University of Otago covid-19 experts are not immune to the increasingly vitriolic attacks dished out to scientists commenting on New Zealand’s pandemic response.
Among a litany of attacks University of Otago epidemiologist Professor Michael Baker has endured over the course of the pandemic, at the start of this week a caller told him he had “a target on his back”.
Professor Baker said he kept the caller on the line for about 20 minutes and asked him what that meant “in real terms”.
The caller was an anti-vaxxer who was accusing Professor Baker of propaganda on behalf of pharmaceutical companies, telling him vaccines were dangerous, especially so for children.
The caller had half-baked information gleaned from various sources that did not really make sense, Professor Baker said.
“He had these slogans he was throwing at me, but when I asked him what he meant he didn’t really have any answers.”
Professor would call police
But Professor Baker said he had not raised any concerns for his safety with his employer, the University of Otago.
If anyone made a threat where he felt he or his family was unsafe he would not hesitate to involve the police.
The Wellington-based scientist received the occasional phone call where a caller delivered a stream of abuse and hung up, but Professor Baker said he was most likely to receive abuse in the form of emails, averaging a few attacks by email every day.
As an exercise, Professor Baker began classifying the forms of abuse he received into “five categories of insult”, he said.
There were the incoherent streams of abuse, which were easily dealt with, he said.
Some people had major grievances but did not know where to go, and contacted him to vent and, in some extremely sad cases, he would reply and express sorrow and sympathy.
There were anti-vax propagandists whose positions were not based on facts, which he ignored.
There were those with ideological stances who disapproved of the government’s overall strategy, who at times delved into conspiracy theories.
Personal attacks stream
Finally, the group he found the hardest to deal with came as personal attacks from a small stream of people who persistently contacted him, and tried to undermine his ability to comment.
“Talking about how you look, or how you appear – they’re obviously making quite a concerted effort to look at where you might feel a bit vulnerable,” he said.
The attacks had never made him question his role of speaking publicly about the pandemic response, Professor Baker said.
Dr Jemma Geoghegan … limited her media exposure. Image: University of Otago
University of Otago evolutionary virologist Dr Jemma Geoghegan said she, too, had not raised any concerns with her employer.
She said “no” to about 90 percent of media requests because the issues were not related to her field of expertise.
In limiting her media exposure, she had limited the number of people who wanted to harass her about her expertise, Dr Geoghegan said.
“I don’t generally speak about vaccines, so [that] abuse isn’t aimed at me,” the Dunedin scientist said.
‘Weirdly strong views’
However, she had published on covid-19 origins and people had “weirdly strong views about that”.
The issues dealt with by her Auckland counterparts were not surprising though and she had sympathy for them.
“This is happening all around the world,” Dr Geoghegan said.
“I’ve got international collaborators that … I think their mental health has suffered.
“Before covid, or at the start of covid, they were really prominent on Twitter and stuff like that, and now they’ve had to delete their accounts because of the amount of abuse they’ve got.”
Hamish MacLeanis an Otago Daily Times journalist. This article is republished under a community partnership agreement with RNZ and this story first appeared in the Otago Daily Times
Fiji is bracing for a third wave of the covid-19 virus after tests have confirmed the presence of the omicron variant in local communities.
The country’s Health Secretary Dr James Fong said today the ministry was prioritising testing of suspected individuals to prevent severe illness and death and to focus on suppression where the risk of transmission was high.
“Omicron is vastly more infectious than delta. As such, in keeping with what we see in other countries, the omicron will become the dominant variant,” said Dr Fong.
“As omicron spreads very fast, you should assume you are infected, and self-isolate, if you develop any cold/flu-like symptoms such as runny nose, sneezing, nasal congestion, sore throat, cough, body ache, or fever.
“Gatherings have been observed where covid-safe measures have not been followed, or people have attended while having symptoms. We ask that if you have relaxed in your observance of covid safe measures, that you please resume now.
According to Dr Fong, 580 new cases of both the delta and omicron variant were recorded between Monday and eight o’clock today.
Of the 580 cases recorded since the last update, 146 cases were recorded in the Northern Division, 111 cases were recorded in the Western Division, 303 cases were recorded in the Central Division, and 20 cases in the Eastern Division.
2417 active cases in Fiji
There are currently 2417 active cases of covid-19 in the country.
The Health Ministry has recorded two additional deaths in its latest report, bringing the total death toll to 712 during the pandemic.
However, Dr Fong said the omicron variant was likely to cause milder disease as data from the United Kingdom and South Africa had shown the risk of hospitalisation was reduced by 80 percent and, once in hospital, the risk of severe diseases was reduced by 70 percent when compared to the delta variant.
“As with previous variants, unvaccinated people are at higher risk of severe disease. With more than 92 percent of adults fully vaccinated, we expect that our high vaccination rates, plus the infection-induced immunity from the large number of people who were infected during the last wave, will help to lower the number of people that develop severe disease.
“We continue to see that the majority of individuals testing positive in medical facilities are presenting for non-covid medical problems and found to be positive while undergoing routine screening as all admissions to the hospital are currently tested for covid-19.
“Also, the vast majority of cases turning positive have minimal symptoms and remain stable.
He added that severe outcomes would be expected in some individuals, including those who have been immunised with two doses of the vaccine, especially people with severe underlying medical conditions and people over the age of 50.
‘Monitored … in a timely manner’
“We have in place measures that ensure that those vulnerable to severe disease are adequately monitored, tested, retrieved, and effectively managed in a timely manner before their conditions worsen.
“However, we need the cooperation and support of community networks in formal and informal community settings and business settings, working in tandem with the ministry.
The ministry has advised the public to self-isolate at home if they have any of the covid-19 symptoms.
A health care worker must isolate for seven days while everyone else is required to isolate for 10 days.
Meanwhile, Fijians who are eligible to get their booster shot have been advised to do so as the country fights the new variant.
Josefa Babitu is a University of the South Pacific student journalist and contributor to Asia Pacific Report.
Fiji parents are advised not to send their children to school today if they are not feeling well as the country is rocked by a third wave of the covid-19 pandemic.
That was the advice from the Ministry of Education as the last term for 2021 begins on January 4 for Years 8 to 13 to make up the education gap.
Education Minister Premila Kumar said the students were expected to comply with covid-safe measures introduced in school, including the wearing of masks.
“We must all take the necessary steps to reduce risk of covid-19 in our communities to keep our schools safe,” Kumar said.
The minister said the ministry was also aware that not all students had had regular and reliable access to online learning tools during the long school closure due to covid-19.
As such, she said the return of students to school this month would provide them with the opportunity and resources to work closely with their teachers to successfully complete the requirements of the 2021 academic year before progressing to the next level.
“We know that face-to-face learning is vital for the academic achievement, mental and physical health, and overall well-being of our students.
“By continuing to work together, we can help ensure a positive school experience for everyone.”
Kumar added that the schools would be finalising the provisional enrolments for the 2022 academic year by the end of January 2022, giving parents and guardians ample time to prepare their children for the new school year.
805 new cases in Fiji
The Ministry of Health and Medical Services reported 805 new cases of covid-19 in the last three days ending at 8am on Sunday morning.
“Since the last update on 29/12/2021, we have recorded a total of 805 new cases; of which 316 new cases were recorded on 30/12/2021, 223 new cases were recorded on 31/12/2021, and 266 new cases in the last 24 hours ending at 8 am this morning,” stated the ministry in a statement.
The Fiji Times reports that Health Secretary Dr James Fong said plans to amend curfew hours and close Fiji’s international borders were still under discussion.
He said that if a variant was transmissible enough, stringent border and community measures would only delay the inevitable entry and spread of current and future variants of the covid-19 virus.
“We must all get vaccinated when it is our turn and continue to be strict with our covid-19 safe measures,” he said.
The ministry, in a statement, said that from January 1, 2022, travellers from travel partner and non-travel partner countries must produce a negative covid-19 PCR test taken no more than two calendar days before the scheduled day of departure.
Timoci Vulais a Fiji Times reporter. Republished with permission.
Success can be its own worst enemy. If the plane doesn’t crash or the ship doesn’t sink, that doesn’t prove the safety measures were unnecessary, or that anyone can fly a plane.
It can also be taken as an indication that the safety measures are working. Ditto during a pandemic.
Arguably New Zealand has managed the best response to covid in the entire world. This didn‘t happen by accident. It reflects the skill and dedication of tens of thousands of people working at the borders, in MIQ facilities and in the public health system. Hundreds are alive and well today who would have not have been if the government had bowed to pressure from the business sector and its friends in the media, and thrown the borders open prematurely.
Little of this reality has been reflected in a media narrative that has been skewed towards allegations of confusion, mis-management, shambolic disarray and the hardship resulting from the government’s treatment of public health as its major priority. Yes, this can be hard financially (and stressful) on people whose business model was built on a pre-covid reality where foreign tourists and locals could mix and mingle freely.
We now have vaccines, but they do not render even the double vaccinated entirely bullet proof.
Therefore, the need for caution in removing restrictions and safeguards remains, especially given what we know about how readily delta and omicron spread covid-19. Moreover, and throughout the pandemic, compassionate taxpayers have poured hundreds of millions of dollars into the hospitality and tourism sectors. They did so (a) to keep firms afloat and workers in jobs, while (b) those firms adapted to the new reality.
Some firms in hospo and tourism have made that adjustment. However, many others have been given a media platform to repeatedly complain about their plight, as if the government (and taxpayers) have a duty to sustain their old business model for them, forever.
Instead of providing a megaphone for grievance, shouldn’t the media be more willing to challenge those employers to explain how they’ve dynamically changed their business practices, and what their transition plans look like?
The last time I wrote about this, this was mis-construed by some as an argument for turning the media into government apologists or publicists, and preventing journalists from heroically doing their job. To be clear on this point: there’s not much that’s heroic about amplifying complaints without context or pushback.
Also IMO, it isn’t particularly heroic to be wilfully naïve about the political dimensions of your work. Meaning: the risks of being an apologist and virtual publicist apply not only to government policies and actions. Especially in the aftermath of the delta outbreak mid-year, much of the media has been a virtual echo chamber for the attack lines originated by the Opposition.
The wilful lack of context has, at times, been breathtaking. Outside the business pages, the recognition of the relative success of this country’s economic management during the pandemic has been almost non-existent.
– Gordon Campbell
The wilful lack of context has, at times, been breathtaking. Outside the business pages, the recognition of the relative success of this country’s economic management during the pandemic has been almost non-existent.
Last year, New Zealand – and the rest of the world – were expecting the worst recession since the 1930s. In some countries, the covid recession has been deep and lasting. Here, not so much.
In fact, our Reserve Bank has recently been forced to intervene to dampen down the inflationary fires within a growing economy. Much as this may hurt the feelings of the centre-right, the results have vindicated the borrow and spend approach taken by the government in unison with the Reserve Bank.
Last month, the government books were opened. People are in jobs. Unemployment fell to 3.4 percent in the quarter to September, and is headed further downwards. Yes, prices are rising faster than wages, but this is largely due to supply chain bottlenecks and oil price rises beyond our control.
It is also because of record global demand for our farm exports that — despite what the Groundswell protesters claim — has left farmers extremely well placed to meet the costs of meeting their climate change and water quality obligations.
As this column has consistently argued, the inflationary surge in prices is forecast to peak early in 2022, and to recede sharply thereafter. Despite the covid effect, the Operating Balance evidence is that deficits will revert to surplus in 2023/24, three years ahead of schedule. Similarly, there will be a spectacular decline in net debt, which will peak at 40.1 percent of GDP next year, before steeply declining to only 30.2 percent within five years, a full 18 percentage points below the gloomy forecasts on debt that were made at the outset of the pandemic.
So much for fears that covid-related spending would impose an intolerable debt burden on future generations. Instead, the borrowing sustained (and generated) levels of economic activity that will largely take care of the debt incurred in obtaining the subsequent social benefits. Another triumph of neo-Keynesianism over the policies of austerity.
Finally on this point, the Treasury is predicting government debt will fall from 35.3 percent of GDP to only 30.5 percent next year and head further downwards over the forecast period. This means that New Zealand is blessed with one of the lowest Crown debts to GDP ratios in the developed world.
Among other things, it leaves acres of room for the government to borrow more to invest in infrastructure and social needs. There is also plenty of headroom in the economy for a further active response to covid-induced needs. More to the point, these figures render the centre-right criticisms of government economic policy almost entirely irrelevant.
This is what I mean about a skewed media narrative. In its horse race journalism fixations on the new leader of the National Party — did he or didn’t he best PM Jacinda Ardern in the House etc etc — there has been almost zero attention paid to what Luxon is advocating as an alternative to the current economic settings. For all his vaunted experience as a CEO, Christopher Luxon has so far brought nothing whatsoever to the table by way of an alternative economic strategy.
All that Luxon has offered (so far) are 40-year-old Thatcherite ideas about reducing debt, balancing the budget and tinkering away at the fringes with wasteful government spending. These policies are antiquated relics of a bygone era.
There is a fixation on style — is he John Key Redux? — as though querying Luxon closely about his lack of content would be bad form, and rather mean to such a political novice.
– Gordon Campbell
There is a fixation on style — is he John Key Redux? — as though querying Luxon closely about his lack of content would be bad form, and rather mean to such a political novice.
In reality, it seems as if the centre right has slept through the Global Financial Crisis, let alone the covid recession. In both these crises, the countries that did best — including the US — borrowed and spent their way out of trouble. The countries (mainly in Europe) that did worse during the GFC in particular, had actively embraced the policies of austerity, the ideology of small government and the service cutbacks that the current leadership of the National Party is being allowed to peddle by a compliant media.
There’s so much more media interest (and clicks) in the Luxon vs Ardern popularity contest.
Footnote: In the US over the past few weeks, the same debate has arisen over the prevailing media narrative on the Biden presidency. Again, the lack of context (e.g. in the coverage of the US exit from Afghanistan) , the relentlessly negative focus on trivialities (e.g. Biden’s cough) and the resort to horse race journalism (e.g. the Biden approval ratings) all have their counterparts here. Here’s a Columbia Journalism Review article on the media’s skewed stances towards Biden.
Much of the recent debate has been kicked off by a (paywalled) column written by the Washington Post’s Dana Millbank, who has argued that the US media’s amplification of what are relatively insignificant government failings is serving to advance the country’s drift to the extreme right. As Millbank says in this MSNBC interview:
“Compare the last four months to the last four months of 2020, when Donald Trump was threatening to not honour the result of a free and fair election..He was embracing the Proud Boys white supremacists, and embracing QAnon. He was sabotaging the Post Office.[Yet] in that period of time he got similar to, and even more favourable, coverage than what Biden is getting today.”
