New Zealand’s Parliament was on high security today as thousands marched through the capital Wellington for an anti-lockdown and anti-vaccination protest.
Thousands of people gathered at Civic Square for an anti-lockdown and anti vaccination protest this morning.
The group intended to march to Parliament for what they are describing as a “freedom protest”.
Significant disruptions to the bus services in the capital were expected as buses detoured away from the central business distruct (CBD) to avoid the protest.
About 50 protesters arrived from the northern side of the boundary on State Highway 1 at Te Hana.
Traffic in both directions was brought to a halt by the group and some of their vehicles.
Police said they attempted to engage with the group and a number of vehicles were towed in order to clear the roadway.
Officers physically intervened to move protesters off the road and in the process one was bitten by an “as yet unidentified protester”, police said.
“Actions like this are totally avoidable and poses unnecessary risk to our staff who are simply trying do their part in preventing the spread of covid-19,” Waitematā District Commander Superintendent Naila Hassan said in a statement.
Protesters have dispersed and police will keep monitoring the site.
Protest ‘interferes with vaccination efforts’
Te Rūnanga ō Ngāti Whātua uri and chief operating officer Antony Thompson said trucks carrying food and medical supplies were being held up unnecessarily, “creating major risks to our communities and whānau of the North”.
He said thoughtless moves like this put whānau in danger and urged members of these groups to think about the impact they were having on those they believed they were trying to protect.
Thompson said protesters were using this as an opportunity to “grandstand their issue”.
This article is republished under a community partnership agreement with RNZ.
Prime Minister Jacinda Ardern announced today that the New Zealand cabinet agreed to loosen restrictions for Auckland and upper Northland this week, while 190 new cases were reported and the deaths of two people who had covid-19 are under investigation.
Ardern said at the 4pm post-cabinet press conference that last week’s in principle decision to move Auckland to alert level 3, step 2, had been confirmed by cabinet.
Auckland will move to the new step from 11.59pm tomorrow, which means retail businesses and public facilities like libraries, museums and zoos can reopen.
Outdoor gathering limits increase to 25 people and the two-household restriction is removed.
“While we’re getting those rates higher still, we are easing into our reopening,” she said.
Ardern said that it’s hoped Auckland will reach 90 percent double-vaccination rates by the end of November, when the city will then change to the new traffic light framework.
81 covid people now in hospital
There is now an increase to 81 people in hospital with covid-19.
Two deaths were reported today of people who were positive for covid-19, but their causes of death will be determined by the coroner.
One person in their late 60s died in Auckland City Hospital on Saturday. The patient was admitted to hospital on October 23 for a trauma incident and tested positive for covid-19 on admission, the Ministry of Health said.
Another death was reported in a managed isolation facility this morning. In a statement the ministry said the returnee arrived on November 3 and tested positive during a routine day three test.
The cause of that person’s death will be determined by the coroner, including whether it may have been covid-19 related.
All three of Auckland’s district health boards (DHBs) had hit the 90 percent milestone for first doses of vaccinations late yesterday.
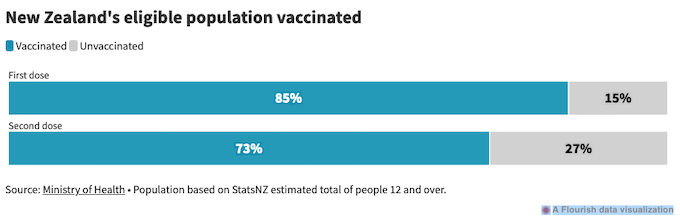
89% of NZers had first dose
To date, 89 percent of New Zealanders have had their first dose and 78 percent are fully vaccinated.
There were 14,280 vaccine doses administered yesterday, including 3272 first doses and 11,008 second doses.
Medsafe has also approved a booster dose of Pfizer vaccines for people aged over 18, at least six months after the second dose. The next step is for the technical advisory group to inform ministers about this, Ardern said.
She said there was a “strong expectation” that Auckland would move to the new “traffic light” system after a November 29 cabinet meeting.
“Moving to the new framework at that time will mean certainty for Auckland. It will mean all businesses can be open and operate, it will mean we will manage covid safely, but differently,” she said.
Deputy Prime Minister Grant Robertson told RNZ Checkpoint the push will now be on to meet that second dose target.
“We know that people now understand the importance of getting the second dose, we’re going to be working doubly hard to make sure that everybody over the next three weeks … comes forward.”
This article is republished under a community partnership agreement with RNZ.
Only 1.7 percent of Papua New Guineans have been fully vaccinated against covid-19. This has been a cause of concern for the international community, who are watching the virus spread through an exposed population with high rates of co-morbidities and minimal access to healthcare.
The mood within the country, however, is very different. No doubt there is abundant fear, but this has centred on the vaccine itself.
Many Papua New Guineans have access to the vaccine, even in some of the remotest corners of the country. They are also fully familiar with injected medicines and vaccinations against diseases like polio and measles.
But millions of Papua New Guineans are not getting vaccinated against covid because they are terrified of this specific vaccine. This is not “vaccine hesitancy”, but full-blown opposition, a genuine antipathy.
So, why is there such a fierce resistance to the covid vaccine? The key difference, as any good anthropologist will tell you, is cultural context.
Spiritual sickness Any attempt to understand local views on the covid vaccine must first appreciate that, within Melanesian societies, physicality is intimately connected to morality and spirituality. Because of this, biomedical explanations for disease are usually secondary to other causes or irrelevant.
My uncle died in my arms today. Please get your family vaccinated against COVID. Don’t listen to the anti vexers, everytime you do you are putting your loved ones and family at risk. #png#COVID#COVID19https://t.co/iFxqAa0u4c
This is mainly due to the small, sometimes non-existent role played by government education in the lives of most Papua New Guineans, especially the roughly 80 percent that live in rural villages.
For example, should an otherwise healthy person suddenly become ill and die, sorcery or witchcraft may be deemed the cause. Accusations are linked to interpersonal conflicts and jealousies that may have precipitated the mystical assault.
Such interpretations usually occur with individual misfortunes — not much larger events like a global pandemic. This is where Christianity becomes hugely important, making sense of broader problems like this.
The role of Christianity Nearly all Papua New Guineans (99.2%) are Christian. And the religious landscape in the country is powerfully influenced by Pentecostal and evangelical churches.
In PNG, Christianity provides not only the promise of eternal salvation, but biblically inscribed frameworks and prophetic ideas that inform how people live and view the world around them.
Many Christians, especially those believing in the Pentecostal and evangelical traditions, have a strong interest in the end of the world, as this signals the return of Jesus Christ.
Crucially, the imminent return of Christ is heralded by the world’s rapid moral decline and humanity being branded with the mark of the beast — a process mandated by Satan. As such, many Papua New Guinea Christians continuously and fearfully scan the horizon for this definitive sign.
Years ago, some Papua New Guinean friends declared barcodes were the mark. More recently, they insisted it was the government’s national ID card initiative.
Now, in a completely different order of magnitude and intensity, it is the covid vaccine.
As one group protesting a vaccine drive recently chanted, “Karim 666 chip goh!”, or “Get out of here with Satan’s microchip”.
From this perspective, the vaccine is a vehicle for much larger forces of global and cosmic tyranny. The speed with which the vaccine was developed, its global reach, and the apparent coercion of vaccine mandates all further strengthen suspicions of its evil origins.
However, Christianity is not the sole factor spurring anti-vaccination sentiment. Indeed, powerful misinformation on social media has also been influential, such as rumours the vaccine carries a microchip or commonly causes death. People also have a well-founded distrust of outsiders, and they view both the virus and vaccine as foreign assaults on PNG’s sovereignty.
In the absence of Western biomedical knowledge or a lack of faith in its validity, these theories flourish. Those with more sustained exposure to Western culture often try in vain to convince their compatriots against this kind of thinking.
A member of the public voicing concerns about covid vaccines during the launch of the Johnson & Johnson vaccine in Madang. Image: PNG National Department of Health/Facebook
Alternative treatments
While defiantly resisting vaccination, many Papua New Guineans nonetheless acknowledge covid-19 is real and that it causes sickness.
With infection rates, hospital admissions, and deaths now surging, it would be hard to ignore this reality. The rising covid-19 mortality across the country has scared some into receiving the vaccine, but even those open to vaccination are easily spooked by rumours of subsequent death.
In the absence of vaccinations, Papua New Guineans have turned to three main methods of treatment: prayer and healing, organic remedies, and reliance on a claimed strong natural immunity to disease.
As Christians strongly influenced by the evangelical and Pentecostal traditions, many people pray to God, Jesus, and the Holy Spirit to not just mitigate, but annihilate, the evil sickness.
In addition, many are turning to organic traditional remedies to ward off illness. This mainly consists of spices and leaves used in drinks and steaming.
Finally, there is a strongly held belief that Papua New Guineans possess an intrinsically strong immune system, buttressed by a diet of garden food, which makes them more resistant to the incursion of the covid virus.
What can the authorities do? For most Westerners, vaccines are an obvious and intrinsic good. For many Papua New Guineans, vaccines are a dangerous, unknown, and sinister threat. This is due to a combination of forces – governmental neglect, strong religiosity, and a justified distrust of outsiders.
This local position needs to be very sensitively understood and respected, not dismissed or criticised.
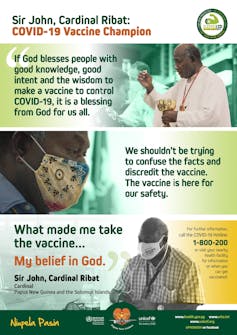
Vaccine campaign message featuring Cardinal John Ribat of Papua New Guinea. Image: PNG National Department of Health/Facebook
At the same time, deaths must be prevented and the thick fog of opposition surrounding the vaccine must be dissipated. But how?
Detailed information about the vaccine, including its creation, contents, efficacy, and potential side effects, must be made fully known to people before asking them to be vaccinated. Insisting a population with minimal information be vaccinated is not ethical or fair.
Likely in response to the widespread apocalyptic interpretations of the vaccine, the PNG Council of Churches is now actively promoting its safety and benefits. The government also needs to step up its efforts and commit to a nationwide educational campaign if hopes for substantial vaccine uptake are ever to be realised.
The success of the whole endeavour — and steering Papua New Guinea away from a public health catastrophe — will likely turn on persuading ordinary people the vaccine is a divine blessing and not a Satanic curse.
An Auckland councillor says he is astounded by the lack of cultural awareness shown by the authorities towards Māori and Pacific communities this far into the pandemic.
Manukau ward councillor Fa’anana Efeso Collins said covid-19 has become a Māori and Pacific outbreak, and South Auckland in particular is bearing the brunt.
He said calls over the past year for Māori and Pacific representatives to be at the decision-making table had been largely ignored.
Collins said those designing the response seem to have little knowledge of the communities, and it was showing.
Fa’anana Efeso Collins … “decisions are so far detached and disconnected from the realities on the ground.” Image: RNZ
“[We should have] people who are on the ground who understand our communities — right from the very beginning our request was that they be around the table that makes the decisions.
“And so these decisions are so far detached and disconnected from the realities on the ground.”
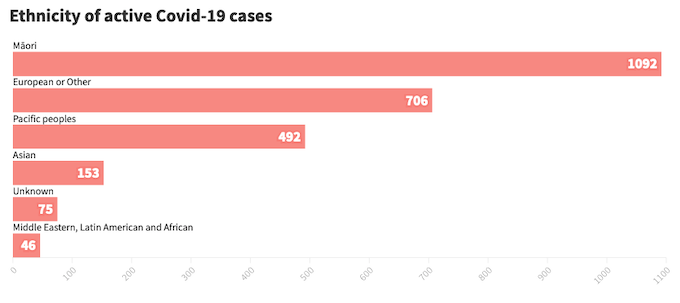
A breakdown of covid ethnicity statistics in NZ. Source: Ministry of Health
Fa’anana said the fact the government’s process for dealing with people in self-isolation was not practical was a glaring example.
On Friday a man in his fifties died in a Mount Eden apartment block after discharging himself from hospital on Wednesday.
And a 40-year-old man died while self-isolating in Manukau on Wednesday.
The cause of death has not been determined in either case, but the Health Ministry said the deaths were being considered as part of a wider systemic review it was carrying out with Auckland district health boards (DHBs).
“You know, the Ministry of Health says everyone gets sent an email. I think it’s time to get real — none of us read emails.
“And so I think that’s the level of lack of intelligence that perhaps we’re seeing from the Ministry of Health because they’re not on the ground, they don’t understand our communities.”
Battling the Health Ministry
“Fa’anana said health reforms cannot come soon enough.
Fa’anana’s criticisms come as Whānau Ora is battling the Health Ministry in court to try get access to personal data on unvaccinated Māori released to them.
The organisation wants to use the data for directing campaigns to increase vaccination rates among Māori.
The ministry has agreed to provide some of the data sought. It agreed to supply individual’s vaccination status for previous clients of Whānau Ora services, and anonymous vaccination status data to street level, to show unvaccinated areas in communities.
While the ministry has so far refused to hand over the full personalised data, after a High Court ruling this week it agreed to work with Whānau Ora to identify places where “outreach to Māori is most needed”, and to identify what data sharing was needed in those cases.
South Auckland health workers going door-to-door Manurewa-Papakura ward councillor Daniel Newman said the ministry’s vaccination campaign had fallen short and left too many people vulnerable to the virus.
He said the government’s failure to set vaccine targets for Māori was already having consequences, and that is showing in hospitalisation statistics.
In his ward, frontline healthcare workers have resorted to door-to-door visits in an effort to reach vulnerable and vaccine-hesitant residents.
However, that could potentially expose them to people who are infectious with the virus and are isolating at home, he said.
He called on the government to protect healthworkers by letting them know where people are isolating at home with covid-19.
“It’s really important that we stay safe, because not only do we need to protect our own health, but we can’t become conduits for covid-19 ourself.
“The important thing for us is that we have enough scale that we have the ability to get to enough people as soon as possible.”
He said the door-to-door approach was necessary: “We’re in a race against covid-19 which is seeding in those streets, we need to get people protected before they become unwell.”
This article is republished under a community partnership agreement with RNZ.
Church minister Suiva’aia Te’o says proactive communication, compassion and clear information have led to a fully vaccinated congregation.
Like most churches operating under level three and four rules, the Sāmoan Methodist Māngere Central church livestreams services on Facebook and holds Bible studies and prayer meetings over Zoom.
To keep the young people engaged they run Kahoot! quizzes and online talent shows.
But when lockdown rules lift, the congregation will be able to confidently worship in person — because all 120 of them are already double-vaccinated.
The church’s Reverend Suiva’aia Te’o says no edict or mandate was imposed by her or anyone else. Rather, she made sure everyone was given clear and relevant information, and then members of the congregation got the vaccinations of their own volition.
“One Sunday I gave a brief talk about why they should take it. My thinking was if everybody understands why, then they can make a decision for themselves,” she says.
Te’o was motivated to promote the vaccine after attending a talk organised by Pacific health provider South Seas for church ministers in South Auckland. She says the crux of her message to the congregation was to do it for the “love of family”.
‘We breathe the same air’
“We all live in the same world and we breathe the same air,” she says. “The delta variant can spread so easily, and so I reminded them it was about the safety of their families, the safety of the community and the safety of the church.”
She also recruited the support of her church’s youth group leaders, including Māngere College student Gardinea Lemoa.
“We have youth meetings every Friday and so I’ve just been encouraging them to get vaccinated and to get their friends and family vaccinated as well,” says Lemoa.
