off almost immediately: by February 1 at just over 13,000, by the 9th hitting about 62,000, and peaking in mid-February at over 81,000.
Numbers drop slightly
The numbers drop slightly if everyone gets their booster shot, but there is a significant difference when 80 percent of people are wearing masks.
These are the two public health controls taken into account, so the modelling does not include other measures in place, for example, under New Zealand’s red setting; the different responses around the world vary considerably and compliance would be difficult to accurately gauge.
After peaking in mid-February, infections are projected to fall back to around 50,000 by the first week of March, then tailing off through the rest of that month and April.
The government has been preparing for up to 50,000 cases a day and this week unveiled the “three phase” response, under which testing, contact tracing and isolation requirements will change once cases start to rapidly increase.
Associate Health Minister Dr Ayesha Verrall gives details of the three-phase government response to the Omicron outbreak. Image: Angus Dreaver/RNZ
In the face of criticism the government had failed to increase the number of fully resourced ICU beds, Health Minister Andrew Little said there were 289 ICU or High Dependency Unit beds available, insisting that could be increased to up to 550 under surge capacity if needed.
Strongly challenged
That was strongly challenged by clinicians and ICU experts who said the extra capacity was more like 67 — totalling 356 — mainly due to an acute shortage of highly skilled ICU nurses
At the peak of the outbreak, in early March, the modelling estimates 458 ICU beds could be needed, and occupancy could come under “extreme stress” for a number of weeks.
Experts from the University of Otago summarised and analysed the findings, saying the government should take heed and consider police settings accordingly.
They noted socio-economic status and ethnicity were not taken into account, so the modelling would not highlight potentially disproportionate impacts on Māori, New Zealand specific data is incomplete, if delta cases start emerging again and we end up with a “dual variant” outbreak the numbers could be worse, and ICU capacity — outlined in classified Across Government Situation Report leaked to Māori Television — may be underestimated so the predicted pressure on the healthcare system may be even greater.
The authors also draw attention to the “high uncertainty” in the data, for example “the number of cases in hospital might peak at 2790 in early March 2022 … but the 95 percent confidence interval around this 2790 figure is large at: 120 to 9,070”.
“As well as considering the strengths and weaknesses of this IHME modelling, policy-makers will need to consider the potential social and economic disruption from an Omicron outbreak,” they conclude.
Stronger border approach
They also call for a stronger approach at the border, as a key area of vulnerability.
“The NZ government is obviously taking this threat seriously with a recent suspension of future places in MIQ. However, this change will not have an impact on arriving cases until March 2022.
“Therefore, substantially reducing the risk now will probably require a rapid and marked reduction of incoming international flights from some countries (ie, until their outbreaks subside in coming weeks).”
Professor Baker also says the phased opening of the border, due at the end of February, should be pushed out, and the time between the second vaccine dose and booster reduced from four to three months.
This article is republished under a community partnership agreement with RNZ.
A covid-19 Māori health analyst says more than 106,000 vaccinated Māori are not eligible for a booster shot until after March 1 — too late to protect against the expected omicron surge in Aotearoa New Zealand.
Dr Rāwiri Taonui is calling on the government to urgently pull back the waiting period for boosters from four months to three.
He said otherwise Māori will be dangerously exposed to the serious outbreak widely expected by the end of February.
Dr Taonui said the age banding for the original vaccination rollout favoured Pākehā (an overall older population) and pushed Māoridom’s more youthful population to the end of the queue.
“Many Māori didn’t become eligible for vaccination until September 1. Around that time, there was a 23 percent gap between Māori vaccination and the national average,” Dr Taonui said.
“Our health providers have done a really amazing job in terms of narrowing that gap back to 10 percent and that included vaccinating over 106,000 people since November 1.
“But the inequity rolls on because now those people wouldn’t be eligible for a booster until March 1 — and that’s going to be too late if omicron surges as we expect it will through February.”
International evidence
Ministry of Health data shows 571,052 Māori aged 12 years and over are eligible for vaccination.
Dr Taonui said international evidence showed a third booster Pfizer dose increased protection 55 to 65 percent against infection, 70 percent against symptomatic illness and 90 percent against hospitalisation, including in older populations over 65 years.
But on Sunday’s numbers, the Māori uptake of boosters was 18.9 percent of the eligible over-18 years population — well behind the national average of 27 percent.
“The government must shorten the qualifying period to three months to meet its obligation under Te Tiriti o Waitangi to actively protect the lives of Māori,” Dr Taonui said.
He said Britain, Australia and some other countries allowed a three-month booster waiting period.
“The international reporting is telling us that indigenous peoples, for example in Australia, Canada and the United States, are being disproportionately inundated with omicron infections.
“Māori are going to be particularly vulnerable because in terms of total vaccinations we’re 10 percent behind the national average. We’re about 12 percent behind in terms of being fully vaccinated and with the booster rollout we’re nearly 10 percent behind the national average there as well.
Māori children vulnerable
“This leaves 17.6 percent of Māori aged over 12 years unvaccinated and therefore particularly vulnerable to the hyper-infectious omicron variant.”
Dr Rawiri Taonui … Indigenous peoples in countries such as Australia, Canada and the US have been the worst affected by omicron. Image: LDR
The low rate of vaccination for Māori children aged 5-11 years was “very, very serious”, he said.
“The Ministry of Health hasn’t released national figures yet but there are progress figures available for different DHBs. In Auckland, the Māori rate of tamariki vaccination is running at about half that of the rest of the city. That is another area where Māori need more support from the government.”
Dr Taonui said during the holiday period, active Māori cases declined by 70 percent while active Pākehā cases increased. That reflected higher vaccination rates and was a credit to the vigilance and leadership among Māori communities.
Notwithstanding the lower numbers for Māori, the country’s relatively good vaccination rates, compared to other countries, could slow omicron down but the traffic light system would only go so far with that, he said.
“At the end of the holiday period there was quite a lot to celebrate, except now we’re facing omicron. We’ve also had cases become more widespread across 18 of 20 DHBs now.
“So the traffic light system actually facilitates the more widespread movement of the virus. omicron is going to accelerate and increase quite rapidly, certainly before the middle of February.”
Local Democracy Reporting is Public Interest Journalism funded through NZ On Air.
Fiji has recorded 987 covid-19 cases, says Ministry of Health permanent secretary Dr James Fong who says the latest deaths are a “stark reminder” of the seriousness of the pandemic.
Dr Fong said 656 cases were recorded last Saturday while 81 new cases were recorded on Sunday and 250 new cases in the past 24 hours ending at 8am on Monday morning.
Dr Fong said it was known there remained a high risk of resurgence of endemic variants and the arrival of new variants.
“Our socioeconomic survival depends on our ability to build and sustain individual and community-wide resilience. We should expect that covid-19 will be endemic, however we need to appreciate that ‘endemic’ doesn’t mean harmless,” he said.
“Endemic means that we expect continued circulation of the disease in the community, the baseline levels of which are yet to be determined.
“Leptospirosis, typhoid and dengue are endemic in Fiji and they are associated with serious outcomes, especially when the number of cases increases to outbreak levels.
“Building resilience means that we must adopt healthier lifestyles, make covid-safe behaviour a habit that we adopt and support others to adopt. Our objective is to live with the virus and, at the same time, ensure a high level of transmission suppression and prevention of severe outcomes.”
Luke Rawalai isa Fiji Times journalist. Republished with permission.