In this situation, the media’s ordinary combative instincts – they originate in the admirable journalistic urge to hold power to account – can be ill-suited to recognising, let alone dealing with, the bigger picture. Because, Millbank argues, the stakes involved in the US are more than the usual party political jockeying between Democrats and Republicans. In his view, the struggle is between small “d” democrats, and authoritarians.
As Milbank said in his Post column, “Biden is attempting to re-establish democratic norms. The people opposing him are using fascist tools of deception and voter disenfranchisement. Neutrality in this struggle is not a virtue.”
Footnote Two: Luxon’s CEO experience might be the worst possible preparation and qualification for heading a government. After all, CEOs are answerable only to the shareholders, and their main fidelity is to the bottom line. Yet governments — if they’re competent — need to be willing and able to juggle competing interests, to acknowledge the minority view, and to minimize the risks to the vulnerable, even if this involves sometimes abandoning the quest for optimal economic efficiency.
By and large, the current government has managed that balancing act pretty well. Arguably, by focusing so much coverage on the angrily disgruntled, the media has taken an easy clickable route that downplays — or negates — the fact that such people are actually outliers within what has been so far, a successful response to the pandemic.
Pacific Island New Zealanders are now 90 percent fully vaccinated against covid-19, and a public health expert is urging them to keep up that momentum in the New Year.
In a daily briefing, the Ministry of Health said 90 percent of eligible Pacific people in New Zealand had now had both vaccines.
Associate Professor Collin Tukuitonga from the University of Auckland said that is a tremendous effort and the threat of omicron is the next challenge.
He hopes the community embraces booster shots to guard against the more infectious variant.
“It looks as if the two doses doesn’t give you enough protection for omicron, and the most important priority now is to get people to get their boosters as soon as that’s possible.”
He hopes as many regions move into lower levels of restrictions in the government’s Framework Protection system people will still stay vigilant, contact trace and get tested.
“There’s a risk that people might have gone back into a lower level of alertness, so I would hope that we maintain that [alertness].
Ramp up once again
“In mid-late January I think we’re going to have to ramp up once again in respect of rolling out the vaccine for the young ones.”
Children aged between 5 and 11 become eligible for covid-19 vaccinations in mid-January, and those 12 and older are already eligible.
“Parents are perhaps less certain about the benefits and more concerned about risks. So every effort is going to be needed to get the vaccination rollout in children up to the kind of levels that is needed.”
This article is republished under a community partnership agreement with RNZ.
After a year and a half, the ravages of the pandemic show no signs of slowing down. The Omicron variant is spreading rapidly around the globe and is nowthe dominant version of Covid in the U.S., accounting for an estimated 73 percent of new cases. The U.S. is now averaging over213,751 new Covid cases per day, which is equal to 85 percent of the number of cases during the peak when the highest daily average was reported on January 7, 2021.
While it is still unclear if Omicron causes more severe symptoms than other strains of Covid, it’s clear based on the variant’s high transmissibility1that the sheer number of infections puts the most vulnerable members of the population at serious risk of illness. In just six weeks there has been a39 percent increasein Covid-related hospitalizations all over the country, likely from the spreading of both the Delta and Omicron variants.
After all this time, the complete lack of a public health-based approach to this pandemic is criminal. The Biden administration has instead chosen to lay all responsibility on the individual decision to vaccinate or not, implicitly blaming the unvaccinated for the ongoing ills resulting from the pandemic. After facing heavy criticism for his administration’s incompetent management of the Omicron surge, Biden recentlyaddressed the status of the pandemic, doubling down hard on this narrative. He said, “If you’re vaccinated, you’ve done the right thing, celebrate holidays as you’ve planned them.”
In the same address, Biden pledged to distribute 500 million free Covid rapid tests. While this may seem like a huge number, 500 million tests will only last abouta month, and such a limited supply of rapid tests will also miss many positive cases, which often require more than one test per individual to detect. Following exposure to Covid, a person may initially test negative but then test positive after the virus has had time to replicate and achieve a detectable viral load. Biden’s pledge, with no promise of an ongoing supply of tests, is laughably and criminally inadequate. The tests will not be available for at least a few weeks, far too late to deal with the Omicron surge. When they do become available, it will not be all at once but inbatches, leaving the vast majority of people needing a rapid Covid test without one.
During his candidacy, Biden was relentlessly critical of Trump for the lack of available testing, but since taking office, he has focused almost exclusively on a“vaccination only”strategy. Abbott, a Covid test manufacturer, evendestroyed millions of testsdue to decreased demand in August 2021, when the administration could have been preparing for the entirely predictable holiday surge and the increase in testing demands. This reveals how the incentives of a capitalist health system are fundamentally at odds with the goals of public health and the production of lifesaving technologies. What is” rational” from the standpoint of capital is a stupid and deadly mistake for public health.
Biden promised to open federal testing sites across the country, but provided no provisions for people to get paid time off, leaving workers to “figure it out” at the mercy of their employers. AsBree Newsome Bass pointed out, taking time off from work to wait in long lines for testing is often not an option for the poor and working class. Even when people can obtain tests, the delay in the delivery of PCR results, partially a result of a dearth in lab facilities, makes interpreting and acting on test resultsmore difficult.
Despite all of Biden’s talk about “plans” to fight the pandemic, the United States has yet to establish a coordinated system for tracing cases and isolating those who test positive. Again, this leaves it up to individuals to inform close contacts of positive test results and to isolate themselves to the best of their ability. Unsurprisingly, after years ofgutting public health systemsin an endless effort to “cut costs,” the CDC does not even have theepidemiological infrastructureto track outbreaks accurately. As a result, the American government is relying on data from other countries to do this.
With its vaccine hoarding and exploitative “back to work” attitude, the United States government is only interested in ending the pandemic as long as it can also profit from it. The current administration has disingenuously placed the entire blame for the current state of the pandemic squarely on the unvaccinated. This narrative was crystalized in the recent callousstatementfrom the White House Covid Response Team, which preemptively blamed the unvaccinated for “a winter of severe illness and death,” and for overcrowding and overwhelming hospitals.
But in the absence of other public health measures, “vaccination only” has proven not to be the magic cure that the Biden administration insists it is.
In New York City, for example, higher vaccination rates relative to the rest of the country have not stopped Omicron from spreading like wildfire among both vaccinated and unvaccinated individuals. Vaccines represent just one piece of aSwiss-cheese modelof prevention during the pandemic; focusing exclusively on vaccines without mass expansion in measures such as testing, tracing, and isolation (TETRIS measures), and without making workplaces, schools, and other public spaces safer, will not help bring an end to the pandemic. Relying on vaccines alone was always a poor strategy, and in the face of Omicron, it stands no chance at all.
Joe BidenandKamala Harrisclaimed that no one could have predicted the spread of the Omicron variant. An interesting claim, given that just a few months ago, experts presented the Biden administration with a plan to deal with this very situation. In October, Covid testing experts met with the Biden administration to recommend ramping up production of rapid Covid tests and making them readily available to the public, to prevent a surge during the holidays. The ill-fated proposal,“Testing Surge to Prevent Holiday COVID Surge”, was promptly rejected by the Biden administration, which said they did not have the capacity to produce tests at that scale. The administration decided instead to focus only on vaccination. They later announced a ridiculous plan in which insurance companies would reimburse privately insured patients who would buy a two-pack of rapid tests for up to $35, once again leaving people on their own to squabble with insurance companies known to do everything in their power to reject claims and not pay for healthcare.
The “individual responsibility” narrative of vax, mask, shut up, and work is beneficial for the ruling class as it exploits our labor and our deaths for profit. In addition to vaccination, there are other safety measures that could reduce risk of infection in a pandemic, such as providing people with housing, workers’ democratic organization of their own schedules and working conditions, and paying workers to stay home if exposed. The ruling class, however, would never allow any of these options because they would cut into their profit margin.
As people have died during the pandemic, BioNtech and Moderna shares have increased to the tune ofbillions of dollars. CEOs continue to make million dollar salaries while workers are underpaid and left working in precarious situations. These exploitative conditions have forced many workers (including those in health care, retail, and hospitality) to leave their jobs or quit their fields altogether.
Earlier in the pandemic, many health insurance companies had waived Covid-19 treatment-related costs for patients, but with the vaccine rollouts, the companies haveended the practice. The waivers should never have been eliminated, and the federal government should cover all costs of Covid-related hospitalizations indefinitely. These changes could leave patients — not only those who are unvaccinated, but those hospitalized with breakthrough infections, as well as children who are not yet eligible for the vaccine — with hospital bills totalling thousands of dollars. Bending to supply and demand, the CDCjust shortened the recommended Covid isolation periodfrom 10 days to five days in order to get peopleback to workfaster. The function of the CDC is to analyze risk to determine public health recommendations. In doing so, however, it balances what costs are acceptable — both human and economic — and for what gains. As such CDC hashistorically been malleableto the demands of capitalism.
In a system that truly prioritized preventing people from getting sick and treating illness, all workers would be adequately paid, given access to safe working conditions, and have ample time to rest and recuperate. In such a system, people would have free healthcare instead of avoiding care or having to file for bankruptcy when they get sick. The ruling class is clearly more interested in keeping the wheels of the capitalist system turning — at the expense of the health of the workers and patients — rather than ending the pandemic. To the ruling class, the pandemic is a commodity to be monetized, just like everything else.
Discussions around the nature of the fragmented, profit-driven medical-industrial complex in the U.S. have largely been silenced in the halls of power. One would think that maybe, just maybe, the destabilization caused by a global pandemic might prompt a discussion of the way a healthcare infrastructure that was built to prioritize monetary value over human lives at every level helped to create and exacerbate this pandemic, and continues to fail to address its results. But from street uprisings around the killing of Black people by police to conversations around health care system changes, the Biden administration has been able to take enormous political energy and funnel it into centrist electoral demands under the guise of being more “pragmatic.”
And should this be a surprise? Of course not; the Democratic Party has always served as thegraveyard of social movements, defusing progressive popular mobilizations whenever possible. On the healthcare front, Biden rejected calls to bring the U.S. in line with other nations and move toward a single payer healthcare system. Today,if Biden wanted to, he could take unilateral steps towards releasing Moderna’s vaccine formulation to the WHO, but Biden’s appeal has always come from his representation as a pole of stability and safety for a vaguely defined “everybody,” when in fact, he governs in the interests of the ruling class just as reliably as Trump did.
The narrative of individual responsibility takes pressure off of the government to organize necessary collective action, and therefore leaves people isolated, often at the whims of their employers. A byproduct of constantly hammering “individual responsibility” into our heads is that people learn that they cannot rely on government institutions and health systems to look out for them. Disappointed and alienated by the for-profit healthcare system, some people find comfort in conspiracy theories and flock into the arms of charlatans selling snake oil.
The anti-vaccination crowd is indeed an easy target for both parties of capital. The Republicans have convinced them that they are more “free” by resisting vaccinations. Meanwhile, the Democrats continue to scapegoat and blame them for the current state of the pandemic. Rather than trying to convince those workers who are anti-vaccine while allowing them to work in a way that does not put others at risk, the ruling class strategy has been to use vaccine mandates instead of, rather than in addition to, these other methods of controlling the virus and increasing vaccination rates.
The ruling class wants to direct public rage away from their exploitation and convince the working class and oppressed people to blame each other, creating a “war” of the vaccinated against the unvaccinated. They need to do this to avoid exposing how the ruling class has kept the machinery of extraction and accumulation going during the pandemic at the cost of public health. They are trying to hide a healthcare system whose primary objective is to serve as a means of capital accumulation, extracting profit from people’s bodies as they become damaged by the capitalist system, not to maintain individual or public wellbeing. It would be extremely dangerous to the ruling class if the workers realized that these systems are responsible for creating and exacerbating the pandemic.
Ending a global pandemic is not an “individual issue.” Yes, people should get vaccinated. Yes, they should wear masks. And yes, Covid-19 vaccines should be available to everyone in the world who can be safely vaccinated, but vaccines alone are nowhere near enough. People should take all possible individual measures, but the ability to do so must also be readily available to them. If we want people to trust vaccinations, we need a free healthcare system that clearly prioritizes people’s health. It’s fantastically dissonant to so vehemently tell people to take personal actions to protect themselves when it is clear that societal structures do not prioritize their health. Becoming sick from Covid just adds to the many other threats to one’s existence such as lack of housing, lack of food, and bankruptcy. So it’s no surprise that shaming people for not “doing their part” under these circumstances engenders resentment and tends to backfire.
We need basic public health measures such as housing, food, debt cancellation, paid medical leave, and free medical masks, testing, and treatment. We need a society that values public wellbeing over private profit. We need to destroy the economic system that must continually find areas of capital expansion, destroying the planet we live on andputting us at risk for future pandemics. Bourgeois politicians and governments beholden to capital will deliver none of these needs.
As some North Island regions moved to the orange traffic light setting at 11.59pm last night, New Zealand has now found two omicron cases that were briefly in the community, and close contacts are urgently being chased up.
As a British DJ outed himself as the omicron community case identified yesterday, Covid-19 Response Minister Chris Hipkins yesterday expressed his disappointment in the musician’s non-compliance with rules.
Robert Etheridge, also known as DJ Dimension, went out into the community on December 26 and 27 after 10 days of isolation but before he received his final covid-19 test result.
As such, he has faced abuse online over the matter.
“I want to reiterate my apologies to those who I have inadvertently put at risk as a result of my misunderstandings,” he wrote in an Instagram post.
“I realise the gravity of the situation and I am deeply regretful to those who have been impacted; including members of the public, event organisers and close contacts.”
Etheridge had tested negative to the virus three times before while in isolation. It was also revealed today that he completed his three-day self-isolation period (after seven days in MIQ) on Waiheke Island.
“We understand they travelled by private car and ferry to the island. While on the ferry they did not leave their vehicle and travelled straight to their accommodation.”
DJ Dimension – Robert Etheridge – tested positive for the omicron variant while in the community. Image: RNZ/Instagram
Race to get to close contacts The DJ was due to play at Wanaka’s Rhythm and Alps festival but had been forced to pull out, along with another DJ known as Friction and artist Lee Matthews, who were considered close contacts.
Fourteen people who dined with Etheridge at Soul restaurant are also considered close contacts.
Eight of those people remain in Auckland, while six flew to Christchurch where they performed at the Hidden Lakes Festival on December 28. But the Canterbury District Health Board considered the risk to be extremely low.
“All identified close contacts are being urgently contacted by contact tracers,” the Ministry of Health said.
But the exact number of contacts is still being confirmed and identified, according to Hipkins.
He told media today that while Etheridge was on Waiheke Island, he had drinks on the beach with neighbours, who have been told to self-isolate.