“We’ve also been making up memes so they could post things on their social media accounts.”
Te’o is well aware that some Christian leaders are calling the covid-19 vaccine the “mark of the beast” and a sign of the end times, but she’s got no time for such attempts to stoke fear.
“I know they say that’s what they believe, but I don’t agree. I think it’s just an excuse and they need to get vaccinated.
“We have got this remedy, and I’m convinced it has been developed with God-given wisdom and knowledge by professionals so we can be safe.”
86% of eligible Pacific population
Before this weekend 86 percent of the eligible Pacific population have had their first dose, compared to 89 percent of Europeans and close to 100 percent of the Asian population.
Around 50,000 Counties Manukau District Health Board residents still need to get their second dose in order to reach the 90 percent double-vaccinated threshold. It’s a marker the Auckland and Waitematā DHB populations need about 15,000 and 40,000 doses respectively to reach.
“It is encouraging to see so many community-led initiatives happening now. But these should have been resourced from the beginning,” he says.
“Instead, the first big mass vaccination event was held at [higher learning institution] Manukau Institute of Technology (MIT). It was great that they got 16,000 people vaccinated then, but it actually made things worse in some ways, because they barely vaccinated any Māori or Pacific people.”
He says when local organisations like churches are empowered to take the lead, mistrust and misinformation become less of a hurdle to overcome.
“Now we have Pacific providers taking ownership we are finally seeing a lot more acceptance and uptake of the vaccine.”
Quickly got on board
Te’o says though her congregation quickly got on board with the vaccination rollout, many have still found lockdown challenging.
“I thought with this lockdown it would be quiet for us, but it’s not – there’s more and more Zoom meetings and more work. It’s been a hard time, the world is changing a lot for so many of us and there’s a lot of uncertainty.
“We’ve been providing food parcels for some families and some have needed small monetary grants to help with paying the power or other bills.”
But one thing she is confident about, given all her congregation is vaccinated, is that when they do get back to in-person services they’ll all have that extra layer of protection.
Local Democracy Reporting is a public interest news service supported by RNZ, the News Publishers’ Association and NZ On Air. Asia Pacific Report is a partner.
A record 206 new community cases of covid-19 were reported in New Zealand today, as the total number of vaccinations in this country topped 7 million.
There was no media conference today. In a statement, the Ministry of Health said there were 200 cases in Auckland, four in Waikato and two in Northland.
The ministry said 159 were yet to be linked to earlier cases, with 623 unlinked cases in the past 14 days.
The two new cases in Northland — which are both close contacts of earlier cases — bring the total number of cases in the region to 17. Two of the four new cases in Waikato have been linked to earlier cases.
The ministry said the 206 community cases numbers reported today were “a reminder of the infectiousness of covid-19, and particularly the delta variant, and the importance of vaccination as the number one protection against the virus”.
There are now 73 people in hospital with the coronavirus, including seven in intensive care. The average age of the people in hospital is 51.
There was also one new case reported at the border today.
Papua New Guinea — a country faced with a depressed economy and its public health system on the brink of total collapse due to the covid-19 pandemic sent a 62-member delegation to Europe to attend the COP26 Climate Change conference at a cost of a whooping K5.8 million (NZ$2.03 million).
The Post-Courier was told the initial budget for PNG’s participation in the climate change conference was put at K20 million for 82 people.
However, this was brought down to K5.8 million, but the National Executive Council approved only K3 million and reduced the number of delegates to 62 people.
Prime Minister James Marape stayed in PNG and appointed his Minister for Environment and Conservation, Wera Mori, to head the delegation to Glasgow.
Mori, when contacted by this newspaper to justify the cost, referred us to the NEC.
Apart from Mori, other MPs on the trip are Oro Governor Gary Juffa, Member for Moresby North West Lohia Boe Samuel, Member for Talasea Francis Maneke, Vice-Minister for Works and Member for Anglimp-South Waghi Joe Kuli, Member for Kairiku-Hiri Peter Isoaimo and Member for Rai Coast Peter Sapia.
The money was spent on airfares, accomondation and allowances and the delegation requested from the Finance Department in total K800,000 for airfares and K620,000 for accommodation for 10 nights.
Furthermore, travel allowances for the special envoy, the six other MPs with their officers was at US$500 to US$600 per day and at today’s exchange rate, this works out to about K2500 to K3000 a day.
Travel allowance rates
For the public servants, the current rate for travel allowance is at US$300 (K1500) per day and accommodation between US$200 – US$250 (K600 – K1250) per day, depending on the rate charged by the hotels they are booked in to stay.
According to our findings, the actual cost of the trip would have been K1.32 million.
The delegates travelled in three groups and the round trip — Port Moresby, Singapore, Doha and Glasgow — and back cost K19,000 on business class for the envoy and the MPs and K12,980 for the others on economy class.
The Post-Courier was told the first 20 travelled on PX 009 on October 23, the next 20 on the 24th and the rest on the 25th.
Attempts to get the full list of the delegation as well as an official response on the exorbitant cost from the Prime Minister’s office and the departments of Finance, and Foreign Affairs and Office of Environment and Climate Change were unsuccessful.
PNG’s Kundu London High Commissioner was also sent questions relating to PNG’s participation and the costs, but this newspaper was advised all media responses must be channelled through the Foreign Affairs Secretary Elias Wohengu.
This is the second international conference on Climate Change PNG has participated in as a country.
‘Corruption at its best’
After the COP15 conference held in Paris, France, in 2015, the then Environment Minister, Sir John Pundari, went public and condemned the conduct of some members of the government delegation to that conference.
In his criticism, Sir John particularly talked about the attendance of members of the delegation, noting that some went missing, others turned up late while others left early for home.
At that time, Sir John said he was very disappointed that even his fellow ministers who were part of the government delegation quickly disappeared.
He said then that “getting airline tickets and allowances to attend international meetings, and to show up for a day or two, then spend the rest of the time in other places was corruption at its best, and must never be encouraged”.
Over the last two weeks, the Post-Courier asked Sir John twice to comment on the COP26 trip but he referred the newspaper to the Prime Minister’s office instead.
By PNG Post-Courier reporters. Republished with permission.
Tonga’s only suspected covid-19 case has tested positive when he took his third test today in Nuku’alofa.
The latest result came after the person was tested positive last week and tested negative on Monday this week.
The Health Ministry chief executive Dr Siale ‘Akau’ola said today the person had recorded a very weak positive result which likely reflected a historical infection.
He described the second positive result as “weaker than the first weak positive result”.
Dr ‘Akau’ola said the result showed what appeared to be a fragment of dead virus from old infections.
He said the ministry discussed the result with a team from the World Health Organisation (WHO) this morning.
He said there was a lot of “technicalities in the case”.
‘Not infectious’
“We believe the person is not infectious,” he said.
Dr ‘Akau’ola said the result meant there was no need to panic.
“It is not a new virus and the ministry is highly confident about it.
“The virus is shedding.”
He said the machines Tonga was using for the tests “are very sensitive”.
“Whenever they detected a fragment of a virus they will show it as positive”.
Dr ‘Akau’ola was speaking during a press conference this afternoon attended by the Prime Minister and a team of government officials.
The patient has been transferred to a special quarantine facility in Mu’a after he arrived at the kingdom from Christchurch last Wednesday on a flight carrying 215 people.
They had four contacts in New Zealand — all of whom returned negative tests.
A second person with covid-19 who was isolating at home has died in New Zealand, the Ministry of Health has confirmed.
In this afternoon’s covid media briefing, where it was revealed there were 163 new community cases of covid-19 today, Director of Public Health Dr Caroline McElnay said St John Ambulance attended a call this morning after an emergency call to an address in the suburb of Mount Eden and found a person dead on arrival.
The man in his fifties is understood to have been recently treated in hospital.
“Health authorities in Auckland are working with the police and ambulance crew to review the circumstances around the death,” Dr McElnay said.
Deputy Prime Minister Grant Robertson said it was his understanding the dead man was admitted to hospital on Monday and discharged himself from the hospital on Wednesday.
He said there had been phone contact with them on Wednesday and Thursday.
“I am confident in the system. Obviously when we introduce a new system like self-isolation we need to continully monitor it and that’s happening,” he said.
Looking at wider system
“Between the Ministry of Health and the Auckland regional public health, they’re looking at both these specific incidents, but also at the wider system.
“It’s important to note there are still enquiries going on about the cause of death at the moment and we’ve just got to all make sure we allow that to occur.”
Robertson said before it was decided that a person could self-isolate, there was a public health assessment of issues like the circumstances of someone’s accommodation.
A medical assessment also determined the person’s suitability as a candidate for self-isolation.
“We’re not in a position at the moment to be able to say what the cause of death was for either patient,” Roberston said.
Dr McElnay said the coroner would look at both deaths.
Meanwhile, a covid-19 case fled a Hamilton MIQ facility this morning by removing a section of fencing and jumping into a waiting car, but were stopped by police a few minutes later.
It was one of two attempts to flee a MIQ facility in the past day, with another covid-19 case running away from the entrance to the Holiday Inn at Auckland Airport last night.
They were also caught within five minutes.
In a statement, Joint Head of MIQ Brigadier Rose King said every single event like this was “extremely disappointing”.
This article is republished under a community partnership agreement with RNZ.
Health Ministry Chief Executive Dr Siale ‘Akau’ola says the ministry had not responded to allegations made on social media to protect the privacy of a suspected covid-19 patient.
He said the ministry had been very careful not to release any information that might identify the person.
He said the patient should have been advised not to release any information.
Dr ‘Akau’ola said information had been released through various channels, which had caused problems.
Prime Minister’s concerns During yesterday’s press conference a journalist asked why the patient was allowed to contact other people on his mobile phone.
He said this was why there were concerns in the social media that the government should take the situation seriously because what had been leaked from the MIQ included information that was unreliable.
He asked Prime Minister Pōhiva Tuʻiʻonetoa to make a firm decision on the claim.
In his response, Tuʻiʻonetoa said he had just received a message on his mobile phone and was disappointed with what had been revealed in it.
The Prime Minister did not go into details on what he had received, but it appeared it was a video clip which had been widely shared on Facebook purporting to show the patient talking to what appeared to be family members on a mobile phone while the conversation was being recorded on another phone.
Chief executive of Tonga’s Ministry of Health Dr Siale ‘Akau’ola … another test expected today for the patient. Image: Kaniva Tonga/Christine Rovoi/RNZ Pacific
Serious accusations
In that conversation serious accusations were made against the government, including claims that it was lying to the public when it said the patient had been taken to the Mu’a MIQ on Saturday.
The patient said he had been taken on Monday.
During the conversation the patient said he had tested negative, but the ministry kept on telling the public the test was positive.
Dr ‘Akau’ola said two tests must be carried out to confirm a negative result. The patient’s second test would be today.
Kaniva News reported yesterday that Dr ‘Akau’ola had said the patient had returned a weak positive result and had now tested negative.
The Prime Minister said: “I have listened to it (the recording of the conversation) and I did not like the attitude of their conversation and it said the patient was taken to Mu’a MIQ,” the Prime Minister said.
Tu’i’onetoa asked the meeting for his officials to clarify when the patient was taken to the MIQ.
“I want to confirm that,” he said.
Respect for the patient The Minister of Health and her CEO were looking at each other before the CEO apologised to the Prime Minister and the conference, saying it was true the patient was taken on Monday not Saturday as he was advised, because of some paper work issues.
The CEO said the ministry highly respected the patient.
“We wanted to protect his identity,” Dr ‘Akau’ola said.
“He is carrying a huge burden and the people’s concerns as well.
“As I look at it there was a weakness as he should have been given proper counselling advice for him not to release any information.
“However, we learnt from this”, the CEO said.
Family members This morning some family members of the patient were concerned that some posts on Facebook targeted the patient’s paternal side.
The posts included one which said the problem was that the family should not have released the identity of the patient to the public because it would backfire on them.
Another said the whole family could be stigmatised by the situation, something that is extremely common in Tonga.
It said some families or clans were stigmatised with “kilia”, the Tongan word for leprosy, in the past. Nowadays it was a stigma that people used to identify those families whenever there was any dissatisfaction with them.
Republished with permission.
This content originally appeared on Asia Pacific Report and was authored by Kaniva News.
Welcome to “Movement Memos,” a Truthout podcast about things you should know if you want to change the world. I’m your host, writer and organizer, Kelly Hayes. This week’s episode is a throwback situation. In place of our usual content, we are revisiting “A COVID Memorial Mixtape,” which was released in October of 2020 by Ric Wilson in collaboration with a number of grassroots organizers. The mixtape was created as part of a month-long effort to memorialize people we have lost to COVID-19, and it was played through a loudspeaker outside the Metropolitan Correctional Facility in downtown Chicago. During that month, we dropped banners, built shrines and made art, at a distance, so that we could grieve together. When we made this tape, we had lost over 200,000 people to COVID-19 in the United States. Now, we have lost over 750,000. Globally, more than 5 million people have died. So let’s take a pause, and revisit some reflection, reverence and resistance around those losses.
Note: This a rush transcript and has been lightly edited for clarity. Copy may not be in its final form.
[music begins]
Juliana Pino Alcaraz: My name is Juliana Pino Alcaraz. I’m a Colombiana Afroindígena Wayuu and Bari who is here as an abolitionist in the environmental justice movement in Chicago. My words that follow are in response to how state violence is driving deaths and lying to us about what we know we’re facing from COVID, a respiratory illness whose transmission is made severely worse by air pollution, incarceration, and anti-Black racism, meaning hundreds of thousands of community members have already been lost. Community members, we are here to collectively remember.
You/We bled in water: they don’t even try to pretend you are/were alive.
They will tell you a simple story, full of tall tales about your worthlessness, and they will call it the medicine you actually deserve. They will supply you expired food, and say you earned an expiration date. They will poison your person with exposure to the slow violence of pollution and pandemic, and ask you why you can’t breathe? They will fill their reports with myths of Black danger, justified Native genocide, and friendly evictions. They will claim that cops keep us safe, that the companies imploding toxic clouds into the chests of abuelas really had our best interests at heart.
They will dare to call this correct.
We will reach deeply into the empathetic earth, to the place where Black lives matter and Indigenous spirits thrive and Brown people rejoice, where we all receive our fire from this planet and the seed of our food is nourished, and we will tell the truth. We will rage aloud that air quality indoors is five times worse outside than inside the cages in which they trap you, our families, and that this is the air you are breathing. We will tell them that Personal Protective Equipment requires being treated like a person in the first place, with a filter dignifying your face to shield you and your people from the toxic, viral disregard disintegrating your lungs. We will follow the lead of youth to defend their futures and protect the water from all of their deadly pipelines. We will battle back the abusive attempts to disappear your humanity inside of assaults, numbers, murders, and statistics. We will labor to heal with and protect each other in spite of all of this, and,
We will dare to tear these systems apart.
Perceive me now: the walls of this place WILL crumble and the land returned by the foundation-shaking, system-ending strength of our bonds to each other.
Angela Davis once said, “we have learned to forget about prisons.” We pledge to you that we do not believe their simple stories, and we will not forget. Because try as they might, these bars cannot keep us from destroying their assets and building our reality back up together. We are energized by your sounds of solidarity for Black lives, we love you, and we love all souls we have lost. We will correct the record: YOU are worthy, YOU are our community. WE are worthy, WE are our community, and WE all grieve together.
Together, we transform water dripping with poisonous particles.
Together, we clear the air thick with pollution, COVID, and lies.
Together, we honor the soil ground down with waste of industry and the bones of ancestors.