Epidemiologist Professor Michael Baker said the fact that three of the case’s four Waiheke Island housemates had tested negative so far may suggest he was not infectious at the time.
“But again we will just have to await more of those results.”
However, the source of Etheridge’s infection remains a mystery because his case has not been able to be genomically linked to the other omicron cases that were in MIQ when he was there.
“It’s just really important that we don’t think that seven days [of isolation] is okay and that people are still cautious … After receiving several negative tests, people could still be incubating the virus and that’s what it shows us.”
Five of the international arrivals came from Australia, two from the United Kingdom, two from Singapore, one from United Arab Emirates, and one from Ethiopia.
Surveillance testing on December 27 of an Air New Zealand crew member has returned a positive result, with genome sequencing finding it is the omicron variant.
Their infection has been genomically linked to three other omicron cases from a December 24 flight that the person worked on between Auckland and Sydney.
New Zealand-based international aircrew are mostly exempt from a 14-day isolation or quarantine period as long as they meet certain conditions.
So far for this case, no locations of interest have been identified, but there are eight close contacts — seven of whom have tested negative so far.
The case was immediately transferred to a MIQ facility.
And with positive cases reaching 33 in Rotorua yesterday, iwi-lead health provider Te Arawa Covid-19 Response Hub is stepping up its testing abilities by training more staff.
Meanwhile, across the Tasman two team players and one staff member of the men’s Wellington Phoenix football have tested positive to the virus. The team is currently based in New South Wales, where cases topped 12,000 today.
‘We need to throw everything we can at it’ In light of the cases, the National Party is calling on the government to allow people to get their booster shot sooner, bring forward the timeline for children’s vaccines, and use more rapid antigen testing.
Covid-19 response spokesperson Chris Bishop said there were people who had passed four months since their second dose and had been turned away when they tried to get their booster injection.
Meanwhile, the National Māori Authority said it was not too late to introduce tougher border restrictions.
Chairman Matthew Tukaki said the government should shut the borders to anyone who was not a resident or citizen.
“We can’t afford any more unnecessary prolonged lockdowns, so anything we can do to limit the exposure of Omicron until we can get ahead of this, then I think we need to throw everything we can at it.”
Tukaki said the government should also consider extending the amount of time people from high-risk countries spend in MIQ.
This article is republished under a community partnership agreement with RNZ.
New Zealand’s Ministry of Health has confirmed that a border-related case with the omicron variant was briefly active in the community in the Auckland CBD earlier this week.
The case arrived on a flight from the United Kingdom via Doha on December 16 and is fully vaccinated with a mRNA vaccine.
They completed a full 10 days in isolation – seven days in a managed isolation facility and three days in self-isolation.
“They had previously returned three negative tests for covid-19 while completing 7 days of managed isolation at a facility in Auckland,” the ministry said last night.
However, the person went out into the community before getting the results of their day nine test after the self-isolation period was complete, the ministry said.
The day nine test result came out on December 27, by which time the case had already been out in Auckland’s CBD on December 26 and 27.
Risk of transmission
As a result, there is risk of transmission to unknown members of the public, the ministry said.
“They were immediately transferred to an Auckland MIQ facility on the same day [December 27].”
Subsquent whole genome sequencing has revealed they have the Omicron variant.
“No other covid-19 infections have been identified from the individual’s flight. Investigations are underway as to the source of the infection.”
A number of close contacts have been identified and those tested have returned negative test results.
Locations of interest include the Impala nightclub on Shortland Street, the Sunny town restaurant, Partridge jewellers, Ahi Restaurant and Soul Bar.
Some attendees have been identified as close contacts and will be contacted by public health.
Taking situation seriously
The Ministry of Health said it was taking the situation seriously and taking a precautionary approach.
“However, we do not believe that the individual was highly infectious at the time of the above exposure events.”
It is encouraging all Aucklanders to check the Locations of Interest website regularly and follow the advice provided.
“We have been doing everything we can to prepare for Omicron and to keep it out of the community since the variant was first identified. This has included undertaking whole genome sequencing on every PCR sample taken from Covid-19 cases detected in international arrivals.”
Any further information on the case and next steps will be made available today.
New Zealand’s leading daily newspaper has praised the “gift of inspiration” over global cooperation in launching the James Webb space telescope at the Christmas weekend, but has decried the failure of the international community to seriously tackle the growing covid-19 public health crisis cooperatively.
The New Zealand Herald declared today in an editorial that the timing, cooperation, and development work involved launching the successor to the Hubble telescope “is in marked contrast with the still muddled, individual country-based approach to the pandemic”.
The launch also could not help but “signify the yawning gap between what people are capable of and what they commonly settle for”, the newspaper wrote.
The launch of the James Webb telescope was a collaboration between the space agencies of the United States, Europe and Canada with people from 29 countries having worked on the project, reports AP.
“It blasted away from French Guiana on a European Ariane rocket. As with previous space missions, it involves vision, ambition and precise calculations that have to work perfectly to pull it all off,” the Herald said.
“The telescope has a 1.5 million km journey ahead, far beyond the moon, with a task of eventually gazing on light from the first stars and galaxies.
“It all hinges on the telescope’s mirror and sunshield unfolding on cue over nearly two weeks, having been tucked away to fit into the rocket’s nose cone.
“If that goes right, the telescope will be able to look back in time a mind-boggling 13.5 billion years.”
Fascinating year for science
The US$10 billion telescope project had capped a “fascinating year for space science” after the “incredibly precise landing of a rover and a helicopter drone on Mars, which resulted in the first powered flight on another planet”, said the Herald.
Noting Nasa’s science mission chief Thomas Zurbuchen’s comment welcoming the launch — “what an amazing Christmas present” — the newspaper contrasted the collaborative achievement with the “muddled, individual country-based approach” over covid-19.
“While the rocket was launching humanity’s imaginative time machine, hundreds of thousands of people on Earth were getting a ‘gift’ of covid at Christmas. Both Britain and France hit more than 100,000 cases on Saturday,” the Herald said.
“The cost of the space project is tiny compared to the US$725 billion the US spent on defence in the 2020 financial year — more than the next 11 countries combined. Next year’s bill is US$770 billion.
“It is closer to the US$50 billion amount the OECD has estimated it would cost to vaccinate the world’s population against the coronavirus and protect the global economy.
“Far more money than that — US$12 trillion — was spent by countries in financial support between March and November 2020.
Time to hatch global covid plan
“Although that support was urgently needed, surely there was also time to hatch a US$50 billion global plan for a coronavirus endgame before the vaccines came on stream in late 2020.
“Now, a year later, each country is dealing with the omicron wave its own way, and progress in distributing vaccines to poorer regions is slow. People feel frustrated the vaccines haven’t guaranteed a return to life as we knew it.
“The vaccines themselves are an amazing scientific achievement: developed quickly and still doing their job of protecting the vast majority of vaccinated people against severe covid disease.
“A study by the World Health Organisation and a European Union agency estimated in November that the vaccines had saved nearly half a million lives in a region of 33 countries.
“But it is hard for people to really absorb achievements that involve prevention: When they work as hoped, at least some people believe it’s proof the threat was overblown.”
New Zealand’s Māori vaccination rate continues to tick up, with several district health boards (DHBs) now past 90 percent for first doses.
But experts are warning rates are still far too low — with only 78 percent fully vaccinated — and with Omicron at the door, the danger the pandemic poses for Māori is still very real.
Christchurch GP Maira Patu has been at the forefront of the Māori vaccine rollout in Canterbury for much of the year, a rollout that this week hit 92 percent first doses for Māori.
“Man we’re exhausted,” she said. “It’s been hard work but it is great to see that our service and hard work has paid off. It’s amazing isn’t it.”
It was an amazing turnaround, she said, after a somewhat sluggish start.
“It’s been a struggle with getting funding and up and running. I have to admit that the CDHB has been very supportive and allowed us to operate with a kaupapa Māori service.
“But it has been a struggle, particularly around the age range. It should have been younger for Māori from the start. We should have had an opportunity to have more mobile clinics.”
‘By Māori, For Māori’ approach
In recent months, though, after a “By Māori, For Māori” approach kicked off and clinics went mobile, things changed rapidly, she said.
Six other DHBS have reached the 90 percent first dose milestone for Māori, including Auckland, the two Wellington DHBs, Wairarapa and Southern.
Another is MidCentral, based in Palmerston North but covering Tararua, Manawatū and Ōtaki, which passed the 90 percent threshold this week.
The DHB’s iwi and Māori engagement lead, Adele Small, said working at an equal level with Māori — as well as making sometimes cumbersome health services more agile — has been critical.
“Absolutely crucial, they know their communities and they’re so much closer to their communities and in touch with what their needs and requirements are.
“We just wouldn’t be able to get the buy in without working with them, and they’ve been in pivotal with telling us where we need to be; what times of the day, what businesses to approach.”
But while it’s a milestone to celebrate, no one is under any illusions.
Māori behind for full vaccination
This is just 90 percent for first doses — in MidCentral’s area, and nationally, Māori are still well behind for full vaccination.
This week, the Waitangi Tribunal blasted the government for the vaccine rollout, saying its very structure left Māori vulnerable.
The director of operations for Auckland’s Waipareira Trust, Irirangi Mako, said getting vaccinated was still too difficult for many.
“Those barriers to access just can’t be underestimated. It’s all very well to say. ‘you’ve got a vax centre here at this place’.
“But if you’ve got tamariki at home and you have no transport, even if the bus stop is right outside your house, that doesn’t mean access to being vaccinated, or an opportunity to speak to someone about that is easy.”
Covid data analyst Rawiri Taonui said it was important to bear in mind a statistical undercount of Māori.
He also said the covid outbreak is still very much a Māori outbreak. Most new cases each day are Māori, he said, and Māori hospitalisations are still increasing.
Risk over community transfer
“While overall numbers have been declining in recent weeks — including for Māori — he does not expect it to last.
“The likely scenario is as more people move from Auckland go to holiday spots, we’ll see a number of pockets and outbreaks. The risk is that will transfer over into some undervaccinated Māori communities.”
With Omicron at the door, the remaining work is even more urgent, particularly when it comes to the large tamariki Māori population.
In Palmerston North, Adele Small said they have to keep going.
“We’re just gonna keep going. We know we have a lot of work to keep doing and we know the vaccine is one of our best defences,” she said.
This article is republished under a community partnership agreement with RNZ.
Omicron could force more changes to New Zealand’s contact tracing system, with the Ministry of Health carefully monitoring the situation in Australia and the UK.
Contact tracing is critical to containing any incursion of the new covid-19 variant, but the system struggled to keep up during the height of the delta outbreak.
Tracing will be vital to contain any outbreak over the Christmas period as New Zealanders move around the country.
Director of Public Health Dr Caroline McElnay said omicron was another game changer.
“It spreads fast … cases get infected very quickly after exposure,” she said.
That made rapid tracing of contacts all the more vital, to get them isolating before they could expose anyone else.
The ministry was looking particularly closely at New South Wales were omicron cases were soaring, McElnay said.
Focus for a large outbreak
“If we had omicron in the community and if we had, in particular, some superspreading events, we might start to see a surge in cases quite quickly, and I think that might be challenging for contact tracing alone to be able to bring those numbers down.”
McElnay said omicron, like delta, spread mainly through homes or places where people spent a lot of time in close contact, so that was where the focus would be if a large outbreak developed suddenly.
Any changes to the system could include a greater focus on tracing the highest-risk cases, with less of a focus on those with very few contacts or who had not been in risky settings, she said.
“Individual cases with very few contacts who haven’t been in any high risk locations, we might not spend a lot of time identifying all of those contacts. We may, as we did in Auckland, stop recording all of those locations of interest because we know we’re unlikely to get cases from those.”
Epidemiologist Professor Michael Baker said that was the right approach.
Contact tracing was a critical part of the country’s efforts to try to stop the health system being overrun with covid.
“If we had a very fast moving omicron outbreak in New Zealand we would need all the tools we could get working at maximum effectiveness,” he said.
Huge year for contact tracers
It has been a huge year for contact tracers, particularly those in Auckland.
South Seas Healthcare chief executive Lemalu Silao Vaisola-Sefo runs a large team, including doctors, nurses, testers, vaccinators and contact tracers.
They had been strongly motivated by helping their community and buoyed by the high vaccination rates, he said, but now everyone needed a break.
“The energy levels slowly diminish over time. The last four weeks have been a really big push for staff.”
Auckland’s public health unit is walking the fine line of giving tired tracers time off, while making sure they are able to spring into action if needed.
It will have fewer staff working over Christmas and New Year, but many on standby if they need to come back.
McElnay said if there was an outbreak in a small district health board area, like Tairawhiti, the national system would kick in.
There had been big changes since the start of the delta outbreak, including a national telephone service and an email questionnaire allowing more contacts to be reached.
The system could scale up over a two-week period to be able to trace 1000 cases a day, managing 11,000 initial contacts, she said.
This article is republished under a community partnership agreement with RNZ.
One of the most notorious moments of the presidency of Donald J. Trump has to be that visit he made to the Center for Disease Control (CDC) on March 6th of 2020. COVID-19 hadn’t even been named yet and the World Health Organization (WHO) hadn’t yet designated it a pandemic but we all knew that something very bad was happening. Cases had shown up in Washington state and California. The whole country was riveted by the plight of a cruise ship sailing off the West Coast with sick people aboard and nowhere to moor. The president was reportedly angry about the whole thing and was resisting dealing with it but finally agreed to travel to the CDC’s Atlanta headquarters for a photo-op to show his concern. It was one of the most astonishing presidential performances of all time:
Trump defends gutting the federal government’s pandemic preparedness over his first 3 years in office: “I just think this is something that you can never really think is going to happen.” pic.twitter.com/0fzOUSUBYE
You know, my uncle was a great person. He was at MIT. He taught at MIT for, I think, like a record number of years. He was a great super genius. Dr. John Trump. I like this stuff. I really get it. People are surprised that I understand it. Every one of these doctors said, “How do you know so much about this?” Maybe I have a natural ability. Maybe I should have done that instead of running for President.
Those exchanges illustrated the fundamental bind Trump was in from the beginning of the crisis. He wanted to “downplay” the virus, as he admitted to Bob Woodward around that time, but he also wanted to be the very stable genius who personally solved it. So he wavered back and forth throughout, some days saying the whole thing was just going away by itself and that his political enemies were talking it up to hurt his re-election chances. On other days he promoted snake oil cures, even offering advice to scientists on what they should be researching to treat the virus, apparently convinced that he had brilliant ideas that hadn’t been explored:
“I think a lot of people are gonna go outside all of the sudden” — Trump on DHS’s preliminary finding that the coronavirus doesn’t do as well in sunlight as it does inside pic.twitter.com/tmMCiCh3tq
He grew impatient with the medical professionals who kept telling him bad news and instead turned to the quack remedies like Hydroxychloroquine which people like Fox News personality Laura Ingraham were promoting. He listened to quack doctors like Fox News radiologist Dr. Scott Atlas, who would tell him what he wanted to hear. As his COVID task force coordinator Dr. Deborah Birx has testified before Congress, during the final months of his term, Trump completely lost interest in COVID altogether — at least until he came down with it himself.
However, towards the end, the vaccines were coming on line and Trump very much wanted to be given credit for them. He claimed over and over again that everyone said it would take five years but he made sure they were done in record time and nobody could have achieved that but him. In his first press conference after the election he said this:
The vaccines, and by the way, don’t let Joe Biden take credit for the vaccines. If Joe Biden… Joe Biden failed with the swine flu, H1N1. Totally failed with the swine flu. Don’t let him take credit for the vaccines because the vaccines were me and I pushed people harder than they’ve ever been pushed before. But the vaccines, there are those that says one of the greatest things. It’s a medical miracle. Don’t let anyone try and take credit for it.
As you can see, he was desperate to be given credit, as if he had personally spent that previous few months cooking up the vaccines in the White House kitchen. After all, he had a genius uncle who taught at MIT and all the doctors were astounded by his “natural ability.” As he put it, “the vaccines were me.”
We found out later that he and Melania Trump were among the first to be vaccinated while they were still in the White House, although they didn’t announce it or do what all the other politicians were doing by having cameras present to record the moment as a way to reassure the public that they were safe. Nonetheless, over the following months, Trump would from time to time talk up the vaccines, mostly as a way to talk up his part in it, and while always emphasizing that people “have their freedoms.” Last September, he even joined the freedom from sanity club himself saying that he probably wouldn’t get the booster when they became available.
His followers were not convinced.
After all those months of Trump downplaying the virus, refusing to wear a mask and otherwise encouraging his voters to see the mitigation strategies as a Democratic plot to bring him down, they have continued to chase snake oil cures and refused to get vaccinated. They don’t see the “medical miracle” of vaccines as a Trump triumph. They see it as a threat.
This week, Trump told another audience that he had received the booster after all — and he got booed. He took the opportunity to once again try to make the case that he should get credit and that his supporters are “playing into [the Democrats’] hands” by booing him.
“Take credit for it. What we’ve done is historic,” Trump told an audience over the weekend. “If you don’t want to take it you don’t have to, you shouldn’t be forced to take it, no mandates. But take credit because we saved tens of millions of lives, take credit, don’t let them take that away from you.”
He meant, “don’t let them take that away from me.“
Many people have seen those comments as Trump encouraging people to get vaccinated, but it really wasn’t and I doubt any of his followers saw it that way. In fact, he made it clear that he doesn’t care if they do it or not and that all that matters is that he is acknowledged as a big hero. In other words, his comment was really just more of his partisan politicization of the pandemic that’s gotten us into this mess in the first place.
And even if he did make an explicit pitch for people to get vaccinated, it’s unlikely that it would make a difference. Pollsshow that the resistance to vaccines is now baked into the MAGA psyche, with him or without him. He may have created this problem but he has no power to fix it and I imagine that’s intensely frustrating for him.
Trump yearns to be worshiped as the great leader who single-handedly saved the world but his followers are all inexplicably offering themselves up as human sacrifices instead.
In April 2008, Jonathan Agin’s 27-month-old daughter, Alexis, was diagnosed with DIPG, a rare brain tumor. Agin, then a civil defense lawyer in Washington, D.C., was dislodged from his comfortable life and dragged into the surreal world of a young cancer victim’s parent: the sleepless nights in the din of a hospital, the grueling clinical trials.
“I always had hope,” Agin said in a recent interview, though he knew most DIPG patients survive no more than two years after diagnosis.
Alexis lived for 33 months after her tumor was found. Toward the end of her life, she was unable to walk or speak. She died at 3:03 p.m. on Jan. 14, 2011.
“My knowledge back then of children with cancer was watching St. Jude and Ronald McDonald House commercials,” Agin said. The image of a “smiling, bald-headed kid living happily ever after” was cruelly misleading, he learned, when it came to intractable cancers like DIPG, short for Diffuse Intrinsic Pontine Glioma.
While children with a diagnosis like Alexis’ face almostinsurmountable odds, death rates for many childhood cancers have gone down, thanks to advances in treatment. But incidence rates — the number of cancer cases per 100,000 children — increased 43 percent from 1975 to 2018. While there’s no clear explanation, some experts suspect environmental contamination has played a major role.
“They cannot be explained by increased access to medical care or by improvements in diagnosis,” wrote Landrigan, director of the Program for Global Public Health and the Common Good at Boston College. His theory is that exposure in the womb or early childhood to chemicals is driving the trend. “Recognition is growing that hazardous exposures in the environment are powerful causes of cancer in children,” he wrote.
When it comes to drug development, children with cancer — defined as people under the age of 20 — have long been at the back of the line. There simply aren’t enough of them to inspire massive investment. In 2018, the most recent year for which complete data is available, 15,178 children in the United States were diagnosed with cancer and 1,841 died, according to the Centers for Disease Control and Prevention. By comparison, 1.7 million adults were stricken and 599,265 died.
Now comes the realization that some or many of the 86,000 chemicals used at one time or another in the U.S. may be having an outsize effect on the very young. Few of those chemicals have been tested for safety.
“The American public loves treatments, loves magic fixes,” Landrigan said in an interview. “The rising incidence is not a good-news story. There are no heroes.”
Links Between Environment and Cancer
In April 2010, thePresident’s Cancer Panel, an advisory group created by Richard Nixon in 1971, issued agroundbreaking reporthighlighting what it called the “growing body of evidence linking environmental exposures to cancer.”
The panel concluded that “the true burden of environmentally induced cancer has been grossly underestimated. With nearly 80,000 chemicals on the market in the United States, many of which are used by millions of Americans in their daily lives and are un- or understudied and largely unregulated, exposure to potential environmental carcinogens is widespread …. The American people — even before they are born — are bombarded continually with myriad combinations of these dangerous exposures.”
A co-author of the report was Dr. Margaret Kripke, who founded and chaired the Department of Immunology at The University of Texas M.D. Anderson Cancer Center in Houston. The panel had already looked at lifestyle factors, such as nutrition and smoking, and turned its attention to the environment because of public interest in the topic, Kripke, now retired, said in an interview.
“I was not that enthusiastic about this in the beginning,” she said. “It was controversial, unclear what we’d advise the public to do.”
Kripke’s opinion changed as she worked on the report in 2008 and 2009. “It was truly the most eye-opening experience for me,” she said. “I learned how little attention had been paid to this issue for a very long time.”
That inattention comes in part because “childhood cancers still make up only 1 percent of the cancer diagnoses in the U.S.,” said Dr. Philip Lupo, an associate professor at Baylor College of Medicine in Houston and a genetic epidemiologist at Texas Children’s Cancer and Hematology Center. “That creates a challenge for epidemiologists, who often need large sample sizes.”
Lupo and a colleague at Baylor, Dr. Michael Scheurer, have begun collecting biological specimens, such as saliva samples and primary teeth, from newly diagnosed patients and administering questionnaires to their parents in hopes of identifying novel risk factors for cancer development.
“As we see this explosion in environmental chemicals in human populations, it’s entirely likely they’re playing an important role in the increased incidence of childhood cancer,” Lupo said. Some, such as benzene, a solvent and an ingredient in gasoline, have been shown by occupational and/or animal studies to cause DNA damage, a precursor to the disease.
It’s unlikely genetics are behind the rising numbers, Lupo said, “because genetics don’t work that quickly.”
Congress created a body to investigate possible connections between chemical exposures and illness as part of theSuperfundlegislation in 1980. But theAgency for Toxic Substances and Disease Registry, part of the CDC, has never achieved widespread credibility.
In 1992, the Environmental Health Network and the National Toxics Campaign Fund released areportaccusing the agency of conducting poorly designed studies “used by polluters and government officials to mislead local citizens into believing that further measures to prevent toxic exposures are unnecessary.”
That criticism is still valid, said Stephen Lester, science director at the Center for Health, Environment and Justice, a research and advocacy organization in suburban Washington, D.C. The disease registry, known as the ATSDR, relies on existing data — generated, for example, by a state environmental agency — that is often incomplete and of little value for assessing health risks.
“The conclusions are always limited by the data,” Lester said. “Even if the agency could determine that a health cluster exists — and I’ve seen them do that maybe two times out of hundreds of cases — they cannot determine what’s causing the cluster.”
In an emailed statement to Public Health Watch and the Investigative Reporting Workshop, the CDC said, “While we know that chemical exposures can contribute to a variety of health issues and we continue to learn more about these pathways, determining a causal relationship from community-based chemical exposures to specific cases of cancer is rare.”
The ATSDR is being stretched thin, having seen its “purchasing power eroded by relatively flat funding levels despite increasing demand for support in responding to environmental exposures,” the statement said.
The agency received $4.5 million from Congress in recent years to update itsguidelinesfor investigating cancer clusters. The money came from the Strengthening Protections for Children and Communities from Disease Clusters Act — better known as Trevor’s Law, after Trevor Schaefer, who was diagnosed with medulloblastoma, a form of brain cancer, when he was 13 and living in McCall, Idaho, a small town north of Boise.
Schaefer and his mother, Charlie Smith, believe his illness was triggered by waste from an abandoned mine that wound up in the lake that supplied McCall’s drinking water. Five children in the town of 1,700 developed brain cancer within nine months of Schaefer’s diagnosis in 2002, but state health authorities said they found no evidence of a cluster.
Smith won the ear of then-Senator Barbara Boxer, D-California, who introduced Trevor’s Law in 2011. The bill languished and was finally signed into law by President Barack Obama in 2016. Schaefer said he’s grown increasingly impatient with the ATSDR’s failure to finish updating the guidelines in the five years since.
“While the federal government drags its feet and fritters away essential funding, our children are dying,” he wrote in an email to Public Health Watch.
The CDC said it has been using the funds to review the scientific literature, convene an expert scientific panel to discuss best practices and meet with community members and organizations to hear their concerns.
“Concurrent with efforts to update the guidelines are projects aimed at making county-level cancer rate data more readily available and a pilot effort to determine the utility of electronic health records to provide more timely cancer surveillance data,” the agency said.
In an interview, Schaefer, who runs theTrevor’s Trek Foundation, said, “We’re frustrated. When we talk to parents around the country, they’re getting frustrated. It doesn’t seem like it should take this long.”
Chemicals Uncontrolled
In 1942, the Industrial Hygiene Foundation of America presciently advised, “Every new chemical or product should be investigated as to its toxicity before it is prepared in large amounts and released to the public.” Twenty years later, in her book Silent Spring, biologist Rachel Carson warned about the overuse of DDT and other pesticides. “If we are going to live so intimately with these chemicals, eating and drinking them, taking them into the very marrow of our bones — we had better know something about their nature and their power,” she wrote.
President John F. Kennedy read excerpts of the book in The New Yorker and was so shaken he established a special panel to investigate Carson’s dire predictions. The panel’s report in May 1963 validated Carson’s findings and bolstered her credibility, which had come under fierce attack by the chemical industry.
“Silent Spring” generated momentum for the creation of the Environmental Protection Agency in 1970 and the phaseout of DDT. But the chemicals kept coming. By 1976, the year Congress passed theToxic Substances Control Act(TSCA) in an attempt to require safety testing, more than 60,000 of them were on the market. They were grandfathered in — assumed to be safe unless the EPA could demonstrate otherwise.
This proved to be too great a burden. The EPA has restricted only a handful of chemicals that were in commerce before 1976, including certain forms of asbestos, hexavalent chromium, dioxin-contaminated wastes and the paint-stripper methylene chloride.
Congress amended the control act in 2016 in part to shift the burden of proof from the EPA to chemical manufacturers to demonstrate new chemicals are unlikely to present “unreasonable” risks to human health or the environment before being allowed onto the market. During the Trump administration, however, new-chemical reviews by the agency were undermined by unrealistic assumptions that made substances appear safer than they probably were.
“Reviews of existing chemicals were also undermined by tenuous assumptions and illegal exclusions of certain sources of exposure, including environmental releases — of particular relevance to fenceline communities,” said Dr. Jennifer McPartland, a senior scientist with the Environmental Defense Fund.
The Biden EPA has worked to repair the damage but is still way behind. As of August, the agency’sTSCA inventoryhad climbed to 86,607 chemicals, 41,953 of which were considered “active” — manufactured or processed in recent years.
“EPA has to assess the risk of each and every one of those (active) chemicals, but it’s doing so at about 20-something a year,” McPartland said. Eachrisk evaluationis supposed to take 3 to 3½ years.
The math — nearly 42,000 chemicals and only 20 reviews a year — doesn’t bode well for public health.
“It’s the reality of a lack of regulation for decades,” McPartland said.
On top of all this, the EPA must assess new chemicals before they go on the market. The agency says it has finished 3,394 of these assessments since TSCA was amended, though not every assessment results in a requirement to test. McPartland said this program is also flawed. It’s needlessly opaque, she said, and its managers accede too often to companies’ demands for quick decisions.
In a Junepress release, the EPA said it had taken steps to bolster risk evaluations under way on 10 high-priority existing chemicals, including methylene chloride and 1,4-dioxane, a solvent found in paints, cosmetics, detergents and other products that has contaminated drinking water in some parts of the country. The agency said it would take into consideration “exposure pathways,” such as air and water, that had been disregarded by the Trump administration. The aim is to “restore public trust, provide regulatory certainty, and, most importantly, ensure that all populations that may be exposed to these chemicals are protected,” the EPA’s assistant administrator for the Office of Chemical Safety and Pollution Prevention, Michal Freedhoff, was quoted as saying.
In a written statement responding to questions from Public Health Watch and the Investigative Reporting Workshop, the EPA said it found “risks across many uses of these chemicals and will be proposing rules to protect against these risks beginning in 2022.” The agency said it has begun working on the next 20 evaluations.
The health impacts of cancer-causing chemicals land heaviest on low-income communities and communities of color, said Nsedu Obot Witherspoon, executive director of the Children’s Environmental Health Network. In such places “people who are doing all the right things — you know, taking care of their children the best they can and sending them to school and working hard” — face carcinogenic exposures from industrial facilities, heavily traveled highways and other polluting sources.