Together, we remember the souls snatched away from our family, always too soon.
Together, we turn chains to dust, returning the minerals in steel and concrete to the plants.
Together, we rest in community without being disposed of in our own beds.
Together, we rise to deprive the monster of its simple story, and replace it with our own.
Benji Hart: My name is Benji Hart. I’m an author, artist and educator currently living in Chicago, and I would like to offer up, by way of mourning, and by way of grieving, love to the people who we’ve lost to COVID, particularly folks in the mass incarceration system, including detention centers. And I also want to offer up grief for all the lessons that COVID has attempted to teach us: lessons we haven’t heeded, but that we’ve also been discouraged from heeding by the current administration and ruling class. COVID sent us such strong messages about how connected we all are. COVID has taught us so much about the meaningless categories that we divide our society up by — folks on the inside, folks on the outside, folks with healthcare, folks without healthcare, folks with citizenship, folks without citizenship — and in actuality, when there’s a pandemic, you can’t make those distinctions. If a pandemic is allowed to happen in one population, it impacts all of us. If certain parts of the population don’t have healthcare, we actually can’t control a disease like COVID-19.
And instead of slowing down, instead of backing off of the ways that we were harming the environment, instead of really devoting ourselves, and committing ourselves to making universal healthcare a reality, to getting people out of cages, to opening borders so that people can actually move freely as they need to, and share resources with each other as they need to, we did the exact opposite. And so many of the people we’ve lost, it’s because we haven’t heeded the lessons, the teachings, that COVID really has tried so hard to impart on us. So I grieve for both of those things. I grieve for the opportunities for learning, for transformation of our society and ourselves that we so briefly, and so closely, almost attained, and were so quickly discouraged from doing so by folks in power: by the federal government, and by folks with money and resources who were willing to sacrifice young people, Black people, Indigenous people, undocumented people, and incarcerated people so that folks with money didn’t lose a profit, and so that the economy continued to generate the inequities and environmental catastrophe it has always been generating.
I mourn for the ways we haven’t learned this year: that we should have learned, that I wish we collectively did. And I offer up a prayer to those we’ve lost, to their grieving families, and also to a future where we do learn the lessons, where we fight for each other collectively and don’t sacrifice our neighbors, don’t sacrifice the most marginalized among us to a pandemic, whether that pandemic is COVID or whether that pandemic is capitalism, whether that pandemic is the police prison and military system, or whether that pandemic is white supremacy and white nationalism. I dream of a day, and pray for a day, where we learn to see each other as part of one collective and fight for collective liberation.
Bresha Meadows: I am Bresha Meadows, a member of Lifted Voices. I was once incarcerated for an act of self defense. Today, we honor those we have lost to COVID-19, including many counted and uncounted deaths that have occurred behind prison walls. Having been in jail, I know the everyday worry, and adding a virus, one that has taken many lives, can make it almost impossible to want to keep going. Although jail is supposed to be a place for punishment, to hold someone where they are getting more and more sick is almost the same as the death penalty itself. A good friend of mine has a dad in jail, and he has also been diagnosed with COVID, but they have little to nothing to help him. Seeing how this affected her and her family has brought me to the realization that prisons are treating this virus as nothing more than a common cold.
I’m lucky enough to have gotten out, and I try to do everything most people wouldn’t expect me to do. I go to classes at Cleveland State University, I’ve got my own apartment. I have become a part of Lifted Voices, and I found that I also want to help others get free. We can’t leave people behind who were already being left behind. We can’t do what we’ve always done. We can’t allow what happens to people to mean less to us over time. Whether people live or die, it has to matter more and more to us, not less. We cannot help people if we forget them. We cannot help ourselves if we give up on people. We are not giving up on people in jails and prisons or detention centers. We are not giving up our hope.
Tanuja Jagernauth: My name is Tanuja Devi Jagernauth, and I am honored to contribute to this mixtape on behalf of the Mutual Aid Mourning and Healing Project. We are a diverse group of folks who came together in March of 2020, connected by a shared understanding that, one: collectively devastating times call for collective methods of healing and, two: no one should have to grieve alone. We are also connected by a drive to politicize what is often shrugged off as “private” or “personal.”
Every single death due to COVID-19 is as political as it is personal. Every single death implicates Donald Trump, a fascist who continues to spread lies and misinformation about the severity and impact of the pandemic.
However, wherever this finds you, please know: your life matters to us
and if this moment finds you holding the pain of loss
I want to humbly offer a moment
to hold it with you.
For the loss that is fresh, hot — an open wound,
For the loss that is so old you can’t remember which lifetime — or whose — it came from,
For the loss you cannot name yet,
For the loss of a friend,
For the loss of a lover,
For the loss of family,
For the loss of home,
We mourn and rage with you.
And inside our grief, wherever it might live in our bodies,
However it feels today,
May we find that thing — anything — that can move.
May we find that thing we can touch, pick up,
and roll around in our hands
like a perfect ball of clay,
heavy and cool to the touch.
May we find its potential
and use it to build the next world together.
Cindy Milstein writes in Rebellious Mourning, “Our grief can open up cracks in the wall of the system. It can pry open spaces of contestation and reconstruction, intervulnerability and strength, empathy, and solidarity.”
Through our mutual aid work, we are learning to let go of our privatized selves. We are learning to connect our personal needs for survival, safety, healing, and community to people around us who we once considered strangers.
We are learning how to ask for help, and we are learning how to receive it.
We are learning the critical difference between harm and accountability.
We are learning that we have all we need, and we are finally admitting that we are all we’ve got.
Slowly but surely, with care and intention, we are co-creating the next world.
Until it comes we will continue to love each other out loud.
We will continue to rage and weep together.
We will continue our riot of empathy.
Our bonds make us powerful,
and that scares the shit out of Trump
because at the end of the day, he knows
there are more of us than them.
There are more of us than them.
There are more of us than them.
Aislinn Pulley: I am Aislinn Pulley. I am the co-executive director of the Chicago Torture Justice Center, co-founder of BLMChi, and a board member of Ujimaa Medics. I am a long-time organizer, an artist, born and raised in Chicago.
I have known so many people who have been affected by COVID. I have known people who themselves have lived through, suffered through the virus. People who have succumbed to death. The disproportionate number of people of color and specifically Black, indigenous and Latinx people who have died from this virus is unconscionable. In the United States, Black, Indigenous, Pacific Islander, and Latinx people all have COVID-19 death rates that are roughly triple or more than White people. In a country that has historic wealth, amassed at the detriment of services needed in our communities, the example of how COVID is disproportionately affecting the poor is unconscionable.
This is a country that has amassed the richest resources in the world and yet uses them to incarcerate, torture, and kill its populace. We must dismantle this system. We must create a system that is built on sustaining life and ensuring our livelihoods.
COVID has proven how necessary this is, and that the time is now. We can no longer wait. We have to dismantle, we have to upend, we have to create new. It has never been clearer that it is this system that is causing unnecessary deaths. It is incumbent upon us to act.
Kelly Hayes: My name is Kelly Hayes. I am a Native writer and a prison abolitionist organizing in Chicago, Illinois. Over 950,000 people have died of COVID-19 worldwide. More than 200,000 deaths have been attributed to COVID-19 in the United States, but we know the real number is much higher. We know that even before COVID-19, imprisoned people were experiencing conditions that were stripping away years of their lives, robbing them of both the present and the future. For many people living in cages and outside of them, survival was already a daily struggle. And now, as winter approaches, we know that greater atrocities are close at hand. We know that COVID-19 is already tearing its way through jails, prisons and detention centers, striking people who already had no functional access to healthcare. The results have been devastating, now with flu season upon us, people will suffer and die in even greater numbers, unless we get them out.
Freeing imprisoned people may seem too radical an aspiration for some right now. The election has given people a whiff of hope that the system might yet save them, and while it is possible to reduce the damage done, we are staring down mass death, nationwide evictions, financial collapse, and even the potential collapse of our profit-based healthcare system. In a time of crisis, capitalism will always cut its losses, as needed, to survive. It has done so by way of the prison industrial complex for a very long time. People who do not fit neatly into society, psychologically, economically, or otherwise are disposed of. Some die, and some are simply stuffed into containers. Disabled people and the elderly are similarly discarded and contained in the U.S., which is why we have seen so many retirement homes and assisted living facilities ravaged by this disease. No plan was made to safeguard these people. They were never an economic or social priority, so they were disposed of.
In the coming years, the system will have to dispose of more and more of us to sustain itself. This is a time of collapse, and also of possibility. We cannot afford to be meek or passive, or to allow history to simply happen to us. Rather than shrinking away from our imprisoned siblings out of some misguided fear of rocking the boat, we should be rejecting the continued expansion of a carceral state that threatens to swallow so many of us in the years to come.
This society wants us to believe that our fates are our own — that by abandoning one another, we can keep ourselves safe individually. But what will happen to us, to our neighbors, and to our families, as jobs continue to evaporate, and mass eviction and displacement play out across the country? Where will we be contained? In poverty districts that we are not allowed to leave? Will we be surveilled, criminalized, and monitored by ankle bracelets? That dystopian framework does not have to be invented. It is here, growing, and grinding people under. It is the sprawling prison industrial complex that not only keeps people locked in prisons but has also outsourced imprisonment into our own homes.
COVID-19 is a genocidal weapon in the hands of this government, but it will also knock on many doors at random in the months to come. If we organize, our collective pain can become collective empathy and action. But this will not happen on its own, as a result of social deterioration. It will take political will, compassion, and courage. Whatever is ahead, our survival will depend on our willingness to organize, and our freedom will depend on our willingness to fight for each other — and that means fighting for our imprisoned siblings.
There is a reason they don’t want us to grieve together. Because they know we will be more powerful if we do.
May the fallen rest in peace, and may the rest of us raise hell.
New Zealand’s Ministry of Health has reported 139 new community cases of covid-19 today, with 64 people now in hospital with the coronavirus.
In a statement, the ministry said two of the new cases were in Waikato and one was in Northland, with the remaining cases were all in Auckland.
The Northland case — which takes the total number of cases in the region to 15 – is a close contact of the two previously reported Taipa cases and has been isolating at home.
The person tested positive for covid-19 on October 24 and had been self-isolating in Manukau.
The ministry said the cause of death was unknown and the coroner would determine whether it was due to the virus or something else.
It said today it was aware of speculation that the death was vaccine related, “but we can confirm it was not”.
“The Northern Region Health Coordination Centre and the Ministry will undertake an incident review of the public health and clinical oversight of this person with independent input.”
There have now been 3871 cases in the current outbreak.
There were 26,999 vaccine doses administered yesterday, including 6659 first doses and 20,340 second doses. The ministry said 89 percent of New Zealanders had now had their first dose and 77 percent were fully vaccinated.
“Getting vaccinated will help to stop people from becoming seriously ill from Covid-19 and will save lives,” said the ministry.
This article is republished under a community partnership agreement with RNZ.
A person who tested positive for covid-19 in Tonga has now tested negative, says the Ministry of Health CEO.
Dr Siale ‘Akau’ola said another test was expected tomorrow for the patient.
He said yesterday the covid-positive person, who arrived in Tonga from Christchurch, would continue to stay in the MIQ until his 21-day quarantine was over.
Dr ‘Akau’ola, who joined the Prime Minister and a team of government officials in a press conference in Nuku’alofa, said he was advised on Monday that the person had provided a second negative test.
Dr ‘Akau’ola reiterated during the conference that the sample from the patient was tested on Thursday, October 28 and Friday, October 29. He referred to the positive result as “weak positive”.
The Tonga case came after a weak positive case tested negative on the second test in New Zealand.
Last month, a covid-positive person who travelled to Katikati from Auckland, tested negative on their second test.
“The person had a high CT value, indicating a weak positive result, and was tested again following their initial positive result last week”, Stuff reported.
Tested on three machines ‘Akau’ola said the person’s sample was tested on all three of the Health Ministry’s covid-19 testing machines on October 28.
He also repeated what he had said in the previous conference on Friday that the weak virus could be a historical virus or a “baby virus” which tried to grow, but was stopped by the antibiotic because the patient was fully vaccinated.
“The nature of the virus is shedding and it can be negative or positive at various times and this is why we have the 21-day quarantine rule.”
All the people on the flight from Christchurch were required to have negative covid tests prior to departure.
New Zealand’s Ministry of Health said the positive case was fully vaccinated with the Pfizer vaccine, and had their second dose on October 15.
Tonga’s main island Tongatapu is currently on lockdown for one week until Monday, November 8.
Kalino Latuis editor of Kaniva Tonga. Republished with permission.
Manurewa-Papakura Ward councillor Daniel Newman has called the death a tragic example of the toll that the pandemic is having on South Auckland.
The Ministry of Health said that currently the cause of death was unknown and it may have been covid-19 or some other cause.
The death will be referred to the Coroner, it said.
New Zealand has recorded 28 covid-19 deaths since the pandemic began. If covid is confirmed as the cause of this death, it would bring the total to 29.
Almost 700 self-isolating at home
Nearly 700 people are self isolating at home in Auckland, with the total number of active cases in the region now more than 1900.
There were 97 new community cases in Auckland today, and the city is now dealing with 1904 active cases.
Prime Minister Jacinda Ardern did not turn up to a planned New Zealand media event at a vaccination clinic in Whanganui today where a group of anti-vaccination protesters gathered.
Ardern was visiting a vaccination bus in the city and changed the time of the stand-up to just after 1.20pm at a new venue.
Around 200 anti-vaccination protesters made their presence felt at the mobile clinic on Victoria Avenue.
The government has purchased another 4.7 million doses of the Pfizer/BioNTech vaccine for use in New Zealand over the next year, Covid-19 Response Minister Chris Hipkins revealed while giving the latest details on the pandemic with Director-General of Health Dr Ashley Bloomfield.
Second day in row
This was the second day in a row that an Ardern covid media briefing had been disrupted by protest over covid vaccination. Yesterday, heckling in Northland by an American pharmacist claiming to be a journalist forced the prime minister to change venues in the middle of the press conference.
“We are at a stage in the vaccine roll-out where we are trying to reach into communities that may hold firm views,” Ardern said today.
“But we need to have those conversations and, just talking to some of our health practitioners, their goal is to talk to everyone wherever they can to have those conversations about why it’s so important that people are vaccinated.”
On teachers who may be about to lose their jobs due to the government vaccination mandate, Ardern said: “We have not taken lightly the decision for some areas to require vaccination. It’s taken a lot of discussion and careful thought and we have focused in on those groups that we consider high risk.”
On whether mandates have destroyed social cohesion and forced some into corners, Ardern said although it may have had that effect with some, for others it had forced a conversation and made people ask questions.
“We had the experience of having already rolled this out for our border workers and what we noticed was by putting a date it did cause those who had questions to go and seek advice, talk to trusted health professionals and then make a decision.”
On her statement at the beginning of the pandemic that vaccinations would never be forced on anyone, yet mandates seemed to contradict that, Ardern said it was always her view that the government would not force all New Zealanders to be vaccinated and that view had not changed. They would not.
‘Duty of care to the vulnerable’
“This is about certain workforces and work places, where we’ve applied assessment on whether or not we have a duty of care to look after those most vulnerable.”
“We’ve guarded against requiring vaccines where we need to ensure that people are always, no matter what, they are able to access health services, food, government support.
“We have been very clear, we will not require nor will we ever require vaccine certificates to access food, government benefits, access services that people need to live.”
Vaccination efforts across the country are in fully swing as district health boards work towards 90 percent full vaccination rates.
Only five district health boards have hit the milestone for first jabs: Capital and Coast, Auckland, Waitematā, Canterbury, and, just yesterday, Southern DHB.
Counties Manukau District Health Board is on the home stretch to meeting the 90 percent first dose milestone, only 3951 injections away.
This article is republished under a community partnership agreement with RNZ.
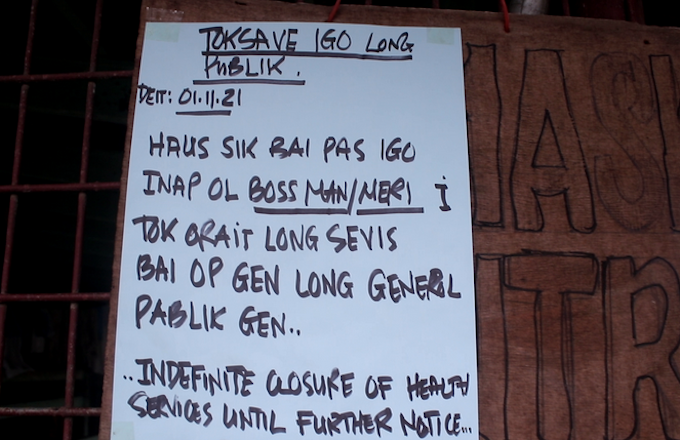
Urban clinics in Papua New Guinea’s second city Lae have closed for an indefinite period following attacks on health workers.
Anti-vaxxers have been verbally or physically attacking health workers over false claims of state mandatory vaccinations against the covid-19 pandemic.
Health workers and support staff manning facilities around the city have reported incidents of stone throwing, swearing and threats to their personal safety, with some people viewing them as “agents of a forced covid-19 vaccine”.
The National reported at the weekend on an attack on a three-member ambulance crew by people last Thursday wrongly believing St John Ambulance staff were administering vaccines.
A surge in covid misinformation and disinformation on social media is hampering health authorities in their work.
While the Morobe Provincial Health Authority is yet to advise residents about the crisis, health workers say nobody is manning the clinics as they have all been asked to stay at home until further notice.
A visit to the Malahang and Butibam clinics revealed that similar notices were posted saying: “Haus sik bai pas inap ol bosman/bosmeri i tok orait lo open gen”. (Hospital will close until approval is received from bosses.)
The next option for residents is to go to the overcrowded ANGAU Memorial Provincial Hospital or visit private clinics and pharmacies.
Barely 1 percent vaccinated Asia Pacific Report reports only 1.2 percent of the nine million Papua New Guineans are vaccinated against covid-19.
According to the John Hopkins University covid dashboard, 29,715 cases of covid and 370 deaths have been reported on Papua New Guinea but health officials fear the real toll is far higher because of limited testing and records.
Prime Minister Jacinda Ardern says the New Zealand government wants to lift vaccination rates and wants to remove anything that is a barrier to getting as many people vaccinated as quickly as possible.
Ardern and Māori-Crown Relations Minister Kelvin Davis, who is also the MP for Te Tai Tokerau, are in Northland viewing the rollout of vaccinations.
Ardern spoke to media this afternoon until she was continuously interrupted by a conspiracy theorist in the crowd. She then decided to shut down and move the conference.
Covid-19 Response Minister Chris Hipkins announced that the northern part of Northland would be tightened to level 3 from its current level 2 from 11.59pm tonight until Monday November 8 in response to two new cases that have no epidemiological or other link to cases in the region;
The Ministry of Health announced 126 new community cases today — 107 in Auckland, 18 in the Waikato, and one in Northland. Of these, 59 cases were not epidemiologically linked;
Low vax rates not government’s fault
In today’s media conference, Ardern said the low vaccination rates in Northland were not a failure of the government.
She said the government wanted to lift vaccination rates, and wanted to remove anything that was a barrier to getting as many people vaccinated as quickly as possible.
“I asked one provider, what are you hearing when you’re out vaccinating … they described it as covid not necessarily feeling close enough to the community yet, that even when there have been cases in Northland it might be seen as a valley over, not at the front door,” she said.
“We will do everything we can to keep it isolated, but we need everyone to be vaccinated.”
She said decisions were made based on public health advice.
Watch the media conference:
Prime Minister Jacinda Ardern and Māori-Crown Relations Minister Kelvin Davis speak about vaccination in Northland. Video: RNZ News
In the conference, Ardern said the low vaccination rates in Northland are not a failure of the government.
She said the government wants to lift vaccination rates, and wants to remove anything that is a barrier to getting as many people vaccinated as quickly as possible.
“I asked one provider, what are you hearing when you’re out vaccinating … they described it as Covid not necessarily feeling close enough to the community yet, that even when there have been cases in Northland it might be seen as a valley over, not at the front door.”
“We will do everything we can to keep it isolated, but we need everyone to be vaccinated.”
She said decisions were made based on public health advice.
She would rather people were getting vaccinated regardless of alert level, because it was the right thing to do, she said.
Asked about the ruling ordering the ministry of health to reconsider its stance of withholding Māori vaccination data on the basis of privacy, Ardern said it was an issue about what data had been available or able to be shared, and she would allow the health team to work through that.
Raise concerns with professionals
She said people should be able to raise concerns about the vaccine, and if they had questions or concerns they should be able to come forward to talk to health professionals, or someone they trusted, to make the right decision.
She said the number of people who “would be described as … anti-vaccination” was relatively small in New Zealand. She said she absolutely believed the 90 percent double vaccinated rate the government was aiming for could be achieved.
She said young people in particular could be exposed to misinformation online, so there was more work ahead.
Ardern said despite best efforts, cases had come out of Auckland “and so we do need people to be vaccinated”.
Minister Davis said Te Tai Tokerau had not been forgotten.
“I have weekly meetings with all iwi leaders, so there’s a lot of work going into protecting our people, and as we’ve said there’s extra $4m going into the north today. We’re doing everything we can to make sure that our people are protected and people get vaccinated.”
Ardern said the approach from the government had been to ask Māori providers to focus on older kaumātua and kuia, and to take a whānau-based approach.
‘They think they’re smarter than the virus’
Davis was asked about protesters.
“That’s the first protest I’ve seen, there were two people. Obviously, they think they’re smarter than the virus… I don’t think it helps what we’re trying to do here, to protect whānau, to protect whakapapa.
“And to have people think that what’s going on is not reality? I think that they’re just living in a strange world.
“Our focus is on making sure that as many people as possible get vaccinated to protect their whānau, to protect their whakapapa, and that sort of stuff just doesn’t help at all.”
Ardern said misinformation existed everywhere but it was a minority voice.
It is also the region that needs the largest number of first doses to reach 90 percent of the eligible population, with more than 17,000 doses required to reach that milestone.
The government’s proposed traffic light system would see restrictions across New Zealand reduced, and lockdowns ended, once every DHB in the country reaches 90 percent double dosed.
Northland also has a high percentage Māori population. Māori have accounted for about 40 to 50 percent of cases in the delta outbreak in recent weeks, and have lower vaccination rates than the rest of the population.
Demonstrators gathered in Port Moresby yesterday for a march to Parliament in protest over the covid-19 vaccines, which they claimed wrongly to be mandatory, a day after Papua New Guinean police warned such gatherings were illegal.
The protest was a result of a post circulating on social media about a “peaceful protest march” planned for the day against mandatory vaccination.
Despite assurances from Controller of the Pandemic Response and Police Commissioner David Manning that the notice circulated was false and misleading because vaccination was not mandatory and still remained a personal choice, the protesters gathered for the rally.
The anti-vaccine crowd disobeyed advice from the police to disperse. Instead, they took to the Gordon bus stop, gained momentum from others who joined them and attempted to march through a residential street towards the Wardstrip Primary School and on to Parliament.
However, police thwarted their their attempts by blocked the route and spoke to the crowd who disregarded social distancing and masks.
The NCD/Central Assistant Commissioner of Police (ACP), Anthony Wagambie Jnr, addressed the crowd. He said their concerns had already been heard.
It was not clear who the organisers of the march were.
Endangering public safety
ACP Wagambie explained that the march had to be stopped by police to prevent disorder stemmed that would endanger the safety of others in Port Moresby.
The anti-vaxxers carried a banner with messages condemning “666” and “artificial intelligence”.
Misinformation about the covid-19 vaccines is currently swamping genuine information available to Papua New Guineans and is allowing fear and confusion to gain momentum.
Asia Pacific Report reports only 1.2 percent of the nine million Papua New Guineans are vaccinated against covid-19.
According to the John Hopkins University covid dashboard, 29,715 cases of covid and 370 deaths have been reported on Papua New Guinea but health officials fear the real toll is far higher because of limited testing and records.
Of the dozens of patients Dr. Jim Yates has treated for covid-19 at his long-term care center in rural Alabama, this one made him especially nervous.
The 60-year-old man, who had been fully vaccinated, was diagnosed with a breakthrough infection in late September. Almost immediately, he required supplemental oxygen, and lung exams showed ominous signs of worsening disease. Yates, who is medical director of Jacksonville Health and Rehabilitation, a skilled nursing facility 75 miles northeast of Birmingham, knew his patient needed more powerful interventions — and fast.
At the first sign of the man’s symptoms, Yates had placed an order with the Alabama Department of Public Health for monoclonal antibodies, the lab-made proteins that mimic the body’s ability to fight the virus. But six days passed before the vials arrived, nearly missing the window in which the therapy works best to prevent hospitalization and death.
“We’ve been pushing the limits because of the time frame you have to go through,” Yates said. “Fortunately, once we got it, he responded.”
Across the country, medical directors of skilled nursing and long-term care sites say they’ve been scrambling to obtain doses of the potent antibody therapies following a change in federal policy that critics say limits supplies for the vulnerable population of frail and elder residents who remain at highest risk of covid infection even after vaccination.
“There are people dying in nursing homes right now, and we don’t know whether or not they could have been saved, but they didn’t have access to the product,” said Chad Worz, CEO of the American Society of Consultant Pharmacists, which represents 1,500 pharmacies that serve long-term care sites.
Before mid-September, doctors and other providers could order the antibody treatments directly through drug wholesaler AmerisourceBergen and receive the doses within 24 to 48 hours. While early versions of the authorized treatments required hourlong infusions administered at specialty centers or by trained staff members, a more recent approach allows doses to be administered via injections, which have been rapidly adopted by drive-thru clinics and nursing homes.
Prompt access to the antibody therapies is essential because they work by rapidly reducing the amount of the virus in a person’s system, lowering the chances of serious disease. The therapies are authorized for infected people who’ve had symptoms for no more than 10 days, but many doctors say they’ve had best results treating patients by Day 5 and no later than Day 7.
After a slow rollout earlier in the year, use of monoclonal antibody treatments exploded this summer as the delta variant surged, particularly in Southern states with low covid vaccination rates whose leaders were looking for alternative — albeit costlier — remedies.
By early September, orders from seven states — Alabama, Florida, Georgia, Louisiana, Mississippi, Tennessee and Texas — accounted for 70% of total shipments of monoclonals.
Those Southern states, plus three others — Arkansas, Kentucky and North Carolina — ordered new courses of treatment even faster than they used their supplies. From July 28 to Sept. 8, they collectively increased their antibody stockpiles by 134%, according to a KHN analysis of federal data.
Concerned the pattern was both uncontrolled and unsustainable given limited national supplies, officials with the Department of Health and Human Services stepped in to equalize distribution. HHS barred individual sites from placing direct orders for the monoclonals. Instead, they took over distribution, basing allocation on case rates and hospitalizations and centralizing the process through state health departments.
“It was absolutely necessary to make this change to ensure a consistent product for all areas of the country,” Dr. Meredith Chuk, who is leading the allocation, distribution and administration team at HHS, said during a conference call.
But states have been sending most doses of the monoclonal antibody treatments, known as mAbs, to hospitals and acute care centers, sidestepping the pharmacies that serve long-term care sites and depleting supplies for the most vulnerable patients, said Christopher Laxton, executive director of AMDA, the Society for Post-Acute and Long-Term Care Medicine.
While vaccination might provide 90% protection or higher against serious covid in younger, healthier people, that’s not the case for the elders who typically live in nursing homes.
“You have to think of the spectrum of immunity,” Laxton said. “For our residents, it’s closer to 60%. You know that 4 out of 10 are going to have breakthrough infections.”
The mAb treatments havebeen authorizedfor use in high-risk patients exposed to the virus, and experts in elder care say that is key to best practices in preventing outbreaks in senior facilities. That could include, for example, treating the elderly roommate of an infected nursing home patient. But because of newly limited supplies, many long-term care sites have started to restrict use to only those who are infected.
Still, some states have worked to ensure access to mAbs in long-term care sites. Minnesota health officialsrely on a policythat prioritizes residents of skilled nursing facilities for the antibody therapies through a weighted lottery. In Michigan, state Medical Director Dr. William Fales directed emergency medical technicians and paramedics to the Ascension Borgess Hospital system in Kalamazoo to help administer doses during recent outbreaks at two centers.
“The monoclonal antibodies made a huge difference,” said Renee Birchmeier, a nurse practitioner who cares for patients in nine of the system’s sites. “Even the patients in the assisted living with COPD, they’re doing OK,” she said, referring to chronic obstructive pulmonary disease. “They’re not advancing, but they’re doing OK. And they’re alive.”
Long-term care sites have accounted for a fraction of the orders for the monoclonal treatments, first authorized in November 2020. About 3.2 million doses have been distributed to date, with about 52% already used, according to HHS. Only about 13,500 doses have gone to nursing homes this year, according tofederal data. That doesn’t include other long-term care sites such as assisted living centers.
The use is low in part because the treatments were originally delivered only through IV infusions. But in June, the Regeneron monoclonal antibody treatment was authorized for use via subcutaneous injections — four separate shots, given in the same sitting — and demand surged.
Use in nursing homes rose to more than 3,200 doses in August and nearly 6,700 in September, federal data shows. But weekly usage dropped sharply from mid-September through early October after the HHS policy change.
Nursing homes and other long-term care sites were seemingly left behind in the new allocation system, said Cristina Crawford, a spokesperson for the American Health Care Association, a nonprofit trade group representing long-term care operators. “We need federal and state public health officials to readjust their priorities and focus on our seniors,” she said.
In anOct. 20 letterto White House policy adviser Amy Chang, advocates for long-term care pharmacists and providers called for a coordinated federal approach to ensure access to the treatments. Such a plan might reserve use of a certain type or formulation of the product for direct order and use in long-term care settings, said Worz, of the pharmacy group.
So far, neither the HHS nor the White House has responded to the letter, Worz said. Cicely Waters, a spokesperson for HHS, said the agency continues to work with state health departments and other organizations “to help get covid-19 monoclonal antibody products to the areas that need it most.” But she didn’t address whether HHS is considering a specific solution for long-term care sites.
Demand for monoclonal antibody treatments has eased as cases of covid have declined across the U.S. For the week ending Oct. 27, an average of nearly 72,000 daily cases were reported, a decline of about 20% from two weeks prior. Still, there were 2,669 confirmed cases among nursing home residents the week ending Oct. 24, and 392 deaths, according to theCenters for Disease Control and Prevention.
At least some of those deaths might have been prevented with timely monoclonal antibody therapy, Worz said.
Resolving the access issue will be key to managing outbreaks as the nation wades into another holiday season, said Dr. Rayvelle Stallings, corporate medical officer at PruittHealth, which serves 24,000 patients in 180 locations in the Southeast.
PruittHealth pharmacies have a dozen to two dozen doses of monoclonal antibody treatments in stock, just enough to handle expected breakthrough cases, she said.