Witherspoon was born in 1975, the year childhood cancer incidence began rising. “That shows you right there it’s not genetics only,” she said. “There’s something else happening that is making young, young children predisposed. Childhood leukemia and certain brain cancers and tumors and whatnot are very much, sadly, related to certain levels of exposure. When you look at young children, they’re not smoking, they’re not drinking.”
Some in the private sector aren’t waiting for government intervention. In 2013, two students at theHelen R. Walton Children’s Enrichment Centerin Bentonville, Arkansas, were diagnosed with cancer. The illnesses were determined to be non-hereditary, and suspicion fell on chemicals the children might have ingested, inhaled or absorbed in their daily lives.
“It made us think twice about what we could be doing better,” said the center’s executive director, Michelle Barnes. “I was just horrified to hear about what is in our furnishings and carpets and things like sealants and non-stick cookware.”
The campus, which opened in 1982, was already marked for replacement. After the students’ cancer diagnoses, Barnes, other members of the center’s leadership team and its board of directors were determined to do things differently. New York-basedLTL Architectswas deemed to have the right sensibility and was hired in 2016. The new, $18 million campus opened in May 2019 with a 50,000-square-foot building that houses 244 students ages 5 and younger.
“We eliminated or significantly reduced exposures to six major classes of chemicals,” Barnes said, including a group of “forever chemicals” known asPFAS. Food is no longer stored in plastic bowls covered with plastic wrap, which can leach hormone-disrupting phthalates and bisphenol-A. Instead, it’s kept in stainless-steel bowls with lids made of medical-grade silicone. Teethers are natural rubber, not plastic.
Twelve million children 5 or younger are in some form of child care in the United States. Barnes said she’s heard from parents, school administrators and developers interested in replicating what the Children’s Enrichment Center created.
“We want to use this as a model for the early-childhood industry as a whole,” she said.
Children “Fall Through the Cracks”
For the foreseeable future, thousands of children will continue to be diagnosed with cancer each year and require treatment. But unless the drug-development process undergoes a significant transformation, they will remain a lower priority than adults.
Promising therapeutics for children have a difficult time moving from concept to commercial viability, said Vickie Buenger, president emeritus of theCoalition Against Childhood Cancerand mother of Erin Buenger, who died of neuroblastoma at age 11 in 2009.
“The children fall through the cracks because it’s tough to develop drugs for very small markets,” said Buenger, a business professor at Texas A&M University. The Food and Drug Administration has approved hundreds of cancer drugs, she said, but only six were developed with children in mind.
This disparity forces children to endure a “blast furnace of toxicity” during treatment with drugs designed for adults, she said. “They have to live with the side effects of such harsh treatment for decades.”
Uplifting survival stories create a sense of complacency, said Agin, who left his law practice after Alexis died to lead the nonprofitMax Cure Foundationand later start his own organization,Prep4 Gold. “When the messaging is, ‘Look how great we’re doing,’ that drives the lack of haste in developing new therapies,” he said.
And survival doesn’t guarantee a normal life. Many childhood cancer victims develop new strains of the disease or suffer other health problems, some related to the treatments themselves. Trevor Schaefer said he suffers from tinnitus in his right ear, double vision, hearing loss, post-traumatic stress disorder and depression almost two decades after his brain-cancer diagnosis.
A National Cancer Institute spokesman did not respond to written questions intended for one of its pediatric cancer experts. Instead, he referenced a Septemberblog postby institute director Dr. Norman Sharpless, who touted the progress that has been made. Treatments have become more precise, leading to better outcomes, Sharpless wrote. Today, for example, roughly 90% of children diagnosed with acute lymphoblastic leukemia are cured; a half-century ago the disease was almost always fatal.
Responding to lobbying by the Coalition Against Childhood Cancer and other groups and individuals, Congress has tried to improve the odds for children with hard-to-treat tumors, passing thePediatric Research Equity Actin 2003, theCreating Hope Actin 2011 and theResearch to Accelerate Cures and Equity for Children Actin 2017. The bills incentivized, to varying degrees, drug development for pediatric cancers, though one big loophole had to be closed.
The legislation has shown “the beginnings of value,” Buenger said. All six of the child-focused oncology drugs approved by the FDA came into use after the bills were passed.
Gregory Reaman, a pediatric oncologist and associate director for oncology sciences at the FDA’s Center for Drug Evaluation and Research, cautioned that there are still “major challenges to cancer drug development in children because many of the cancers that are most difficult to treat and that remain as major problems from the standpoint of not having effective therapies are driven by molecular abnormalities that are very, very different from the molecular abnormalities that cause adult cancers.
“I think kids are at the back of the line because the laws have not allowed them to be at the front of the line, where they belong,” Reaman said. “So, that is now changing, and we’ll have to see if the change in the laws actually does live up to the promises.”
Peter Adamson, who leads cancer drug development at Sanofi, a global pharmaceutical company, said researchers’ understanding of childhood cancer has advanced, especially over the past decade, “and that understanding is now helping to drive research.”
Still, he said, cancer remains “the leading cause of death from disease” in children.
“I think the community continues to look for the right balance of requirements and incentives to help catalyze drug development,” Adamson said.
Buenger acknowledged the work of “good actors” in the private sector. In November, for example, a firm called Oncoheroes Biosciences Inc.announcedit had agreed to license a drug called volasertib, which shows promise in treating acute myeloid leukemia and rhabdomyosarcoma, a type of soft-tissue cancer, to Notable Labs Inc. The former will have the right to commercialize the drug for use on children, the latter for use on adults.
But Buenger isn’t ready to declare victory.
“It’s a process, and we don’t want it to be just performative,” she said. “We’re not going to be satisfied by people saying, ‘We’re trying.’”
Oro Governor Gary Juffa has called on Papua New Guinea’s Health and HIV/AIDS Minister Jelta Wong to present a paper recommending a “proper and transparent” procurement system for the Department of Health (DOH) to procure medicine and pharmaceutical drugs.
Juffa, who was a member of the Public Accounts Committee of 2019 that held an inquiry into the DOH procurement, supply and distribution process, said the recommendations were endorsed and approved by stakeholders and donor partners that supported PNG in the health sector.
“The recommendations for the procurement system were put together by the Special Parliamentary Committee for Public Sector Reform.
“After the inquiry the DOH did not take action in implementing the recommendations made by the committee,” Governor Juffa said.
He said that recommendations proposed a more transparent system to procure, distribute and supply medicines and pharmaceutical drugs.
“I urge Minister Wong to present this paper to the National Executive Council for consideration.
“It is in the best interest of the country and the people,” Governor Juffa said.
Attempts to get a response from Wong yesterday were unsuccessful.
Meanwhile, Borneo Pacific Pharmaceutical has been awarded a one-year contract worth K65 million to supply medical kits throughout the country.
Rebecca Kukuis a PNG Post-Courier reporter. Republished with permission.
More moves to tighten the New Zealand’s borders may be needed on top of the decision to delay the start of the self-isolation scheme for Australian travellers, a professor of public health says.
For those who had booked to come home to New Zealand from Australia from January 17, the government would work with airlines to ensure some MIQ space was available, Covid-19 Response Minister Chris Hipkins said at a media update.
Air New Zealand has already cancelled about 120 flights, mostly from across the Tasman, as a result of the changes.
The rapid spread worldwide of the omicron variant of covid-19 is the main reason for the policy rethink.
It is among changes announced today that include a vaccine rollout for five to 11 year olds from January and a reduction in the time to wait for booster shots — from six months to four months.
Public health experts welcome change
The changes are being welcomed by public health experts, with Professor Nick Wilson from Otago University saying that the delay in self-isolation was the most important.
He said temporarily turning down the tap on international travellers from countries with the worst omicron outbreaks (at least for two to three months) may also be needed.
New South Wales officials over the weekend noted omicron was now likely the dominant strain in the state’s third outbreak, in which today alone it recorded more than 3000 cases.
But Professor Wilson said the government may also need to:
insist on rapid antigen tests at the airport for international travellers coming into Aotearoa;
make more improvements to MIQ facilities in terms of ventilation and avoiding shared spaces such as exercise areas; and
re-design the alert level system so that it can rapidly eliminate any outbreaks of the omicron variant that arise in the community.
“While there is still a lot of uncertainty around the omicron variant, especially the risk of severe disease, it is wise to try to keep it out of NZ as long as possible and until more is known about this variant,” Professor Wilson said.
No clear evidence of lower severity
Dr Matthew Hobbs, a senior lecturer in public health at the University of Canterbury, said he was concerned that a recent study from Imperial College London showed no clear evidence that omicron had lower severity than delta.
“Though it will be disappointing for many, through reviewing and postponing current border reopening plans, New Zealand has bought itself some much needed time while it works out how much of a problem omicron could be — like the last time we closed the Trans-Tasman bubble,” he said.
“It also provides us with a few more crucial months to get the booster shots up and roll out the paediatric vaccines.”
Dr Hobbs suggested the vaccination requirement for arrivals could be raised to three doses to reduce the risk of Omicron coming to New Zealand.
“More broadly, we also need to shift our domestic focus to a global perspective. The root of this issue is that the world isn’t doing enough to stop the spread of covid-19,” Dr Hobbs said.
“Wealthy countries around the world continue to hoard vaccines. This ultimately gives the virus more opportunities to replicate and mutate.
“Omicron should act as the wake-up call to ensure worldwide equitable vaccine delivery before even more concerning variants emerge.”
Omicron would ‘reach NZ quickly from Australia’ Professor Michael Plank, from Te Pūnaha Matatini and the University of Canterbury, said the rapidly growing omicron outbreak in New South Wales and its spread to other Australian states meant it would almost certainly get into the community in New Zealand within weeks if the country went ahead with border reopening plans in January.
“Delaying reopening plans to the end of February gives us a chance to keep omicron out until the majority of adults have received their third dose of the vaccine,” he said.
“Increasing the MIQ stay to 10 days and shortening the pre-departure test period from 72 to 48 hours are sensible ways to reduce the risk of the highly transmissible Omicron variant leaking out of MIQ. Adding a requirement for a rapid test on the day of the departure would be a useful extra measure.
“Hopefully these measures will keep omicron contained at the border. But if omicron does find its way into the community, the government has said it intends to use the red level of the traffic light system to try and control its spread.
“It’s unlikely this would be sufficient to prevent rapid spread of the variant if community transmission became established.
“Rolling out booster doses as quickly as possible is therefore essential to minimising the risk that omicron overwhelms our healthcare system.”
Hipkins also noted in the announcement today that the variant would spread quickly if it was in the community, and that public health advice suggested that soon every case coming into our border will be the omicron variant.
28 new covid-19 community cases The Ministry of Health reported today there are 28 new cases of covid-19 in the community, and no new omicron cases in Managed Isolation and Quarantine (MIQ).
In a statement, the ministry said of the new cases, 21 were in Auckland, five in Bay of Plenty, and two in Taranaki.
There are 57 cases in hospital, 10 in North Shore, 25 in Auckland, 19 in Middlemore, one in Northland, and two in Waikato. Seven cases are in ICU or HDU (one in North Shore; two in Auckland; three in Middlemore, one in Northland).
The ministry has also revealed that a recent returnee who left Middlemore Hospital without discharge, after being transferred from MIQ, also took their young child with them.
The child was transferred in the ambulance with the parent because it meant they could not be left unattended in managed isolation due to their age.
Police are currently investigating the incident which happened early on Monday morning.
This article is republished under a community partnership agreement with RNZ. The public health comments in this report were put together by the Science Media Centre. Professor Michael Plank is partly funded by the Department of Prime Minister and Cabinet for research on mathematical modelling of covid-19.
The Waitangi Tribunal has released a scathing ruling of the New Zealand government’s covid-19 response and vaccine rollout, saying Māori were put at risk.
The tribunal held an urgent hearing early this month, and released its findings today.
The tribunal says cabinet’s decision to go against official advice and not prioritise Māori in the vaccine rollout breached the Treaty principles of active protection and equity.
The government has said it instead opted for a whānau-centred approach.
The tribunal, in its report, said it could not understand why it would go for this against all expert advice.
While accepting a shift to the traffic light system was necessary, it found the rapid transition put Māori at risk.
The decision also put Māori health providers under extreme pressure on limited resources — pressure created by a delayed rollout, and years of chronic underfunding by the state.
It also said the Crown did not consistently engage with Māori to the fullest extent practicable on its pandemic response, a breach of the principle of partnership.
Better support recommended
It recommended better ethnicity data collection, better resourcing and support for Māori providers and communities, and a more equitable rollout for booster shots and paediatric vaccines.
Māori Council national secretary Peter Fraser described the Waitangi Tribunal report as “vindication”.
Fraser told RNZ Morning Report it was a strong ruling that showed the Crown had to uphold its Treaty obligations during a pandemic.
“We want to give credit to the tribunal, they took urgency.”
He said the “exceptional report” of more than 140 pages was put together in a couple of weeks before Christmas.
“It’s absolutely vindicated the Māori Council.”
He said he expected a difference in the paediatric vaccine rollout and booster programme.
Hopeful about new Māori Health Authority
“We are hopeful about the Māori Health Authority and we wish it was up and running now.”
Interim Māori Health Authority chief executive Riana Manuel … “we expend a lot of our time getting our people out of that misinformation mode.” Image: Andrew McRae/RNZ
Interim Māori Health Authority chief executive Riana Manuel said the report’s findings were not surprising.
She told Morning Report that she had been on the frontline during the pandemic, vaccinating and swabbing communities for nearly two years.
“We knew that if we didn’t prioritise Māori, we were going to be having to do what we’ve done for the last five months, which is try and get our people back online to getting them vaccinated.”
She said Māori were exposed to lots of misinformation while they waited for access to the vaccine, which had increased hesitancy.
“The problem is, though, like everybody else, we expend a lot of our time getting our people out of that misinformation mode and getting them back into those clinics.
“If we can learn to take the politics out of health and actually focus on what health requirements are … it’ll bring us back to what we need to do, what the right thing is to do.”
This article is republished under a community partnership agreement with RNZ.
With the emergence of the highly transmissible Omicron variant, the United States is now averaging over 130,000 newCOVID-19 cases a day, and health officials warn the U.S. could see a million new cases a day by February. We speak with health expert Dr. Carlos del Rio, who says that vaccination complemented by booster shots is the best defense against severe illness. “Everybody’s going to get infected. You’re going to be exposed to this virus because it’s essentially going to be everywhere,” says del Rio.
TRANSCRIPT
This is a rush transcript. Copy may not be in its final form.
AMYGOODMAN:President Biden is preparing to address the nation Tuesday about the government’s efforts to combat theCOVID-19 Omicron variant, which is rapidly spreading across the United States and the world. The U.S. is now averaging over 130,000 newCOVIDcases a day, nearly double the numbers of nearly a month ago. New York state has set new dailyCOVIDrecords on each of the past three days. OutgoingNIHDirector Dr. Francis Collins warned the nation could see a million new cases a day by February.