“But it’s definitely not enough if we were to have a significant outbreak this winter,” she said. “We would need 40 to 50 doses. If we saw the same or similar surge as we saw in August and September? We would not have enough.”
Phillip Reese, an assistant professor of journalism at California State University-Sacramento, contributed to this report.
Leaders of the world’s richest nations wrapped up the Group of 20 Summit in Rome on Sunday after taking virtually no concrete action to tackle the coronavirus pandemic and the intensifying climate crisis, drawing condemnation from human rights advocates who deemed the gathering’s outcome an “abysmal and total failure.”
“G20 leaders could have taken urgent action to dramatically scale up manufacturing and access to Covid-19 vaccines around the world, promote a fair economic recovery, lower dangerous greenhouse gas emissions, and help the poorest countries adapt to the climate change already happening,” Jörn Kalinski, senior adviser at Oxfam International, said in a statement. “The bottom line is that this summit failed to deliver much of anything for people, planet, or prosperity.”
The weekend summit drew to a close as the global death toll from Covid-19 topped a staggering 5 million, a figure that’s likely to continuegrowing by thousandseach day as billions of people worldwide are denied access to lifesaving vaccines.
G20 nations constitute 62% of the global population but have used 82% of the world’s Covid-19 vaccines, according to the London-based advocacy group Global Justice Now. Just3.6%of people in low-income countries have received at least one coronavirus vaccine dose — inequity that threatens to prolong the pandemic and leave the door open to devastating new variants.
A recentanalysisby the science data firm Airfinity showed that G20 countries have received 15 times more coronavirus vaccine doses per capita than countries in sub-Saharan Africa. The United States, the European Union, Britain, and Canada arecurrently hoardingroughly 240 million surplus Covid-19 vaccines as they begin offering booster shots to certain segments of their populations, ignoring the World Health Organization’spleasfor a moratorium on boosters.
“It’s an absolute scandal that the G20 has wasted a year ignoring a proposal, backed by the majority of its members, to break vaccine monopolies and ensure the lifesaving vaccines can be made around the world to save countless lives,” said People’s Vaccine Alliance policy lead Anna Marriot, referring to astalled patent waiverat the World Trade Organization.
At the end of the two-day Rome summit, G20 leaders adopted adeclarationpledging to “enhance our efforts to ensure the transparent, rapid, and predictable delivery and uptake of vaccines where they are needed” and endorsed the WHO’s modest goal of “vaccinating at least 40% of the population in all countries by the end of 2021.” The document does not mention vaccine-related intellectual property rules, which activists view as key barriers to ramping upproduction, closing distribution gaps, and ending the pandemic.
Tamaryn Nelson, a health adviser at Amnesty International, said Sunday that the “vague promises” issued by the heads of the richest countries in the world are “an affront to those who have died, and to everyone still living in fear, of Covid-19.”
“With just two months left of this year, only a radical change in approach will close the shameful vaccine gap,” Nelson argued. “If we continue down our current path, the end of the pandemic will remain a glimmer on the horizon.”
Environmentalists offered similarly scathing rebukes of the climate rhetoric and commitments that emerged from the G20 gathering, which concluded just ahead of the pivotalCOP26 talksin Glasgow, Scotland.
In their final communique, G20 leaders — whose countries are responsible for more than 75% of global greenhouse gas emissions — “acknowledge the close link between climate and energy and commit to reduce emission intensity, as part of mitigation efforts, in the energy sector to meet timeframes aligned with the Paris temperature goal.”
The declaration also includes a vow to “put an end to the provision of international public finance for new unabated coal power generation abroad by the end of 2021.” However, to the dismay of climate campaigners, G20 leaders did not agree to a specific target date to end the use of coal asAustralia and other countriesstood in the way.
“Heads of state from the world’s richest — and therefore most powerful — countries had the opportunity to radically reset multilateral politics and generate the commitments necessary to keep global heating below 1.5°C,”saidNamrata Chowdhary, chief of public engagement at 350.org. “Instead, they’ve made a contradictory and empty statement on climate: they’ve restated their commitment to keeping global heating below 1.5°C, but failed to commit to any action themselves, not even agreeing that their national climate plans must be improved. Right now, they have us on a path to nearly 3 degrees of heating. These so-called leaders need to do better.”
Jennifer Morgan, executive director of Greenpeace International, echoed that sentiment, saying in a statement that “if the G20 was a dress rehearsal for COP26, then world leaders fluffed their lines.”
“Governments must respond to the deadly warnings the planet is giving us and cut emissions drastically right now to stay in line with 1.5°C, and that requires stopping any new fossil fuel development,” said Morgan. “At COP26, we will not let up and continue to push for more climate ambition, as well as the rules and actions to back it up. We need to stop all new fossil fuel projects immediately.”
New Zealand’s cabinet has decided to ease restrictions for some, Prime Minister Jacinda Ardern says cases may peak this month at 200 a day, and Tonga will enter a snap lockdown at midnight.
Restrictions are set to ease slightly in both Waikato and Tāmaki Makaurau, albeit at different times.
Prime Minister Ardern announced at today’s post-cabinet briefing that Waikato would move down to alert level 3 step 2 from midnight Tuesday.
In Auckland, fewer than 5000 first doses remain before reaching 90 percent single-dose vaccination, and for Auckland as a whole 80 percent has had two doses.
“And that’s incredible,” said Ardern, praising Aucklanders for their progress.
“Case numbers, while growing, remain within some of our expectations as modelled and the public health assessment of the impact of changes like opening up retail include that this activity is generally not responsible for marked increases of new cases.”
Meanwhile, cabinet has decided in principle to move Tāmaki Makaurau to alert level 3 step 2 next Tuesday at 11.59pm.
Covid-19 Response Minister Chris Hipkins said potentially slightly easing restrictions in Auckland was a pragmatic move.
Hipkins told RNZ Checkpoint tonight the in-principle decision was based on public health advice.
Covid-19 modeller Professor Michael Plank earlier warned that relaxing restrictions in Auckland and parts of Waikato would accelerate case numbers.
The lockdown will stay in place until next Sunday.
The positive case arrived in Nuku’alofa on a repatriation flight from Christchurch and while he is asymptomatic, he is being cared for alone in a special quarantine facility in Mu’a.
Tonga’s Ministry of Health Chief Executive Dr Siale Akau’ola said the remaining 214 passengers were in MIQ at the Tanoa Hotel while about 80 frontline workers who met the flight are also in MIQ at the Kupesi Hotel.
“In terms of gatherings this is the most significant part of the lockdown. No schools, all schools are closed, no church gathering, no kava club, no entertainment or any kind of gathering,” RNZ Pacific’s correspondent in Tonga, Kalafi Moala, said.
Safety fears as supplement sales soar Sales of natural health supplements have risen since covid-19 arrived in New Zealand, but some products can have adverse effects such as anaphylaxis or death.
Supplements, however, are largely unregulated in New Zealand, with the Ministry of Health saying the pandemic has delayed new legislation.
Ten years of Medsafe data shows two people died from complementary and alternative medicine, or CAM, and that 30 percent of suspected reactions are life-threatening or cause disability.
About eighty percent of New Zealanders have taken natural health supplements, and Nielsen data shows sales in supermarkets alone rose by nearly 14 percent in the past two years, reflecting worldwide trends.
Progress in New Zealand vaccination levels of eligible population. 01112021. Source: Ministry of Health
Police said one of the people has been found and returned to MIQ. He was found during a vehicle stop in west Auckland.
The whereabouts of a woman who also skipped MIQ on Saturday is known to police but public health officials said she did not need to return.
Police said a decision around any charges would be made soon.
Meanwhile, police said a 36-year-old man had been arrested and charged with Failing to Comply with Order (Covid-19) in relation to attending a gathering at the Auckland Domain and subsequent march through Newmarket on Saturday.
Ronapreve covid-19 treatment A covid-19 treatment the government is purchasing can help reduce the number of people dying from the virus, says an expert from the University of Otago.
Pharmac revealed yesterday it is set to subsidise Ronapreve, also known as Regeneron or REGEN-COV, which is used for people in danger of becoming severely unwell.
The World Health Organization’s (WHO) recently released Global Tuberculosis Report for 2021 paints a dismal picture of the impact that the COVID-19 pandemic has had on the fight against TB across the globe.
Progress against TB has long been inadequate to reach the target of elimination by 2030. But before the pandemic the world was making steady progress in diagnosing and treating TB, and deaths from TB had steadily decreased every year since 2005.
The report is based on annual responses to the WHO from 197 countries. It represents around 99% of the world’s population and TB cases and provides annual feedback to the national and international public health community.
This year it contains very worrying news about the COVID-19 pandemic’s wide-ranging and longer term effects on TB services.
For the first time since 2005, the number of deaths due to TB increased from one year to the next. In 2020 there were 1.3 million deaths among HIV-negative people and 214,000 among HIV-positive people. In 2019 the death numbers were 1.2 million among HIV-negative and 209,000 among HIV-positive people.
Mathematical modelling projections for the 16 worst affected countries, including South Africa, suggest the knock-on effect will be worse in 2021 and beyond. These countries are likely to suffer even greater increases in the number of new cases and deaths from TB.
The most urgent priority, according to the report, is to restore access to and provision of TB services to enable levels of TB case detection and treatment to recover to pre-pandemic levels. In the longer term, countries must invest in research and innovation to address the priority needs. These are: TB vaccines to reduce the risk of infection and the risk of disease in those already infected; rapid diagnostics for use at the point of care; and simpler, shorter treatments for TB disease.
Why Gains in TB Control Have Been Reversed
COVID-19 has had a large negative effect on all health services. The effect on TB services has been profound. This is especially the case with regard to TB diagnosis — the essential first step to treating TB and preventing death.
The number of people newly diagnosed with TB had increased annually between 2017 and 2019. But there was a startling drop of nearly 20% between 2019 and 2020 from 7.1 million to 5.8 million. In contrast, the number of TB deaths increased by about 10%, taking us back to 2017 levels.
In the 2021 report, 16 countries accounted for 93% of the total global drop in new TB diagnoses of 1.3 million. The worst affected were India, Indonesia and the Philippines. These three countries are among a group of 10, including South Africa, considered high-burden countries for drug sensitive, drug resistant and HIV-associated TB.
The new data shows that the gap between reality and targets in high burden countries has widened dramatically.
The COVID-19 epidemic has had many consequences for TB services.
patients have delayed seeking care due to restrictions on movement,
reduced likelihood of diagnosis because of resource constraints,
reduced treatment initiation because of medicine supply interruptions and stockouts.
Model estimates of future impact may also be underestimates, as they do not account for the negative effects of COVID-19 on the social determinants of TB. For example, low income and malnutrition increase the chances of developing TB disease in people who are already infected with Mycobacterium tuberculosis, the infectious agent that causes TB disease.
Trend Will Continue Unless the World Acts Now
The increased number of undiagnosed and untreated TB cases will lead to more TB transmission and a further increase in TB disease and death in the years to come unless action is taken now.
TB preventive treatment is given to people who are at high risk of developing TB disease after being infected with Mycobacterium tuberculosis. The WHO recommends that TB preventive therapy be given to people living with HIV, household contacts of individuals diagnosed with TB of the lungs, and certain people with co-morbidities such as those receiving dialysis or diabetics.
Unfortunately, services for TB preventive treatment have also suffered setbacks in the past 18 months. Globally the number of people who received TB preventive treatment had increased by over 250% from 2015 to 2019. But this trend reversed in 2020 with a 21% reduction from 3.6 million to 2.8 million. Substantial action and resources must be directed towards the provision of TB prevention treatment to people who meet the criteria.
The standard of care for drug sensitive TB disease is a six-month course of treatment. On a positive note, the report shows that more countries (36, up from 21) are using newly recommended, shorter treatment regimens for drug susceptible TB.
TB is a leading cause of death in people with HIV. The absolute number of people diagnosed with TB who knew their HIV status fell by 15% in 2020. But the global coverage of HIV testing among people diagnosed with TB remained high in 2020. Treating TB and providing ARVs to HIV-positive people diagnosed with TB is estimated to have averted 66 million deaths between 2000 and 2020.
Catching Up
The first South African National Prevalence survey and other emerging research has shown that only about half of people with active TB disease report having one of the classic symptoms of TB disease: cough, fever, weight loss and night sweats.
This implies that people in the early stages of active TB disease, without any recognisable symptoms, may be contributing to TB transmission without knowing it. It is vitally important that attempts to recover from COVID-19 setbacks, such as catch-up campaigns for case-finding and treatment, involve methods to find people with TB who do not have symptoms as well as those who do.
It is sobering to reflect that, during the 18 months of the COVID-19 pandemic, about 90,500 South Africans have died of TB – more than the 88,754 reported to have died of COVID-19 during the same period. The COVID pandemic has proved that health systems are capable of making drastic changes when the need arises. It is time to apply the same determination to fighting TB.
Indira Govender receives funding from Economic and Social Research Council (UK) and the National Institutes of Health (USA).
Alison Grant receives funding from the Economic and Social Research Council (UK), National Institute of Allergy and Infectious Diseases (USA), Bill and Melinda Gates Foundation, Wellcome Trust. She is affiliated with the South African TB and HIV Think Tanks.
Al Leslie receives funding from the National Institute of Allergy and Infectious Diseases (USA), the Wellcome Trust and the South African Medical Research Council.
Emily B. Wong receives funding from the National Institutes of Health (USA), the Bill and Melinda Gates Foundation and the Wellcome Trust. Members of her lab are funded by the African Academy of Science and the South African Medical Research Council.
Yumna Moosa receives funding from the South African Medical Research Council and the Sub-Saharan African Network for TB/HIV Research Excellence (SANTHE).
New Zealand has reported 143 new community covid-19 cases today – 135 in Auckland, six in Waikato and two in Northland.
There were no community cases in Christchurch today. One previously reported case in the city has been reclassified as a historical case, so the total Christchurch tally is now four.
There was no media conference today. In a statement, the Ministry of Health said that because of the recently reported cases in Canterbury, it was important that anyone with any symptoms — no matter how mild — got tested.
The ministry said 73 cases were still to be linked.
There are 384 unlinked cases from the past 14 days.
The ministry said the reported number of cases in Auckland “is not unexpected and is line with modelling to date”.
Fifty-six people are in hospital, up from 47 yesterday. Two are in intensive care.
There were no cases detected at the border today.
There have now been 3348 cases in the current community outbreak, and a total of 6068 cases since the pandemic began.
There were 42,617 vaccines given yesterday, including 10,703 first doses and 31,914 second doses.
More locations of interest in Northland The two Northland cases reported today were announced yesterday and have been formally added to the official tally today.
There have now been 12 confirmed covid-19 community cases in Northland in the current outbreak. All of the cases are isolating at home.
Tonga traveller contacts The ministry said the four household contacts of the person who reportedly tested positive for covid-19 in Tonga yesterday have been traced, are in isolation and have returned an initial negative result.
Two close contacts are in isolation at home in Christchurch and two in Porirua.
“Anyone with symptoms is asked to please get tested and reminded to get vaccinated today if they have not already. Testing locations in the Wellington region can be found at Capital and Coast DHB and Hutt Valley DHB.”
A man infected with covid-19 was yesterday reported to have broken out of an Ellerslie MIQ hotel in Auckland, but was caught by police less than half and hour later and has been arrested.
New Zealand has reported eight new covid-19 cases, including seven residents, at an Auckland retirement village, adding to one announced yesterday.
This was part of a jump to a total of 160 new community cases reported today — 151 in Auckland, seven in Waikato and one each in Northland and Canterbury.
Following further testing at Edmonton Meadows retirement village in Henderson, the seven residents and one staff member have been confirmed as having the virus, bringing the total number of cases at the home to nine, the Ministry of Health said in a statement.
The ministry said it was important to point out the village had high levels of vaccination among residents of the home, and all staff are fully vaccinated.
All staff and residents have now been tested and will also receive day five and day 12 testing.
Auckland Regional Public Health staff are supporting the residents and staff at the privately owned facility.
At this stage, only one positive staff member has been required to stand down.
Investigation seeking source
An investigation has begun to try and find out the source of the infection.
The retirement village has been operating under alert level 3 guidelines for visitors, meaning people have only been able to visit the village on compassionate grounds.
Meanwhile, the focus today in Auckland remains on testing in areas identified as having higher positivity rates, where the risk of unidentified cases is higher.
Public health staff are asking people in the suburbs of Redvale, Rosedale, New Lynn, Wiri, Drury, Henderson and Manurewa with symptoms to get tested — no matter how mild their symptoms may be.
The advice is the same even if people are vaccinated.
There are 16 community testing centres available for testing across Auckland today. Up-to-date information on testing locations in Auckland, visit here.
There was no media briefing today. In a statement, the ministry said 95 of today’s cases were still to be linked and there had been 358 unlinked cases in the past 14 days.
There are 47 people in hospital, up from 37 yesterday. Two are in intensive care.
Tonga’s Prime Minister is urging people on the main island of Tongatapu to use the weekend to prepare for a potential lockdown next week after the kingdom’s first covid-19 case was confirmed.
The positive case was a passenger on a repatriation flight from Christchurch with 215 other people on Wednesday.
The passengers from the Christchurch flight are quarantined in the Tanoa Hotel, Nuku’alofa.
Dr Pohiva Tu’i’onetoa said the reason the lockdown would not happen this weekend was because he had been advised that the virus would take more than three days to develop in someone who caught it before they became contagious
Tongan PM Dr Pohiva Tu’i’onetoa … no lockdown over the weekend. Image: RNZ Pacific/Tongan govt
Matangi Tonga Online reports the prime minister announced at a press conference that Tongans should use this time to get ready in case more people were confirmed they had the virus.
The Ministry of Health’s CEO Dr Siale ‘Akau’ola explained that if the covid-19 virus entered a person, that person could not spread it right at that time, the virus needed time to grow and that person would become infectious three to five days after contracting it.
“Frontliners should be safe because even if say the [quarantine bus] driver returned home that night, and whether he wore PPE or not, if he contracted the virus then there is that incubation period where it grows, becoming infectious three or more days after. That is why I think they are alright,” Dr ‘Akau’ola said.
Chief executive of Tonga’s Ministry of Health Dr Siale Akauola … “I think they [frontliners] are alright.” Image: RNZ Pacific/Christine Rovoi
He said that when they got the news just before midnight of two positive community cases in Christchurch, they had informed the frontliners involved and they self-isolated at home.
Then after the covid-19 positive test was confirmed yesterday in Tonga, the frontliners were also taken into quarantine.
“So, we have acted swiftly in just a day,” he said. “Our frontliners are trained and have been fully vaccinated.”
Health officials say the passenger who tested positive to covid-19 was inoculated with the first dose of the Pfizer BioNTech vaccine in the last week of September, and had received a second dose in mid-October.
“So the person is fully vaccinated and their protection level will be up two weeks after this second shot,” Dr ‘Akau’ola said.
“We are satisfied despite this person being positive, we believe the person would not get seriously ill and reach a dangerous level.”
Tanoa Hotel in Nuku’alofa … the quarantine venue. Image: RNZ Pacific/Tanoa Hotel
Meanwhile, it has not been confirmed if the covid-19 virus is the delta variant, which spreads easily.
“When there is a covid-19 positive case we can assume it’s delta, then confirm later,” he said.
People can still get their covid-19 vaccinations over the weekend including on Sunday.
Dr ‘Akau’ola confirmed Health would still be providing vaccinations even if there was a lockdown.
Fully vaccinated Meanwhile, New Zealand’s Ministry of Health confirmed that the case had returned a negative pre-departure test before leaving New Zealand and was fully vaccinated and had their second dose on October 15.
Passengers on the flight, including members of Tonga’s Olympic team who had been stranded in Christchurch, were required to provide a negative covid test result at least 72 hours before boarding.
They also had to show vaccination cards prior to the flight, with dates for first and second doses.
The Olympic team were double vaccinated before they departed Tonga for the Olympic Games in Japan.
This article is republished under a community partnership agreement with RNZ.
This content originally appeared on Asia Pacific Report and was authored by APR editor.
In May 2018, a rare and virulent strain of salmonella caught the attention of America’s top disease detectives. In less than two months, the bacteria had sickened more than a dozen people, nearly all of them on the East Coast. Many said they’d eaten chicken, and federal food safety inspectors found the strain in chicken breasts, sausages and wings during routine sampling at poultry plants.
But what seemed like a straightforward outbreak soon took a mystifying turn. Cases surfaced as far away as Texas and Missouri. A 1-year-old boy from Illinois and a 105-year-old woman from West Virginia fell ill. There was a teenager who’d just returned from a service trip in the Dominican Republic and a woman who’d traveled to Nicaragua. But there were also people who hadn’t traveled at all.
Victims were landing in the hospital with roiling stomach pains, uncontrollable diarrhea and violent bouts of vomiting. The source of the infections seemed to be everywhere.
Even more alarming was that this strain of salmonella, known as multidrug-resistant infantis, was invincible against nearly all the drugs that doctors routinely use to fight severe food poisoning.
With a public health threat unfolding across the country, you might have expected federal regulators to act swiftly and decisively to warn the public, recall the contaminated poultry and compel changes at chicken plants. Or that federal investigators would pursue the root cause of the outbreak wherever the evidence led.
None of that happened.
Instead, the team at the Centers for Disease Control and Prevention closed the outbreak investigation nine months later even though people were continuing to get sick. The U.S. Department of Agriculture, which oversees meat and poultry, was not only powerless to act but said nothing to consumers about the growing threat. So supermarkets and restaurants continued selling chicken tainted with drug-resistant infantis.
And they continue to do so today.
An eight-month ProPublica investigation into this once rare, but now pervasive form of salmonella found that its unchecked spread through the U.S. food supply was all but inevitable, the byproduct of a baffling and largely toothless food safety system that is ill-equipped to protect consumers or rebuff industry influence.
Several European countries have dramatically reduced salmonella in poultry by combating it on the farms where chickens are raised. But over the past 25 years, the U.S. has failed to bring down the incidence of salmonella food poisoning — even as the rates for E. coli and other bacteria have fallen dramatically.
Consumers may get the impression that the meat and poultry they find at supermarkets is safe because it bears the USDA seal of approval. But the agency doesn’t prohibit companies from selling chicken contaminated with dangerous salmonella like infantis. And even when people get sick, it has no power to order recalls.
Instead, the agency relies on standards it can’t enforce and that don’t target the types of salmonella most likely to make people sick. The USDA’s Food Safety and Inspection Service, unlike its counterparts in some countries, has no authority to control salmonella on farms, where the bacteria often spreads. And even when there’s persistent evidence of contamination in a plant’s products, the USDA can’t use those findings to suspend operations. All the agency can do is conduct a general review of the plant, and that rarely leads to a shutdown.
“It’s a system that’s untenable,” said Sarah Sorscher, a consumer advocate at the Center for Science in the Public Interest.
Last week, after repeated interview requests from ProPublica and years of criticism from consumer groups, the USDA announced that it was rethinking its approach to salmonella. The agency didn’t announce any concrete changes but said it would set up pilot projects and hold meetings in an effort to come up with a plan.
“Whether it should have been done sooner or could have been done sooner, the good news is we’re doing it,” said Sandra Eskin, the agency’s deputy undersecretary for food safety. “We’re going to really take a look at everything we could look at and, I hope, develop a different approach that winds up being more effective.”
Scientific advancements over the last decade have provided the USDA with tools to identify the most dangerous strains of salmonella. But the agency isn’t using those tools to prevent it from spreading in our food supply.
To piece together how food safety officials and the poultry industry allowed infantis to spread, ProPublica used the same genetic data available to the USDA and other agencies, analyzing seven years of infantis samples taken from food and patients and catalogued by the National Institutes of Health.
Through dozens of public records requests, ProPublica was then able to link the genetic information on those 8,000 samples to the foods that victims ate and the processing plants the chicken samples came from.
The analysis, along with hundreds of internal government records and interviews with nearly two dozen scientists, allowed us to uncover that the infantis outbreak never abated and has continued to run rampant through the chicken industry.
In fact, ProPublica found that more than twice a day this year, on average, USDA inspectors detected multidrug-resistant infantis in poultry that’s genetically similar to the outbreak strain. Each month, the CDC continues to receive dozens of reports of people getting sick from it.
“Many people are still becoming ill, and some of them gravely ill,” Robert Tauxe, director of the CDC’s Division of Foodborne, Waterborne and Environmental Diseases, told ProPublica.
One internal CDC presentation noted that this single strain is “responsible for an estimated 11,000-17,000 illnesses per year.” But the CDC is limited in its ability to protect American consumers from foodborne illnesses. It has no power to order companies to take action or to provide information that would help it solve outbreaks.
And the CDC, despite noting that the strain was “widespread in the chicken industry,” took the spotlight off infantis when it closed its outbreak investigation in February 2019. Tauxe said the investigation ended because the agency had learned as much as it could. “That does not mean that the outbreak was over,” he said. “In fact, we think it may still be expanding.”
As the CDC has contended with infantis, the agency has held several private meetings with the chicken industry, which has publicly downplayed the threat of the strain and its ability to do something about it.
But since closing the investigation, neither federal health officials nor the USDA has said anything to consumers about what the CDC quietly regards as an “epidemic.”
Marva Lamping knew none of this in July 2019 when she took her longtime partner, Arthur Sutton, out to celebrate his 70th birthday at their favorite Mexican restaurant in Bend, Oregon. As Lamping tested her luck at the restaurant’s video slot machines, Sutton snacked on chips and salsa while waiting for a platter of chicken enchiladas.
That night, Sutton began vomiting repeatedly, his stomach aching so badly that he couldn’t lay down. By the next morning, the pain was unbearable, and Lamping rushed him to the emergency room.
At the hospital, doctors would discover that Sutton’s intestines were leaking. Again and again, surgeons opened his abdomen to repair the tears and cut out dead segments of his bowels.
Doctors had quickly identified the cause of Sutton’s ailments as salmonella. But for reasons they couldn’t understand, his body was wasting away.
None of the antibiotics were working.
Missed Opportunities
As sudden as the infantis outbreak seemed to investigators at the CDC, it wasn’t the first time the government had seen this strain, known as Infantis Pattern 1080. In the three years before the outbreak started, USDA inspectors had found the strain 74 times. But they could do nothing to stop the chicken from going to supermarkets and restaurants nationwide.
By the summer of 2018, people all over the country were falling ill. And as investigators studied the cases, clues soon emerged from the USDA, which oversees meat and poultry, and the Food and Drug Administration, which regulates almost all other foods.
The FDA had received a complaint that a dog had recurring diarrhea after eating raw pet food, and samples of chicken-and-vegetable dog food tested positive for multidrug-resistant infantis. A few months later, a Chicago woman fell sick with the outbreak strain after feeding her dog the same brand. Could the pet food be the source of the outbreak? Possibly, but not all the victims had a dog.
There was another lead. Victims reported eating Perdue Farms chicken more than any other brand. Public health officials in Pennsylvania and Minnesota found the outbreak strain in packages of Perdue wings, thighs and drumsticks in three supermarkets. And when USDA inspectors found the strain in raw chicken, more than a quarter of the samples came from Perdue plants.
The FDA’s investigation had quickly led to a pet food recall. But while the FDA prohibits salmonella in the foods it oversees — including dog and cat food — the USDA allows it in raw meat and poultry destined for human consumption.
When people fall ill, the USDA can only request that a company voluntarily recall its products. But to do even that for salmonella, regulators face a high bar: To ensure a strong case, they’re expected to try to find a patient with an unopened package of meat that tests positive for the same strain that made the outbreak victims sick.
“Often, by that time, most of the meat that’s going to be eaten has been eaten,” said Sorscher of the CSPI.
In June 2018, what could have been a key piece of evidence surfaced. An Illinois victim who’d been hospitalized told investigators that he still had a package of Perdue chicken tenders in his freezer. The USDA could have tested the package, but nobody ever went out to collect it, he said.
Perdue did not respond to more than a dozen calls and emails seeking comment, and it didn’t answer questions sent to top company officials.
Wade Fluckey, Perdue’s senior director of food safety at the time, told ProPublica that the company was targeted because Perdue has better brand recognition than other chicken companies, which skewed patient interviews.
“I don’t know that any one company could say they didn’t have it,” said Fluckey, now a vice president at a pork processor. “Had they focused on other places, they would have found the same thing.”
While no company showed up more frequently than Perdue, food inspectors were finding the Pattern 1080 strain in dozens of chicken processing plants as well as raw pet food and live chickens. To investigators, that was unusual because it meant that the salmonella couldn’t have come from a single company or chicken product. It had to be coming from somewhere upstream in the supply chain — perhaps the farms or the few companies that breed nearly all the nation’s chickens.
The country’s antiquated meat safety system virtually ensured it would be no match for a germ like infantis.
The USDA operates under a law passed in 1906, where inspectors physically examine every carcass for signs of animal disease, illegal additives and spoilage. The system didn’t account for invisible pathogens like salmonella and E. coli, which had not yet been linked to eating meat.
That did not change until 1994 after four children died from eating Jack in the Box hamburgers. The USDA made it illegal to sell meat tainted with a strain of E. coli called O157:H7. But it didn’t ban salmonella despite a series of high-profile outbreaks in chicken. Instead, the USDA required processing plants to limit how often salmonella was found on their products and began testing for it. Plants that repeatedly violated these standards faced a shutdown.
That powerful threat didn’t last long. In 1999, a Texas meat processor challenged the USDA’s authority to close plants, arguing that salmonella “appears naturally” in raw meat. Two years later, the 5th U.S. Circuit Court of Appeals agreed that Congress hadn’t given the agency the power to regulate salmonella that’s present before products enter processing plants or to deem a facility unsanitary based on the bacteria alone.
The decision, Supreme Beef Processors v. USDA, has left the agency gun-shy, according to former department officials and food safety advocates. And Mansour Samadpour, a microbiologist who runs a testing and consulting firm that works with the food industry, said the decision distorts the underlying science. Just because salmonella “colonizes” chickens’ guts doesn’t mean it’s “the natural state of the animal,” he said. “It’s nonsense.”
The court ruling severely clipped the USDA’s powers. So it has tried to pressure plants to improve by creating standards for how often salmonella should be found. Plants are rated on the results, which are published online. Violating those standards doesn’t carry a penalty, but it allows the agency to visit the plant and look for more general problems like unsanitary conditions. If they can document significant problems, the USDA can temporarily shut down the plant, though the agency rarely takes such action.
Today, food poisoning sickens roughly 1 in 6 Americans every year, according to the CDC, and salmonella hospitalizes and kills more people than any other foodborne pathogen. Each year, about 1.35 million people get sick from salmonella. While most recover, more than 400 people die and 26,500 people are hospitalized. Some are left with long-term conditions like severe arthritis and irritable bowel syndrome. Salmonella costs the economy an estimated $4.1 billion a year, more than any other type of food poisoning.