The new surge has led to many schools halting in-person classes and the postponement or cancellation of a number of professional sporting and entertainment events. Long lines forCOVIDtests were seen in many parts of the country ahead of the upcoming holiday weekend.
Despite the new surge, many scientists have expressed hope the Omicron variant will prove to be less dangerous than the Delta variant, especially for individuals who have received a booster shot.
Earlier today, Moderna announced its own internal studies show its vaccine booster considerably increases antibody levels against the Omicron variant.
Dr. Anthony Fauci spoke on NBC’sMeet the PressSunday. He said Omicron was raging through the world.
DR.ANTHONYFAUCI:The one thing that’s very clear, and there’s no doubt about this, is its extraordinary capability of spreading, its transmissibility capability. It is just, you know, raging through the world, really. And if you look even here in the United States, you have some regions that start off with a few percent of the isolates that are positive now going up to 30, 40, in some places 50%. So, yes, there is this issue of whether or not it is or more or less severe. The information we’re getting from our South African colleagues still suggests that when you look at it totally, the hospitalization-to-case ratio is less than with Delta. There seems to be less durability of symptomatology, less requirement for oxygen. But you’ve got to be careful. That might be due really to the fact that their population has so much experience with prior infections that it might be underlying immunity that’s making it look like it’s less severe.
AMYGOODMAN:We go now to Atlanta, Georgia, where we’re joined by Dr. Carlos del Rio, distinguished professor of medicine, epidemiology and global health at Emory University, also the international secretary of the National Academy of Medicine and the former executive director of the NationalAIDSCouncil of Mexico.
We welcome you toDemocracy Now!, Dr. del Rio. Why don’t you start off by explaining what Omicron is, how serious it is for this country and around the world, and this issue of its incredible infectiousness, but, on the other hand, whether in fact it makes people as sick as the Delta variant?
DR.CARLOSDELRIO:Well, good morning. And first of all, let me just say that this has been a horrendous pandemic, right? We’re now into our second year, we’re going to be starting our third year, and there really appears to be no end in sight. This virus has thrown to us a variety of different, I would say, curveballs at every step of the process.
We developed vaccines. The vaccines were initially developed to combat the original strain, the Wuhan strain. And then, over the course of the pandemic, we have seen different strains evolve that have been quite serious, first the Alpha strain and now the Delta strain and now the Omicron strain. The Delta strain is still a major problem globally and here in the U.S. I mean, the great majority of hospitalizations cases and deaths in our country continue to be caused by the Delta strain. But we’re seeing the Omicron strain emerge and becoming the dominant variant in the next several weeks.
What is happening? Well, this virus is a respiratory virus, and it’s anRNAvirus that, as it reproduces, as it’s multiplying, is producing mistakes. And some of those mistakes, those mutations, benefit the virus, and others don’t. The ones that we worry about is mutations that increase transmissibility, that increase clinical severity or that increase what we call immune evasiveness, i.e. the ability of the virus to evade our immune system either from prior infection or from vaccine-induced immunity. When a virus has some of those characteristics, theWHOcalls it a variant of concern.
The most recent variant of concern is actually Omicron. And what Omicron has, it appears to be — we’re learning. You know, we’re still learning. But it appears to be much more transmissible than Delta. Delta was already more transmissible than the original strain. The original strain had what we call a reproductive number of 2.5 to 3. What that means is that one person would infect two-and-a-half or three, and each one of those will infect two-and-a-half or three. If you did that 10 times and you did it in an immune population, you would have about a little bit over 9,000 people infected. When we go to Delta, Delta appears to be having an R naught of about six to eight. That means that one person infects six; each one of those infects six. If you put that into a naive population, after 10 cycles of transmission, you’d have 30 million people infected.
Well, Omicron appears to be two to three times more transmissible than Delta, so that would put Omicron in the neighborhood of measles, which has an R naught of about 15 to 18. And with an R naught of 15 to 18, everybody is going to get infected. You’re going to be exposed to this virus because it’s essentially going to be everywhere. And if you’re going to be exposed to this virus at this point in time, you’re better off if you’ve been vaccinated and if you’ve been boosted than if you’re not, because if you haven’t been vaccinated, if you haven’t been boosted, you will get infected. Even if you’ve been vaccinated, you have a chance of getting infected.
As far as clinical severity, I will just say that I agree with Dr. Fauci: It’s too early to talk about whether it’s more severe or less severe. But even if it’s less severe, if the numbers are really, really high, we still may see a lot of people in the hospital, simply because it’s a numbers issue, right?
AMYGOODMAN:You have the South Africa numbers, and many are saying perhaps they’re saying it’s less severe there because it’s a much younger population, and Britain is reporting something different. But I wanted to ask you about — on television, on all the networks, you know, you have the experts repeating what has to be done here — the basics. You’ve got to test. You’ve got to vax. You’ve got to wear a mask, socially distance and be extremely careful. But what’s not added to that list, repeatedly, is this issue of vaccinating the world. What has Omicron taught us about — it’s not just a matter of altruism that you want people to be as safe as perhaps people are in the United States, though many who are unvaccinated are not safe, but that if someone is unsafe somewhere, you are unsafe here?
DR.CARLOSDELRIO:Well, I think we’ve seen this over and over. The variants — Omicron emerged probably in South Africa. Delta emerged in India. In areas of the world with low vaccination rate and high transmission, you’re going to see these variants emerge.
And I think you mentioned the right word. It is “vaccinating” the world, not giving vaccines. If we get vaccines to countries but we don’t, you know, develop, don’t have the infrastructure to get vaccines into people, you will then not have vaccination. We need to do a better job.
I’m surprised that up to now there’s still not national and international leadership to make this happen. We need, really, somebody in charge of making this happen at a global level. And we need coordination, because, you know, they — initially what’s set up was something calledCOVAX, andCOVAXessentially has failed, and it has failed because there hasn’t been support from the different nations, the different organizations. We continue to treat global vaccination as charity: “Well, we have these vaccines left over. We’re going to send them.”
You know, most recently we sent a bunch of vaccines, Johnson & Johnson vaccines, to Haiti, and we were very proud of that. Well, we did that, and, you know, the State Department made a big announcement about that. It was done the same day that theCDCsaid Johnson & Johnson is not a good vaccine. You know, at the end of the day, we’re contradicting ourselves, and our foreign policy on vaccines is not aligning with what the reality is and what needs to happen.
AMYGOODMAN:Ananalysispublished Sunday by theFinancial Timesfound wealthy countries have administered moreCOVIDboosters than the total number of all doses given so far in poorer countries. According to the countries, as defined by the World Bank, where it’s just under 11 shots per 100 people by any doses had been given to low-income countries, something like nearly 16 booster doses per 100 people were administered across the world’s 59 high-income countries, Dr. del Rio.
DR.CARLOSDELRIO:Yeah, no, that’s absolutely true. I mean, I think that the disparities in this world are being seen in vaccination. Rich countries are hoarding vaccines and are boosting and are doing things that, you know, is for their own benefit and the benefit of its citizens, but they’re not — they’re being myopic. They’re not seeing beyond their borders. And when you’re controlling a pandemic, you have to look beyond your borders. This is a global issue. And if we don’t have a global approach, we’re never going to beat this.
AMYGOODMAN:And then the issue of Medicare for All at home, whether this would have made, or could make for future healthcare in this country, a massive difference? And this might go also to the issue of the unbelievable lack of testing available. I mean, we’re here in New York City. The lines are around blocks everywhere for anyplace that is offering a test. That if you had Medicare for All, for example, there would be more preventative care, and this issue of whether tests should be available for free everywhere here?
DR.CARLOSDELRIO:I think you’re talking about important issues, but I think they’re a little bit separate from each other, right? Medicare for All may be one thing, but, again, this is not an issue of Medicare. This is an issue really about the government doing the right thing during a pandemic.
Setting up testing sites — you know, we’ve left a lot of things to the market. And, for example, rapid tests continue to be run by industry, by corporations that produce the tests and want to make a profit out of this. They should have been taken over by the government like we’ve seen in the U.K. and many other places. And basically, rapid tests ought to be available for everybody to go to the drugstore and the supermarket and buy for a reasonable price, not for the price that we’re currently paying. I mean, I bought some rapid tests yesterday to use in my family gathering, and I’m paying $25 for a package of two tests. That is simply something that most of the people in this country cannot afford. And I should have been able to go there and get them for under $5. But the reality is, for that to happen, the government should have stepped in.
We did it with vaccines, right? But imagine if the vaccine approach had been that of the rapid test approach, that the government said, “Well, you know, buy them and then submit a claim to your insurance company to get reimbursed.” Well, imagine if the vaccines had been the same way: “Well, get vaccinated, but you have to pay for it, and then you submit a claim to your insurance company to get reimbursed.” We would have never had the number of people vaccinated that we currently have in this country. The vaccines are — you know, we reached the number of vaccinations we reached in this country because the vaccines are available and are free. And that’s exactly what we needed to happen with rapid tests, but we haven’t done that. And I’m baffled that we haven’t done that.
AMYGOODMAN:Well, let me go to White House Press Secretary Jen Psaki, facing widespread criticism for her comments about making at-homeCOVIDtests available to all Americans.
PRESSSECRETARYJENPSAKI:Look at what we’ve done over the course of time. We’ve quadrupled the size of our testing plan. We’ve cut the costs significantly over the past few months. And this effort to — to push — to ensure insurers are — you’re able to get your tests refunded means 150 million Americans will be able to get free tests.
MARALIASSON:That’s kind of complicated, though. Why not just make them free and give them out and have them available everywhere?
PRESSSECRETARYJENPSAKI:Should we just send one to every American?
MARALIASSON:Maybe.
PRESSSECRETARYJENPSAKI:Then what — then what happens if you — if every American has one test? How much does that cost? And then what happens after that?
MARALIASSON:All I know is that other countries seem to be making them available in greater quantities for less money.
PRESSSECRETARYJENPSAKI:Well, I think we share the same objective, which is to make them less expensive and more accessible, right? Every country is going to do that differently. And I’m just noting that, again, our tests go through theFDAapproval process. That’s not the same process that it — it doesn’t work that way in every single country.
AMYGOODMAN:Dr. Carlos del Rio, your response?
DR.CARLOSDELRIO:You know, I think, you know, yes, they’ve increased test capacity, but the reality is it’s still not sufficient. So, you know, laudable efforts but not enough.
AMYGOODMAN:Well, I want to thank you so much for being with us. Dr. Carlos del Rio is distinguished professor of medicine, epidemiology and global health at Emory University, also international secretary of the National Academy of Medicine.
Coming up, President Biden’s Build Back Better plan appears to be dead, after Democratic Senator Joe Manchin surprises the White House and comes out against the plan to expand the nation’s social safety net and combat the climate crisis. He made the announcement on Fox TV. We’ll speak with one of the six congressmembers who voted against the infrastructure bill, saying, “If we don’t tie it to Build Back Better, Build Back Better will die.” Stay with us.
[break]
AMYGOODMAN:“El Rey” by Vicente Fernández. The Mexican singer recently passed away at the age of 81.
Fiji’s Health Ministry is concerned that people are not taking the new omicron variant of the coronavirus seriously.
Fiji reported two cases of the variant more than two weeks ago — both patients had arrived in the country from Nigeria on November 25.
Health Secretary Dr James Fong said more than 70 countries had reported cases of omicron and it was probably in most countries, even if it had not yet been detected.
He said if there was an outbreak in Fiji, it could again overwhelm the health system.
Dr Fong said vaccines alone would not get any country out of the crisis, and that nations must prevent the spread of omicron with mask wearing, hand washing, and social distancing.
“I anticipate that if we are looking at a third wave right now, based on what’s happening at the moment, we are looking at early next year — probably around the January to February period,” he said.
“We’re concerned that people are dismissing omicron as mild. Surely, we have learned by now that we underestimate this virus at our peril.
Risk of overwhelming health systems
“Even if omicron does cause less severe disease, the sheer number of cases could once again overwhelm unprepared health systems.
“Vaccines alone will not get any country out of this crisis. Countries can — and must — prevent the spread of omicron with measures that work today.
“It’s not vaccines instead of masks. It’s not vaccines instead of distancing. It’s not vaccines instead ventilation or hand hygiene. Do it all. Do it consistently. Do it well.”
Dr Fong also said the evidence suggested a small decline in the effectiveness of vaccines against severe covid-19 disease and death, and a decline in preventing mild disease or infection.
“If a variant is transmissible enough, stringent border and community measures will only delay the inevitable entry and spread of current and future variants of the covid-19 virus, especially as the omicron variant is also spreading into some of our travel partner countries,” Dr Fong said.
“To protect ourselves, our loved ones and our country, we must all get vaccinated when it is our turn.
“And even with our high vaccination levels, we must maintain covid-safe habits: mask wisely by carrying a well-fitted mask when you leave your home and wear the mask properly in public indoor spaces, public service vehicles and outdoor crowded spaces.
Sharp reminder for caution
“Open windows to improve ventilation; avoid poorly ventilated or crowded spaces; 2-metre physical distancing and ensure you are wearing a mask if you cannot maintain distance; cough or sneeze into a bent elbow or tissue, wash your hands frequently with soap and water or an alcohol-based hand sanitiser.
“The discovery of omicron is a sharp reminder to ourselves that the key to avoiding future restrictions and lockdowns is for us all to remain cautious about how we engage in the greater freedom we will enjoy.
“Whilst the easing of restrictions is needed to facilitate livelihoods, we must ensure that together with vaccination, we continue to observe our covid-safe measures and avoid contained spaces and crowds.”
Dr Fong said following the delta outbreak in Fiji, it was understandable that many would feel the urge to relax and celebrate now that case numbers were low, especially during the festive season.
“And many of us have let our guards slip. We are all human.
“But this must stop as vaccination and the Covid Safe measures are the only way to safely navigate our way through the pandemic while facilitating socio-economic recovery and well-being.”
19 new cases in community Dr Fong confirmed 19 new cases of covid-19 in the community.
This brings the total number of active cases to 116, including two cases of the omicron variant of the coronavirus, he said. Seven of the latest cases were recorded last Thursday while 12 on Friday.
Dr Fong said there were seven covid patients in hospital in critical condition.
He said with Fiji’s international open to tourists, the public is being urged to take Omicron seriously.
“The threat of cases coming in through our borders will always be there for as long as the word pandemic is applied throughout the world. And the only that we can protect ourselves is ensuring good adherence to our covid health measures.”
There are no deaths to report and the toll remained at 697, Dr Fong said.
“We have recorded 612 covid-19 positive patients who died from serious medical conditions they had before they contracted covid; these are not classified as covid-19 deaths,” he said.
“For this second wave, there have been 52,553 cases recorded, with 71 percent of the cases from the Central Division, 28 percent from the Western Division, and 1 percent of the cases from the Eastern and Northern Divisions.
“Our national 7-day rolling average is 5 daily cases calculated for 13 December 2021.”
Close to 92 percent of Fiji’s adult population is fully vaccinated, Dr Fong said.
He said 38,321 children aged 12-17 are also fully vaccinated against covid-19 while 57,697 have received their first dose.
This article is republished under a community partnership agreement with RNZ.
The doses include both the Pfizer — the main vaccine deployed in New Zealand — and AstraZeneca vaccines.
MidCentral and Hutt Valley have also reached 90 percent first doses for Māori, becoming the fourth and fifth district health board (DHB) areas to reach the mark.
However, nationally, the second dose rate for Māori remains at 77 percent.
Canterbury continues to lead the way overall, with 98 percent of eligible people having had a first dose and 94 percent being fully vaccinated.
New Zealand has a population of five million.
55 new community cases, 13 omicron cases in MIQ
The ministry reported 55 new community cases of covid-19 in New Zealand today and five more cases of the omicron variant in recent international arrivals.
The new omicron cases in MIQ take New Zealand’s total to 13.
Four of these cases remain in managed isolation. One person has now recovered and has been released.
The recovered case arrived from London via Singapore on December 7. This case tested positive on day one and was closely managed in MIQ, the ministry said in a statement.
The person was never in the community while infectious.
Of the new community cases, 41 are in Auckland, with the remainder spread between Waikato, Bay of Plenty and Taranaki.
This article is republished under a community partnership agreement with RNZ.
The COVID-19 catastrophe presents a challenge of planetary proportions. You would expect it would elicit a response drawing on all our skills, compassion and collective resources. But, as Andrew Smart, argues, we are seeing the opposite.
New Zealand’s longest covid-19 hospitalisation in Auckland and Northland during the first three months of the current outbreak was 61 days, and an overwhelming majority of patients were Māori or Pacific.
Figures from the Northern Region Health Coordination Centre (NRHCC) released to RNZ News under the Official Information Act (OIA) show 704 people with covid-19 were admitted to hospital between August 17 and November 18, 2021.
“There were 309 Māori patients, 295 Pacific patients, 36 Asian and the rest [64] were of other ethnicities,” Counties Manukau District Health Board chief executive Margie Apa said in the OIA response.
Responding to questions about the response in a statement, a Ministry of Health spokesperson said “protecting Māori and Pacific wellbeing has been an integral part of the ongoing covid-19 response”.
They said the ministry recognised the vulnerability of these communities, “especially given larger family sizes and complex health needs”.
They highlighted how the ministry had redirected $36 million to each of the Māori and Pacific health responses in this current outbreak.
“In addition to providing funding, we remain committed to working with a range of experts, providers, and partners to ensure our response continues to protect Māori and Pacific communities and keeps them safe from covid-19,” the spokesperson said.
‘Unfortunate but predictable’
National Māori Pandemic Group co-leader Dr Sue Crengle said the proportion of Māori and Pacific in the figures was unfortunate but “predictable, given what we know … about how Māori and Pacific communities and whānau are likely to be more vulnerable to transmission of the virus, and also more vulnerable to more severe outcomes”.
National Māori Pandemic Group co-leader Dr Sue Crengle … “we haven’t had a pandemic on this scale since 1918.” Image: RNZ
She said officials could have learnt and acted faster given the pandemic had been going for more than a year when this outbreak started. But she did note: “we haven’t had a pandemic on this scale since 1918”.
Crengle said there should have been “forward thinking” earlier on.
Apa said there were a total of 870 “patient events” – the difference between this number and the total patient count was because of things like patient transfers between hospitals.
The vast majority — 513 — were unvaccinated, with 124 people having had one jab, and 67 were fully vaccinated.
More than half of admissions (479) were for up to two days, compared with only 73 hospitalisations of 10 days or more.
However, 50 patients ended up in intensive care, seven of them being placed on a ventilator, and on 16 occasions people spent 10 days or more there – including two people who spent 950 hours there, which equated to almost 40 days.
Church deacon
One of those two patients would have been a 50-year-old man, who was a deacon at the Assemblies of God Church of Sāmoa and died in Middlemore Hospital in October.
A caveat of the data in this story was that some people had not been discharged by November 18 – the limit of the OIA request scope.
NHRCC forecasting of “specific hospitalisation predictions” only happened first on October 8, 2021 — more than two-and-a-half months into the outbreak — with the earliest predictions beginning November 9, 2021.
In a graph provided separately by the NHRCC communications team, there were at least three days where intensive care admissions met or were higher-than predicted between November 9 and December 10.
Overall hospitalisations in the same period were always below what NHRCC predicted. NHRCC predicted there would be just under 40 people in hospital in its catchment by 28 December.
Its “specific hospitalisation predictions” did not include modelling on the use of ventilators.
“The use of ventilators is a clinical decision made in response to a patient’s condition and while there are thresholds for use and pathways of care we have not modelled the expected use,” NHRCC said.
More hospitalisations In contrast to NHRCC, Te Pūnaha Matatini researcher and covid-19 modeller Professor Michael Plank said there had been more hospitalisations than originally expected.
He thought that was likely down to the fact people were being hospitalised “for a shorter stay” so “they have a relatively small impact on the number of beds”.
Dr Plank said intensive care admissions were hard to predict and “to be honest, we haven’t spent a lot of time trying to model that”.
RNZ is awaiting national figures which have been requested from Ministry of Health.
An OIA request to the ministry for national figures was transferred to the NRHCC, a collective of the Northland and Auckland District Health Boards working together on the covid-19 response. National figures have been asked for again.
This article is republished under a community partnership agreement with RNZ.
Mental illness has historically dwelt in the shadows of the global health and development agenda and only recently has moved from the margins to become a central priority in research and policy. Mental disorders account for 30% of the worldwide non-fatal disease burden and 10% of the overall disease burden, including death and disability, and the cost to the global economy is estimated to reach as high as USD 6 trillion by 2030. Large middle- and low-income countries like Indonesia struggle with a plethora of challenges in delivering adequate mental health care to its 270.2 million citizens. Centralised funding for Indonesian mental health is only 1% of the national health budget; health expenditure is around 3% of GDP. National health programming such as Indonesia Sehat, the incorporation of mental health into primary care basic standards and voluntary contributions from provincial budgets does provide some additional resources. However, there is a severe shortage of mental health personnel, treatment and care facilities, especially outside the island of Java.
Estimations based on the 2018 Basic Health Survey (RISKESDAS) indicate there are 450 000 families in Indonesia with at least one member diagnosed with schizophrenia; given the high level of stigma against mental illness and psychosocial disabilities, we suggest this number is much larger. Many of these people are subject to human rights abuses, being left to languish in cages, stocks or chains referred to as Pasung. Human Rights Watch estimated that 12,800 people were experiencing Pasung at the end of 2018. Over 26.23 million people, more than the entire population of Australia, suffer from clinically relevant symptoms of anxiety and depression and 16.33 million likely meet the diagnostic criteria for a depressive disorder.
Although there is a shift to community-based outpatient models of care, Indonesia’s 48 mental hospitals and 269 psychiatric wards in general hospitals are still the primary sources of care. There are just over 1000 registered psychiatrists, 2000 clinical psychologists, 7000 community mental health nurses, 1500 mental health trained GPs and 7000 lay mental health workers unevenly distributed across the archipelago, (Ministry of Health Regulation on Pasung Management, 2017; Pols, 2020). Need outstrips supply, with eight provinces without a mental hospital: three of these hospitals without a single psychiatrist. Less than half of all primary care centres and only 56% of government district hospitals are equipped to handle mental health cases. Fortunately, there are many passionate and committed mental health personnel, government officials, academics, consumer group founders and mental health advocates who are working tirelessly to implement the vision embodied by the 2014 Indonesian Mental Health Law. Our webinar for World Mental Health Day is a small sample of these extraordinary individuals, who will share their experiences in Indonesian mental health.
Dr Nova Riyanti Yusuf, a psychiatrist, legislator (member of the DPR from 2009-14 and 2018-19), novelist, scholar, television personality and activist, was one of the driving forces behind the 2014 mental health law. She will talk about the ongoing journey of the mental health law, what its vision is for Indonesian mental health and the current state of implementation at the grass roots level. Professor Hans Pols, a renown psychiatric historian based at University of Sydney and expert on Indonesian mental health will then take us through a brief history of Indonesian Psychiatry and will talk about some of the emerging trends for the future of the profession across the archipelago. Anto Sg,Pasung survivor and current recipient of an Australia Award currently studying a Master of Health Promotion at Deakin University, will share his person experience of Pasung and introduce the survivor or consumer group movement in Indonesia. Dr Erminia Colucci currently based at Department of Psychology, Middlesex University, UK will is working with the Center for Public Mental Health (CPMH), Psychology at the University of Gadjah Mada and Ade Prastyani, GP and scholar on traditional healing approaches to mental health. We will show a short exert of their upcoming film produced by their collaborative Together4MentalHealth. After which, CPMH director, distinguished academic and clinical psychologist Dr Diana Setiyawati will provide us with a current update on community mental health initiatives in the age of Covid19. Aliza Hunt, Centre for Mental Health Research PhD Candidate and Endeavour Scholar at the ANU is chairing the session.
New Zealand’s first case of omicron has been identified, as the country hit its 90 percent full vaccination target today, children between five and 11 will be able to get the vaccine, and protesters marched on Parliament demanding an end to vaccine mandates and restrictions.
The protest — organised by Destiny Church leader Brian Tamaki’s Freedom and Rights Coalition — took place the day after Parliament rose for the year.
Police had to close off Willis Street and part of Lambton Quay.
Metlink services which led to the Lambton Quay Interchange were diverted while the protest was underway.
Protesters held a banner reading “Labour Must Go”.
Parliamentary Security fenced off the forecourt to prevent any protesters entering the Parliament building, and staff were warned to stay away from the windows.
About 50 police officers stood on the forecourt.
The numbers
There were 91 new cases of covid-19 in the community today.
Two are in Northland, seven are in Waikato/King Country, 10 in Bay of Plenty, one in Rotorua, 16 in Taranaki and the remaining cases in Auckland.
The new cases in Northland are in Ruakākā.
In Taranaki, the new cases are in Eltham, but all but one of them were reported yesterday.
Fifty eight people are in hospital, with four in either ICU or a high dependency unit.
A wastewater sample collected from Gisborne on Tuesday detected the virus.
This is the sixth positive wastewater result for Tairāwhiti in recent weeks, indicating there may be unknown cases in the community.
This article is republished under a community partnership agreement with RNZ.
Spot checks are happening on roads out of the city, at the airport, and at two new checkpoints in Northland.
The new checkpoints were set at Uretiti on SH1 and on SH12 at Maungaturoto, for northbound traffic only.
Anyone can leave Auckland with proof they are double vaccinated or have recently tested negative for covid-19.
Transport operators will also be checking on passengers’ status.
Even with border restrictions in place, more than 2 million cars have passed through the northern and southern boundaries since the end of August, mostly carrying essential workers.
News reports said that 12,000 people were booked on Air New Zealand flights out of the city today.
In a statement, the ministry also reported that several members of a flight crew had been identified as close contacts of a omicron variant case in Australia.
“These crew members arrived in New Zealand last night and are in a MIQ facility, as per standard international air crew arrival procedure,” the statement said.
Of the new community cases today, 51 are in Auckland, 21 in Waikato, seven in Bay of Plenty and one in the Taupō district.
The ministry also announced an additional case in Canterbury today, which will be officially counted in today’s case numbers.
There are now 9890 community cases in the current outbreak. The number of active cases is 6863.
This article is republished under a community partnership agreement with RNZ.
A New Zealand nurse has been referred to a professional conduct committee by the Nursing Council after posting threats online against medical professionals involved in the national covid-19 vaccine rollout.
Multiple agencies are investigating after the registered Dunedin nurse posted a video to social media “declaring war” against covid-19 vaccinators and calling medical professionals taking part in the vaccine rollout her “enemies”.
Under the pseudonym Lauren Hill, the nurse posted a message to an anti-vax group on social media app Telegram.
In the video she said she was in a rage and called on the Prime Minister, the Covid-19 Response Minister and the Director-General of Health to “cease and desist” in the rollout of the vaccine to five to 11-year-olds.
RNZ can confirm the woman in the video is Dunedin nurse Lauren Bransgrove, who has been taking part in Voices for Freedom anti vax events in the southern city.
The Ministry of Health is aware of the matter and has said they were concerned.
Police, ACC and the Nursing Council are also aware of the post.
‘Resistance’ to monitor schools
In the message, Bransgrove called on fellow antivaxxers — referring to them as “the resistance” — to organise and prepare to monitor schools every day so they could attack vaccination buses when they turned up.
“We do everything we can to stand in the way of you injecting this poison into our children. We will rip the bribes from your hands, we will slash your tyres, and we will remove the poison from the truck. This is not inciting violence, this is inciting self-defence, especially for our youngest people,” she said during the two minute and 23 second long rant.
“So cease and desist now, because this is war. And to the doctors and nurses that are still allowing this to happen, that have seen what is happening in the hospitals and refuse to speak out, I do not consider you a colleague, I consider you an enemy.”
Screengrab of Lauren Bransgrove’s antivax rant on Telegram . Image: RNZ
Medsafe is currently assessing an application to administer Pfizer’s covid-19 vaccine to children aged 5-11.
The vaccine would be one-third of the dose of that administered to those 12 and older, of which more than 7.8 million doses have been given in New Zealand.
The vaccine has been deemed safe and effective by the vast majority of experts, both in New Zealand and globally.
‘Long covid’ symptoms
While the risk of serious covid-19 infection is far lower among children, covid-19 has been one of the top 10 causes of death of children aged five-11 in the US over the past 12 months.
A large study of children in the UK aged 11-17 also found as many as one in seven might still show symptoms of the illness three months after infection, commonly known as “long covid”.
So far, millions of doses of the vaccine have been administered to children aged 5-11 in the US.
Medsafe says it has completed its initial assessment of the application and has received a response to its request for additional information from Pfizer.
It intends to make a decision regarding approval this month.
Bransgrove lists her occupation as a clinical advisor for ACC.
Before that she spent 15 years working as a nurse, including a role as a theatre nurse in a private hospital for seven years.
She completed her training through Otago Polytechnic.