Salmonella outbreaks have been linked to other foods likeonions, but poultry remains the biggest culprit, and people are eating more of it than ever. On average, people in the U.S. eat nearly 100 pounds of chicken each year, a number that has grown by about 40% in the last 25 years.
Cooking poultry to an internal temperature of 165 degrees will kill salmonella. But studies by the USDA and others have found that despite decades of consumer education, home cooks routinely cross-contaminate their kitchens, and few use a meat thermometer to ensure their poultry is cooked properly.
Illnesses haven’t declined even as salmonella rates in raw poultry have. And infections are getting harder to treat. The CDC recently found that salmonella infections were becoming increasingly resistant to antibiotics. In contrast, food poisoning related to E. coli O157:H7 has dropped by about 70%.
Consumer advocates, industry consultants and former USDA officials say that’s because the agency focuses solely on whether salmonella is found in chicken or turkey at the processing plant.
This approach has been criticized for years. One former meatpacking executive called it “worthless.” Even the USDA’s own research arm has said the agency’s measure for salmonella is “not a good indicator” of food safety.
The USDA doesn’t consider two key risk factors: how much salmonella is in the poultry and how dangerous that type of salmonella is. There are 2,500 types of salmonella, but only a fraction cause the vast majority of illnesses.
The industry has greatly reduced the prevalence of one common type of the bacteria, known as salmonella Kentucky, which rarely causes illnesses in the U.S. But it’s made far less progress with the types of salmonella most likely to make people sick, the ProPublica analysis found.
The rate of infantis, for example, has more than quintupled over the past six years.
The full extent of the salmonella problem isn’t even known. The agency does little testing for salmonella to begin with. On an average day in 2020, the USDA took about 80 samples of raw poultry across hundreds of processing plants. But those plants slaughter more than 25 million chickens and turkeys a day.
In recent years, consumer advocates have recommended the agency ban the sale of raw meat carrying the types of salmonella that most often make people sick. That approach has contributed to improvements in Europe. In the U.S., the FDA has seen a dramatic decrease in salmonella outbreaks tied to eggs since the 1990s when it began targeting the most common type.
Last month, a few of the largest poultry companies, including Perdue and Tyson, joined with the CSPI and other consumer advocates to urge the USDA to fix the system. But the letter to the agency didn’t outline specific reforms, and a consensus on salmonella regulations has long proved elusive.
The last push came during the Obama administration, but citing the need for more data, the USDA rejected a proposal to ban certain antibiotic-resistant strains. The agriculture secretary at the time was Tom Vilsack, who now leads the agency again under President Joe Biden.
As the food safety project director for the Pew Charitable Trusts before joining the USDA, Eskin also pushed for reform, but her efforts were met with resistance. With food safety directors from some of the largest companies, she helped craft recommendations to Congress to modernize the meat safety system, including setting new limits on salmonella contamination and giving regulators oversight of farms.
The group sought to enlist trade associations, which represent not only the biggest players but hundreds of other companies. But when it comes to regulation, divergent interests often leave the trade groups lobbying for the lowest common denominator. “They shut us down,” she said in an interview before taking her government post. “They’re the ones that blocked us — not the companies, the trade associations.”
Asked what was standing in the way of change, she said, “I’ll make it simple: Powerful interests in the industry do not want it.”
“We Are Basically Only Talking About Protecting Industry”
Just months before the infantis outbreak started, the USDA gathered representatives from the food industry, researchers and regulators at the agency’s brick-and-limestone headquarters in Washington to discuss a scientific breakthrough that one participant called the “biggest thing” for food safety in 100 years.
Whole-genome sequencing had given food safety researchers an unprecedented look at the DNA of foodborne bacteria. New technology, known as “next-generation sequencing,” was creating a trove of new information and revealing connections that could help investigators stop outbreaks before they spun out of control.
As stakeholders took turns presenting slides in the wood-paneled auditorium, some spoke of the possibility that genome sequencing might help solve the stagnant rate of salmonella poisoning.
The new technology would help identify pathogens in foods like raw flour, peaches and romaine lettuce that were once rarely seen as sources of outbreaks.
While whole-genome sequencing couldn’t confirm the source of an outbreak without additional evidence, it provided powerful clues about the bacteria’s genetic history that could point epidemiologists in the right direction.
But for all the potential, much of the conversation that day in October 2017 centered on how to make this scientific breakthrough palatable to industry. Trade groups had requested the meeting, and they voiced concerns about how the new tool could be used for enforcement or might inaccurately connect companies’ products to outbreaks. Speakers, including USDA officials, emphasized the importance of proceeding with caution. They discussed strengthening firewalls to keep testing data private and establishing “safe harbors” from USDA enforcement.
During a roundtable discussion, one representative from the United Fresh Produce Association raised concerns about the idea of companies sharing genome sequencing data with the government. “I think right now, it’s viewed as very one-sided,” she said. “We see the benefit to the agencies, but it’s less clear how a company would directly benefit.”
The industry’s influence wasn’t lost on regulators. Former USDA officials hold key posts at some of the food industry’s biggest companies. Indeed, two people who led the 2017 meeting for the agency now work for the food industry.
Sitting in the auditorium, Jørgen Schlundt, the former head of food safety for the World Health Organization, was growing increasingly frustrated. Schlundt had helped achieve dramatic reductions in salmonella in Denmark while working for the country’s food agency.
“I understand that I’m in the U.S., but surely this must also be about protecting consumers,” he told the audience. “We are basically only talking about protecting industry here. I thought that this was, the basic purpose was to protect consumers, avoid American consumers and other consumers from dying from eating food.”
While the USDA tiptoed around the new technology, whole-genome sequencing, which is now used to solve criminal cases and track COVID-19 variants, would prove pivotal to the CDC’s infantis investigation.
As the infantis outbreak spread, epidemiologists noticed something unusual: The outbreak strain, Pattern 1080, carried an unusual combination of antibiotic-resistance genes that looked similar to another strain they’d seen before, Louise Francois Watkins, an epidemiologist at the CDC, said in an interview.
At the time, the CDC was still using a method called pulsed-field gel electrophoresis, or PFGE, which produced barcode-like patterns from the bacteria’s DNA that scientists used to connect cases. So the investigators asked the lab to line up the patterns and compare the two strains.
“And sure enough,” Francois Watkins said, the strains were so similar, they differed by “only a single band” of the barcode. With that clue, they decided to analyze the strains using whole-genome sequencing.
That allowed scientists to compare the individual building blocks in the genomes of bacteria. And the infantis investigators discovered that not only were the two strains genetically similar but that PFGE was masking the scope of the problem.
In fact, Pattern 1080 was just one wave in a much larger surge of drug-resistant infantis — one that had been detected nearly a decade ago in Israel and was now circulating worldwide in countries as far apart as Italy, Peru and Vietnam.
One of the reasons the U.S. variant is so concerning is that it typically carries a unique gene that makes it especially hard to treat.
“It’s resistant to four of the five antibiotics that are commonly recommended for treatment,” Francois Watkins said. “The antibiotics that your doctor is going to pick when they suspect you have a salmonella infection are pretty likely not to be effective.”
The strain is also a major public health concern because it has the ability to pass those genes to other bacteria, adding to the growing global problem of antibiotic resistance.
“We don’t want to see resistance climbing in our food supply because it’s not going to stay in that one space,” Francois Watkins said.
Whole-genome sequencing had helped investigators discover that the outbreak was actually a widespread problem in the country’s chicken supply.
But even with these new revelations, public health officials still lacked one of the most basic tools to control the strain.
“A Gap in Our Regulations”
CDC investigators knew that infantis was spreading in chickens long before the birds arrived at the slaughterhouse. But enlisting the USDA’s Food Safety and Inspection Service would be a dead end because the agency has no regulatory authority over farms. The USDA can only force farms to take measures when animals get sick, not when humans do.
That also made it difficult for the CDC investigators to pursue leads involving breeders and feed suppliers to trace back how dangerous bacteria got into the food supply.
“That’s a gap in our regulations,” Tauxe of the CDC said.
Nearly all the chickens we eat descend from birds bred by two companies, Aviagen and Cobb-Vantress, a subsidiary of Tyson Foods. This breeding process has allowed consumers to walk into any grocery store and find chicken of the same quality. But that pyramid structure also makes it possible for salmonella to circulate since the bacteria can be transferred from hens to their offspring, and a single breeding flock might produce 3 million chickens over several years. (Both companies declined to comment.)
And nearly every step of their journey from chicken house to our plates presents an opportunity for salmonella to spread.
When chickens are raised in crowded conditions, bacteria can proliferate through close contact, contaminated feed and communal water, and pests or farmworkers’ boots as they move between flocks. Salmonella can also develop in poultry litter, the organic material like sawdust that’s spread on chicken house floors. As time passes, it becomes increasingly soaked in excrement, serving as a “reservoir of salmonella contamination,” according to the USDA. In some countries, such as Sweden and Mexico, the bedding is typically changed after every flock, or about every five to seven weeks. But in the U.S., the litter is treated and turned over but often changed only once a year, according to the Agriculture Department.
As far back as 2005, the USDA has held public meetings exhorting the poultry industry to take steps at the farm. It has recommended that farmers change or chemically treat the litter between flocks, use traps and bait to eliminate pests and vaccinate hens and chicks against salmonella.
Denmark, Sweden and Norway have largely eradicated salmonella on farms by keeping chicken houses clean, frequently testing the birds and destroying infected breeding flocks.The United Kingdom has dramatically reduced salmonella illnesses by pressuring the industry to vaccinate.
The structure of the U.S. chicken industry makes it ideally suited to implement such interventions. The same company that slaughters the chickens often owns the hatchery and feed mill, and it contracts with farmers to raise the chickens to its specifications. The catch is that because companies are essentially doing business with themselves, there’s little incentive for any of them to press others to reduce salmonella, the industry consultant Samadpour said.
“If it was four or five different companies,” he said, “the processing plant would tell the farms, ‘If you are more than so much positive, you can’t send it here,’ the farm would tell the hatchery, ‘If the chicks coming in are positive, we are not going to take them.’ They would tell the feed mill that if the feed is contaminated with salmonella, ‘We are not going to bring it in.’ Can you do that? No, it all belongs to you.”
Because more isn’t done on the farm, the birds’ skin and feathers are often highly contaminated with salmonella by the time they reach the processing plant, according to the USDA. And in the plant, there are many ways bacteria can spread.
To loosen their feathers, chicken carcasses are dunked into a tank of scalding water. This step can remove dirt and feces. But if the water isn’t managed properly, it becomes fetid, spreading bacteria among the birds. Next, mechanical rubber fingers pluck the feathers, a process that also dislodges feces and massages dirty water into the now-open follicles.
When the birds’ internal organs are removed, they can rupture, spilling intestinal contents onto machinery.
One of the main ways processing plants fight salmonella is the chiller. Here, a bubbling tank of near-freezing water and chemicals decontaminates the birds and reduces their temperature to limit bacterial growth. But researchers say salmonella survives when plants overload the chiller with carcasses.
Birds can be further cross-contaminated when workers cut carcasses into breasts, legs and wings. The USDA recommends workers wash their hands and sanitize knives between each bird. But workers often have a few seconds to make each cut.
Ground chicken, which has become increasingly popular, is especially prone to contamination. Meat sent to the grinder comes from multiple birds, increasing the chance of cross-contamination. The fine texture of ground chicken can also get caught in small pieces of equipment, potentially tainting multiple batches.
While salmonella is found in 8% of the chicken parts tested by the USDA, 25% of ground chicken samples contain the bacteria.
And when the USDA tested for salmonella during the infantis outbreak, more than half of the positive samples were found in ground chicken.
“The Company Can Do Whatever It Wants”
In July 2018, as outbreak investigators began to discover infantis in Perdue products, the USDA had a chance to press the company for answers. Routine salmonella testing had found thatthe company’s plant in Cromwell, Kentucky, was exceeding the USDA’s salmonella standards, which say no more than 15.4% of chicken parts at a plant should test positive for the pathogen.
So USDA staff were sent to conduct an assessment of the plant, which might have seemed well-timed. Of the 76 plants where the infantis outbreak strain had been found, Cromwell, with 8% of the positive samples, had more than any other facility. But failing the agency’s salmonella standard doesn’t give the USDA the power to do anything more than review the plant’s practices.
The USDA noted that Perdue had responded to its high rate of salmonella by adding more chemical dip tanks and sprays to disinfect the chicken. Because Perdue’s internal sampling data showed the new steps appeared to be reducing the bacteria, the agency gave Perdue more time and recommended “no further action be taken.”
According to the USDA report, Fluckey, then the food safety director at Perdue, told auditors that the agency’s testing didn’t paint an accurate picture of the plant because it wasn’t measuring the quantity of salmonella. He added that Perdue managers hadn’t concentrated on the salmonella types most likely to make people sick because they were focused on “meeting the performance standard.”
A year later, USDA sampling indicated that the plant had continued to violate salmonella standards, with a third of chicken parts testing positive for the bacteria. In addition, the USDA said 12 of Perdue’s samples were highly related genetically to samples from people who’d recently gotten sick.
Still, the agency once again deferred to the company’s testing results, which showed a decrease in the rate of salmonella at the plant. The USDA decided it couldn’t cite the plant and that no action was necessary.
ProPublica found that many plants have repeatedly violated the agency’s standards without being shut down or facing any recent public sanction. According to the most recent data, more than a third of the plants producing ground chicken are violating the USDA standard. And many large companies — including Tyson, Pilgrim’s Pride, Perdue, Koch Foods and the processors that produce chicken for Costco and Whole Foods — currently have plants with high rates of the types of salmonella most likely to make people sick.
Whole Foods said it has a team of experts who review the salmonella results of its suppliers and works with them to lower their salmonella rates. The processor,Pine Manor Farms, said it has “worked diligently to make corrections.” Tyson and Costco declined to comment; Pilgrim’s and Koch didn’t respond to questions.
Other Perdue plants where the infantis outbreak strain was found also had a poor track record with salmonella overall. In the last three years, its plants inRockingham, North Carolina, andGeorgetown, Delaware, had more than 35% of their ground chicken samples test positive for the bacteria, and nearly all of them were types commonly linked to human illnesses. Yet neither plant has faced any recent public enforcement action, according to a review of USDA reports. (In April, ProPublica requested detailed files for both plants, but the USDA has yet to provide them.)
In an interview before she joined the USDA, Eskin said the consequences for companies violating the standards aren’t “anything meaningful in terms of enforcement.” “At the end of the day,” she said, “I think the company can do whatever it wants.”
The USDA doesn’t appear to have traced the supply chain for the plants that tested positive for the outbreak strain. Detroit Sausage had one of the highest numbers of samples with the strain.
Phil Peters, one of the owners, said he doesn’t remember anyone from the USDA asking the company who supplied its chicken. “I can’t control something that’s coming in from somewhere else unless I stop using it,” he said.
The company no longer produces chicken sausage because his clients no longer order it. But as a small processor, Peters said, he has little ability to demand chicken companies provide him meat carrying less salmonella. “They’re too big to worry about us,” he said.
A Hidden “Epidemic”
With no powers of its own and stuck with a hesitant regulator in the USDA, the CDC’s investigators needed the industry’s help.
On Aug. 8, 2018, the CDC offered a stark assessment of the outbreak to representatives of the industry’s trade group, the National Chicken Council: Drug-resistant infantis had become a “particular clinical and public health concern” because it was spreading through the chicken industry and increasingly making people sick.