Multiple agencies investigating
A Ministry of Health spokesperson confirmed multiple agencies were investigating the video and its contents.
“The Ministry of Health is very concerned about this and is looking into this as part of a multi-agency approach,” the spokesperson said.
Police also confirmed they were making inquiries into the matter.
The Nursing Council confirmed it had referred the matter to a professional conduct committee.
Lauren Brangrove’s poster is visible in the right distance of an anti-lockdown protest in Dunedin’s Octagon on November 9 – with the slogan “Nurse of 20 Years My Body/Choice” written on it. Image: Tim Brown/RNZ
When a few thousand people marched onto Parliament grounds on November 9 with a mish-mash of gripes with government, Bransgrove took part in a similar but much smaller gathering in the Octagon in Dunedin.
Carrying a sign which read “Nurse of 20 years My Body/Choice”, she spoke to RNZ, but refused to provide her last name.
“I am a nurse who went to Otago Polytechnic, I spent many years in the operating theatre helping the people of New Zealand, I now work for a public agency which I will not name,” she told RNZ.
‘Many vaccine injuries’ claim
She went on to claim many vaccine injuries were being reported to ACC.
When asked how many vaccine injuries had been reported, she responded: “Well I don’t know exactly, but I know they’re being accepted”.
By November 27 ACC had received 1179 claims stemming from covid-19 vaccination treatment injuries.
Of those, 448 had been accepted and 260 declined with 471 yet to be decided.
Allergic reaction accounted for nearly half of the claims, with bruises and sprains the next most common injuries.
No deaths had been lodged with ACC.
To date Medsafe has said one death is likely linked to the covid-19 vaccine and has been referred to the coroner.
‘More going online’
When provided treatment injury numbers as these stood at the time, Bransgrove responded: “I don’t know the number but there’s a lot more going on online.”
“When you go on these groups online, because you can’t see any of this on the news because it is not reported, when you see real people with real injuries and real deaths, you’re going to have to start to wake up.
“This is not about health, this is about control, this is about totalitarianism,” she said.
She claimed she did not care if she lost her job as she believed she would look back on the time and find herself on the right side of history.
When asked why countries with high vaccination rates had low death rates from covid-19, she responded: “Tell me about Israel”.
At the time of the conversation, Israel’s daily case count was less than 10 percent of the peak of the delta outbreak (when 10,000 new cases were reported a day).
That decline in case numbers followed a successful and widespread booster programme in the country.
Israel now has a seven-day average of about 600 cases a day, while the average of daily deaths has been less than 10 since late October and now sits at about two deaths per day.
Many others ‘concerned’
Bransgrove told RNZ there were many others similarly concerned by the vaccine and terrified to speak out.
ACC moved this evening to distance itself from Bransgrove.
“We are urgently investigating this matter,” ACC chief executive Megan Main said in a statement.
“ACC in no way condones threats of violence under any circumstances.
“We have encouraged all of our staff to get vaccinated as the best measure to protect themselves and others against Covid-19. We have instituted a policy requiring all our staff to be vaccinated in order to be on any ACC site from 15 December.
“The opinions expressed in no way represent the views of ACC.”
Anti-vaccine posts removed
Bransgrove earlier told RNZ she worked from home five days a week and so would not be subject to the vaccination policy.
ACC would not comment on whether Bransgrove had been suspended.
Earlier today she removed anti-vaccine posts — including a threat against the Deputy Prime Minister — from her social media accounts.
Anti-vaccine group New Zealand Doctors Speaking Out with Science claimed it had the support of 105 doctors.
In contrast an open letter from doctors supporting covid-19 vaccination had more than 6500 signatures.
This article is republished under a community partnership agreement with RNZ.
Not a single tear was shed as 54 unclaimed bodies and 11 body parts were laid on top of each other in a single open grave dug out at the 9-Mile Cemetery in Port Moresby this week.
It was a rather undignified way to go for the corpses. What were once loved ones clearly had been forgotten — every single one of them.
But what was even sadder was the 9 bodies of children among the mass burial after six months had gone by with not a single family member coming forward to claim them.
A mass burial is unusual in Melanesian society such as Papua New Guinea, but without relatives collecting the bodies it had to be done.
Wrapped in plastic bags and put in standard plain box coffins, the bodies and body parts were taken to the cemetery from the Port Moresby General Hospital in two trucks.
The bodies have been at the mortuary and other makeshift storage containers.
The covid-19 situation in NCD also complicated matters for the hospital and the relatives of the deceased.
No time to waste
At the burial site, it was no time to waste for the morgue attendees as they unloaded the two truckloads containing the bodies and body parts and quickly lowered them stacked into the hole in the ground.
Port Moresby General Hospital director for medical services Dr Kone Sobi said the mass burial came into effect following several media announcements following the overwhelming burden at the morgue facility.
“We come from a Melanesian society and this kind of sending off our loved ones is not expected, however it has to be done,” Dr Sobi said.
“We had to go through due process as it takes time to comply with the processes to take place.
“The mass burial was for dead bodies that have been in the morgue since March, April and May this year.
“There were requests after the initial announcements for mass burial from relatives and friends of the deceased in the name list to reserve and claim their loved ones.”
He said the hospital allowed that process to take place and the period had lapsed.
An approved list
“We then provide the approved list from the coroner to the National Capital District Commission (NCDC) to conduct the mass burial.
“If the body is not claimed after two weeks, then this goes to the Coroner to give an authorisation and once it is authorised, the mass burial is carried out,” he said.
The mortuary is the function of the NCDC social services division and it is the responsible of the office of the governor who has appointed a contractor to carry out the mass burial and all the parties involved have allowed and assisted the hospital to carry out this exercise.
He said the usual costs for mass burial was about K90,000 (about NZ$38,000) because a mass burial is carried out on a quarterly basis during a year, so one mass burial costs about K30,000. However, for this year’s exercise, NCDC is responsible for the costs.
For these mass burials, there were 54 adult bodies, nine children and 11 body parts from individuals who have been involved in accidents and people who have had injuries resulting in amputation of upper and lower limbs.
This is a combination of two mass burials that were supposed to be carried out in the year.
Dr Sobi said that for this year, this was the first mass burial exercise to be carried out.
Grace Auka-Salmangis a PNG Post-Courier reporter. Republished with permission.
New Caledonia’s pro-independence parties say the French overseas minister’s visit in the next few days is unwelcome, describing it as “another provocation”.
Overseas Minister Sebastien Lecornu announced his trip as New Caledonia readies for Sunday’s third and final independence referendum after rejected pleas by the pro-independence parties to postpone it to next year because of the pandemic.
While the minister said he would outline details of the 18-month transition phase following the vote in upcoming talks in Noumea, the pro-independence parties have ruled out meeting him.
They said any negotiations will have to wait until after the French presidential election in April.
The customary Kanak Senate, which is a forum of traditional leaders, has now declared Sunday as a day of mourning for the victims of the pandemic and called on Kanaks not to vote.
Its president, Yvon Kona, has also appealed for calm so there would be no trouble on polling day.
An extra 2000 police and military personnel have been flown in from France to provide security across the territory.
Complaint that Lecornu flouted covid rules Meanwhile, a small pro-independence party has lodged a formal complaint against Lecornu in France after reports that the minister flouted covid-19 restrictions during his visit to New Caledonia in October.
The French investigative news site Mediapart reported that Lecornu had gone for drinks at a meeting with anti-independence New Caledonian politicians.
The complaint alleges that by breaking the rules he imperiled the health of others.
The ministry said the event was a work-related multilateral exchange.
It said in turn it intended to lodge a complaint against the party for defamation.
This article is republished under a community partnership agreement with RNZ.
As New Zealand gets ready for the festive season under the new traffic light system, the emergence of the omicron variant is a reminder this pandemic is far from over.
The new variant of concern is already fuelling a new wave of infections in South Africa and there is some evidence hospitalisations are increasing.
Omicron has already arrived in Australia and the question now is whether it will get to New Zealand during the summer holiday season and potentially affect plans for border openings.
New Zealand is currently planning to start opening its borders and allowing quarantee-free entry from early 2022, first to fully vaccinated New Zealand citizens arriving from Australia after January 16, and then for New Zealanders arriving from all other countries after mid-February.
There is already some discussion about whether this plan may have to be reviewed.
Omicron contains 32 mutations in the spike protein alone. These are mutations that may make the virus more transmissible and better at evading immunity. There is also some evidence to suggest it poses a higher risk of reinfection.
Other anecdotal evidence suggests more children are being hospitalised with moderate to severe symptoms with omicron.
However, it is still too early to draw any firm conclusions. Data over the next few weeks will help determine the variant’s full impact.
Data from the South African COVID-19 monitoring consortium show the impact of the Omicron variant. Graphic: SACMC Epidemic Explorer, CC BY-ND
Perhaps most importantly, delta also taught us that when new variants emerge, they do not stay in one place for very long.
So, how prepared is New Zealand?
FASTEST SURGE TO DATE—The #OmicronVarient is up swinging much faster in both new daily cases and positivity, than all previous waves in South Africa , according to @nicd_sa data illustrated by @jburnmurdoch. This supports the faster transmission theory of #Omicron. pic.twitter.com/BBdAsEGUk0
In the short term, New Zealand is well placed to deal with omicron. Our strong border controls, testing and rapid genome sequencing mean that when omicron arrives at our border, we can respond quickly and prevent community incursion.
It is unlikely it will be our unwanted guest this Christmas. Despite this, significant challenges lie ahead in the long term, including vaccination inequity and disruptions to routine healthcare.
Percentage of the double vaccinated
In several regions, including Auckland and Canterbury, 90 percent of the eligible population are now fully vaccinated. High vaccination rates may blunt the extent of future potential waves of infection, but significant inequities in vaccination levels remain.
So far, New Zealand has been luckier than other countries where concerns are growing about disruptions to routine healthcare. Delays may leave patients with treatable conditions suffering illnesses that can become fatal.
Although unlikely, should Omicron breach our border like Delta did, it will have to be tackled against the backdrop of trying to manage the current Delta outbreak.
Child vaccinations are set to start at the end of January. However, low vaccination levels are often in areas where health provision and hospitals are a long way away. This will need to be incorporated into the rollout strategy to ensure equitable childhood vaccination rates.
Looking forward to Christmas and beyond
The Auckland border will lift next week on December 15 and many are bracing themselves for a covid summer. Calls for staycations have emerged as popular summer holiday spots such as Matai Bay close and iwi are asking people to stay away from some destinations.
Our analysis by regional tourism areas supports this. It shows most regional tourism areas have low vaccination rates, especially for Māori and Pacific peoples.
As New Zealand heads into the holiday season, public health measures such as mask wearing, physical distancing, hand hygiene, contact tracing, case isolation and vaccination will remain essential.
Mandating the covid tracer app increased the number of scans while less than 1 percent of paid staff at St John’s ambulance service left due to the vaccine mandate.
Some experts have suggested the emergence of omicron could be a result of low levels of vaccine coverage in developing nations.
The root of this is that the world isn not doing enough to stop the spread of covid-19.
While some countries, including New Zealand, have had domestic success at controlling covid-19, wealthy countries around the world continue to hoard vaccines. This ultimately gives the virus more opportunities to replicate and mutate.
Omicron should act as a wake-up call to ensure worldwide equitable vaccine delivery before even more concerning variants emerge.
A new study out of York University in Toronto, Canada finds that the US military plays a large role in the spread of diseases globally, including past and present pandemics. Clearing the FOG speaks with one of the lead authors, K J Noh, an expert analyst on the geopolitics of the Asian-Pacific region and health, about the study. Important factors in the spread of disease are Status Agreements that the US military makes with local and national governments that exempt members of the military from being required to follow public health measures and a culture of impunity within the military that leads to members defying all public health restrictions, even those measures imposed by the military. Noh also explains how the weaponization of disease is causing harm to everyone and why the US establishment doesn’t want the public to know there are governments designed to serve their populations.
Health authorities in Fiji have confirmed two people who had arrived in the country from southern Africa last month have now tested positive to the omicron variant of covid-19.
The pair travelled to Fiji from Nigeria on November 25.
They both tested positive to covid-19 while in a border quarantine facility.
Health Secretary Dr James Fong said last night their samples were sent to a reference laboratory in Australia for urgent genomic sequencing.
Dr Fong said both travellers’ results were confirmed positive for the omicron variant.
“The two travellers are Fijian citizens who had travelled back into Fiji from Nigeria, arriving on Fiji Airways flight FJ1392 from Hong Kong on November 25 — the day the discovery of the omicron variant was announced internationally,” Dr Fong said.
“Both travellers tested negative for covid-19 before departure from Fiji and before they left Nigeria.
Fully vaccinated
“They entered a government-designated border quarantine facility immediately upon arrival into Fiji, tested positive while in quarantine, currently have no symptoms, and were fully vaccinated.”
With the exception of four passengers, Dr Fong said other passengers on the flight were from non-travel partner countries.
“They had entered a border quarantine facility upon arrival to undergo the full quarantine protocol of 10 days,” Dr Fong said.
“That has since been extended to 14 days.
“The four passengers on the flight who were from a travel partner country have tested negative.
“The Fiji Airways crew and accompanying passengers from FJ1392 have tested negative at least twice,” Dr Fong said.
No directives to crew
Fiji Airways confirmed none of its crew or staff have been given government directives to isolate.
The airline said it had strict protocols which forced all staff to undergo swabs before and after international flights.
“None of our crew are in quarantine or have tested positive to covid-19. We understand two cases of interest have tested positive but there is no confirmation on which variant it is,” Fiji Airways said in a statement.
“However, given this new threat our staff will undergo PCR testing as a precautionary measure.”
This article is republished under a community partnership agreement with RNZ.










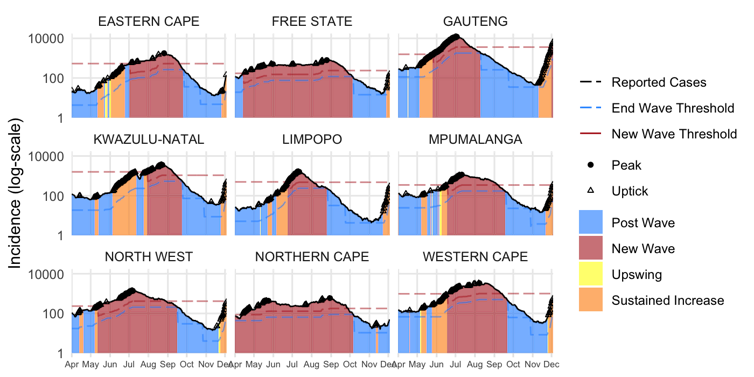
 , according to
, according to