The USDA seemed to take a less urgent approach. After an Aug. 16 foodborne illness investigations meeting with infantis on the agenda, an agency official wrote that there were “zero active illness investigations.” The USDA had begun tracing victims’ grocery purchases, but beyond that, it decided infantis was an “illness cluster” to watch — not a situation that required additional resources.
By then, three months into the outbreak investigation, neither the CDC nor the USDA had said anything to consumers.
People continued to get sick. Twelve days after the USDA meeting, a New York City resident began having stomach cramps. The patient’s spouse told investigators the victim had eaten and shopped in the Flatbush section of Brooklyn. The patient went to the hospital but died two days later, the first known fatality from the infantis outbreak.
For nearly two months, there was still no public warning.
In October 2018, the CDC privately met again with the National Chicken Council. By then, public health officials were convinced that the outbreak strain originated high up in the chicken supply chain.
“The outbreak strain may be persisting in chicken populations, their environments or their feed,” according to the CDC’s presentation to the industry group. “Further investigation is needed to help prevent new illnesses and similar outbreaks in the future.”
The CDC drew up a list of questions for the National Chicken Council:
How was it possible that so many different companies could have the same strain of salmonella infantis? Were common sources of chickens, eggs or other farming products widely used? Would one or more companies be willing to partner with the CDC and USDA to explore possible connections?
The council didn’t have many answers. According to a government official’s notes, the industry said that it “does a lot to try to reduce salmonella across the board,” but that it didn’t have a specific preventative measure for infantis. An industry representative added that it “might have been helpful to have the discussion 4 years ago,” when the first signs of drug-resistant infantis popped up in processing plants.
A few days after the October meeting, a 2-year-old Michigan girl began rubbing her belly before developing a fever and diarrhea, making her the latest Pattern 1080 patient. Her parents said that before she got sick, she’d eaten chicken nuggets and touched a package of raw chicken in their kitchen.
The next day — more than nine months after the first patient from the outbreak got sick — the CDC issued its first public notice. By then, 92 people in 29 states had been infected with the outbreak strain. But the number was likely far higher: The CDC estimates that for every confirmed salmonella case, an additional 30 are never reported. That meant that nearly 3,000 people had likely been infected.
Though the CDC knew that infantis wasn’t a typical outbreak strain, the notice offered little advice to consumers other than to remind them to follow standard food safety steps when handling raw poultry. The CDC told ProPublica that there was little more it could say to consumers. Infantis was so pervasive, Tauxe said, that the CDC couldn’t tell consumers to avoid any specific kind of chicken or brand.
Instead, public health officials held another private meeting with the chicken industry in February 2019, telling trade organization officials that they considered this strain of infantis to be an “epidemic.”
The CDC emphasized how risky this particular bacteria was because of its resistance to first-line drugs used to treat salmonella, especially illnesses involving children and patients with blood infections.
Health officials also presented the clues that had pointed toward Perdue as a potential source of some of the illnesses. The agency wanted to sit down with Perdue, but with no power to compel the company to answer questions, it would be months before a meeting happened.
A little over a week after the February 2019 meeting with industry, the CDC closed its investigation. In its second and last public notice about the outbreak, it said 129 people had gotten sick, 25 had been hospitalized and one person had died. There was no mention of Perdue or any other company.
In ending the investigation, the CDC seemed to send mixed messages. While the agency noted that “illnesses could continue because this salmonella strain appears to be widespread in the chicken industry,” it also told Consumer Reports that the decision was prompted by a decrease in new cases.
Infantis Strikes Another Victim
Five months after the CDC closed the infantis investigation, Arthur Sutton and Marva Lamping walked into El Rodeo, a lively Mexican restaurant in Bend, Oregon, where copper art hangs on rustic yellow walls and red-clay mosaics line the archways.
The couple typically went there at least once a month after paying their mortgage or when friends were in town. Sutton’s stomach had been bothering him since eating there the week before, but he didn’t know why. He decided he was up for going out anyway. It was his 70th birthday, and the couple always went to El Rodeo for their birthdays.
Lamping and Sutton had met 15 years earlier at the local community college when Sutton decided to put his past struggles with addiction to constructive use by becoming a counselor. After math class, a group of students would go out to a Mexican restaurant.
“He just one day said, ‘I noticed when we go out for nachos, that you don’t have a margarita with all the other ladies,’” Lamping said. “And I said, ‘No, I don’t drink and drive.’ And he said: ‘Well, I’ll give you a ride. If you’d like a margarita, I’ll take you.’”
Lamping, 63, was drawn to Sutton’s warm and accepting way of engaging with the world — a demeanor that seemed perfectly suited for his counseling work. Lamping said his clients clearly had a bond with him. Once, while he and Lamping were stuck in construction traffic, a former client working as a flagger recognized Sutton and came over to shake his hand.
Sutton, a large man with a square chin, broad forehead and glasses, was quieter than usual that night as a waiter brought out tortilla chips, salsa and a small oval dish of chopped cabbage slaw mixed with diced jalapenos, tomatoes and cilantro. Lamping went to play a few rounds of video slots in the back of the restaurant before dinner while Sutton dug into the salsa and slaw.
Those appetizers would take on grave importance for Lamping after Sutton developed severe food poisoning that night. She said that during its investigation of Sutton’s illness, the county Health Department would ask her if Sutton had eaten salsa and slaw, which an investigator later described in an internal email as the “likely culprit” behind multiple food poisoning cases connected to the restaurant.
El Rodeo’s owner, Rodolfo Arias, said he “didn’t know anything” about the investigation.
An inspection of the restaurant would find concerns with cross-contamination because El Rodeo thawed and washed frozen chicken in the same three-compartment sink in which it washed lettuce, tomatoes and cilantro. Inspectors also noted the faucet was “uncleanable” because it was wrapped in black tape.
Arias denied that his restaurant was responsible for Sutton’s illness. “I don’t think it was possible,” Arias said.
After dinner, the ache in Sutton’s stomach erupted. He began vomiting and couldn’t lay down to sleep. By the next morning, he could no longer stand the pain. He called Lamping at work, where she handles patient admissions at St. Charles Medical Center. She went home and took him to the emergency room, several hundred feet from her desk.
After a CT scan, a doctor diagnosed Sutton, who was obese and had other medical problems, with a hernia. He was discharged with plans for surgery.
But the pain didn’t go away. Ongoing diarrhea sent him to the toilet every 10 minutes. He tried to hide his pain, but Lamping finally convinced him to return to the hospital. “I’m looking into your eyes right now, Arthur,” she remembers telling him. “You’re dying.”
Sutton’s hospital stay, detailed in 2,000 pages of medical records provided by Lamping, would be marked by one wrenching episode after another. In the emergency room, when a nurse put a feeding tube up his nose, blood started gushing out.
Still, Sutton maintained his signature equanimity. Medical staff described him in notes as “very relaxed and accepting and taking it all in stride.”
Initially, the intensive care doctors thought Sutton was still struggling with the effects of a complex hernia. But in the operating room, it became clear that things were worse than doctors imagined. His bowels were severely damaged. Surgeons set about removing dead segments of his intestines and reconnecting the functioning parts. They also noted that Sutton had an acute kidney injury caused by “profound” dehydration and septic shock from a widespread infection.
Over 16 days, Sutton underwent a similar procedure seven more times. Surgeons cut out pieces of dead intestine, centimeter by centimeter, and tried to repair tears and leaks in his bowels. Sutton was going in for surgery so often they placed a medical dressing over his abdomen so they wouldn’t have to cut him open every time.
Throughout, Sutton cycled through periods of decline followed by flashes of normalcy. Sleep-deprived, he began hallucinating that there were monkeys in trees and sailboats emerging from the ceiling. But he was also able to sit in a hallway chair in the sun with Lamping, eat a popsicle and jokingly tell the physical therapist, “You look like Tom Cruise.”
Still, Sutton was deteriorating. One day, Lamping found a note on the bedside table that Sutton had scratched out: “Why is this happening?”
Sutton’s doctors were also puzzled. After the first surgery, they’d quickly identified salmonella as the source of Sutton’s illness and immediately started antibiotics. But after nearly a week, they couldn’t understand why there was no improvement.
What Sutton’s doctors didn’t yet know was that a pernicious type of bacteria was poisoning Sutton’s blood: the strain of multidrug-resistant infantis circulating throughout the chicken industry.
To Industry, the Mystery of Infantis “Went Away”
A month before Sutton got sick, the CDC’s top foodborne disease experts held another meeting with the National Chicken Council. This time Perdue and four other big chicken processors were at the table.
Internal agency notes drafted before the meeting showed officials bracing for an unreceptive audience. “They have known about our concerns for years,” the notes read. “They know about European practices. As a member-run trade association, their position is often driven by the lowest common denominator. Business margins are ‘razor’ thin; some companies are unable or unwilling to embrace expensive control strategies upstream.”
During the three-hour meeting, the group discussed salmonella prevention and lessons learned from infantis.
But the CDC’s message — that infantis was a serious problem that demanded action — doesn’t seem to have resonated with Ashley Peterson, the industry representative who organized and attended the meeting. In September 2019, Peterson, the National Chicken Council’s senior vice president of scientific and regulatory affairs, told trade magazine Poultry Health Today that infantis wasn’t a problem anymore, according to avideoof the interview.
“We don’t really understand where it came from or why it went away,” Peterson said.
Learning of Peterson’s comments, Tauxe of the CDC seemed surprised and puzzled.
“It didn’t go away,” he said. “We have met with the NCC repeatedly and have emphasized with them that it’s an ongoing problem. That’s wishful thinking of some kind.”
National Chicken Council spokesperson Tom Super said Peterson was referring to the CDC investigation ending and only learned later that the CDC was still seeing cases of infantis. He added that the industry has invested tens of millions of dollars a year in food safety and it has never downplayed infantis.
More than two years after Peterson’s comments — as infantis has sickened thousands more people — the trade group still hasn’t answered most of the CDC’s questions about the strain and has shared little with the agency about efforts to curb it, Tauxe said.
“How it got into the chickens in the first place, and why it expanded across the country through the chickens and why it’s persisting remain open questions for us,” he said. “Stopping it is going to depend on what the industry is willing to step up to and do.”
Super denied that the industry hadn’t answered the CDC’s questions but didn’t provide responses when ProPublica posed them again. “The industry never stopped working to address salmonella infantis — an effort that continues today,” he said.
Swifter action might have made the difference for Sutton.
At the hospital in Oregon, Sutton’s prognosis worsened. By mid-August 2019, the doctors had learned that the type of salmonella ravaging Sutton’s body was infantis. The finding might have helped doctors change course, but it was too late. The bacteria had already taken its toll.
Back in his room after a half-dozen surgeries, Sutton signaled to Lamping, waving two hands to show that he was done. “He just kept going: ‘Enough, enough. No more,’” Lamping said.
She looked at Sutton and shook her head, refusing to give up. But there wasn’t much the doctors could do.
During his eighth visit to the operating room, a surgeon noted that the leak in his bowels was probably so deep that it wasn’t accessible to surgeons: “Any further dissection would be significantly risking more bowel injury and making his current problem worse,” the medical records said.
More than two weeks into his hospital stay, Sutton’s salmonella infection had led to kidney failure. Sutton would need round-the-clock dialysis and a feeding tube to survive.
Lamping and Sutton’s brother, Jim, gathered in Sutton’s room to decide what to do. They agreed that Sutton wouldn’t want to live constantly hooked up to machines.
They told the hospital to stop treatment and move him to comfort care. “Time for him to go to heaven,” Jim Sutton said. After life support was removed, Lamping sat next to the bed and rested her head on Arthur’s hand.
The next day, on Aug. 16, 2019, Arthur Sutton died. The cause was severe blood poisoning and acute organ dysfunction brought on by salmonella. Lamping was paralyzed by grief. Her visions of the future had always included him.
“I watched a man go from happy-go-lucky — someone who should have been with me another 20 years — I lost him,” Lamping said. “I Iost him.”
Two years later, she still replays Sutton’s battle with salmonella over in her mind, certain that something could have been done differently.
Lamping has focused on potential problems with how their food was handled at El Rodeo and hired a lawyer to file a lawsuit against the restaurant in 2020. She blames the restaurant, in part, because a county health inspection after Sutton died noted that it had told El Rodeo about the “findings from the state health lab on salmonella infantis cases.” In court filings, the restaurant denied the allegations.
But Lamping also says there are things that food safety regulators and the industry could have done long before the chicken arrived at El Rodeo.
“If they know that infantis is in the chicken, if they know it’s there, why are they selling it to us?” Lamping asked.
The USDA, to this day, has never said anything to consumers about the risk of multidrug-resistant infantis.
Because of the pandemic, Lamping and Jim Sutton have had to delay Arthur’s memorial. They hope that someday soon, they’ll be able to gather his friends and family on a hill overlooking a canyon in central Oregon.
They’ll walk through shale rock, wildflowers and junipers, and look over the canyon’s edge where a buck can sometimes be seen running through the sagebrush. They’ll open Sutton’s urn and let the wind carry his ashes away.
About the Data: How ProPublica Analyzed Bacterial Pathogen Presence
ProPublica obtained bacterial pathogen genomic sequencing data from the National Center for Biotechnology Information’sPathogen Detectionproject. The project integrates data from bacterial pathogens sampled from food, the environment and human patients by participating public health agencies in the United States and around the world. The NCBIanalyzesdata as it is submitted, and the results are monitored by public health agencies, including the CDC as part of foodborne illness outbreak investigations. The data includes metadata about each bacterial isolate submitted by the person or institute who collected the bacterial sample, as well as computational predictions by NCBI.
Through Freedom of Information Act requests, ProPublica obtained epidemiological information about bacterial samples taken as part of the2018-19 salmonella infantis outbreakinvestigation and samples obtained during routine testing in establishments regulated by the USDA’s Food Safety and Inspection Service. ProPublica also obtained epidemiological information connected to patients considered part of this outbreak, including the date of sample collection and details about a patient’s illness, recent food consumption and demographics — details crucial to foodborne illness investigations. Data about bacteria found during USDA inspections also included the type of meat or poultry the sample was obtained from, the date of collection and the name and location of the facility. Integrating these details with the NCBI metadata offered a way to group samples together not just by genetic similarity, but also by location and time.
The USDA postspublic datasetscontaining the results of its salmonella sampling at poultry processing plants since 2015, which detail the collection date, type of poultry product sampled and, if salmonella was present, information on type and any antimicrobial resistance. The datasets include both routine sampling, conducted at every plant, and follow-up sampling, conducted at plants where the agency has identified high levels of salmonella. (Samples from USDA inspections that contain salmonella are reflected in both the NCBI data and the agency’s inspection data.)
Analysis Decisions
To confirm the persistence of multidrug-resistant infantis in food processing facilities, grocery stores and patients with salmonella infections, ProPublica relied on both metadata submitted to NCBI and genetic features computed by NCBI. ProPublica restricted its analysis to isolates in the NCBI data belonging to what was known as SNP cluster PDS000089910.78, as of Oct. 19, 2021. This cluster contains most isolates involved in the infantis outbreak, and the CDC said it is monitoring most of the isolates in the cluster. ProPublica also filtered for isolates that were reported to be serotype infantis by the submitter or, when user-submitted information was unavailable, were computationally predicted to be infantis by the NCBI data processing pipeline.
ProPublica used data about evolutionary modeling computed by NCBI to establish the degree of genetic similarity between bacterial isolates from the outbreak and isolates collected more recently.
ProPublica’s analysis of salmonella rates in poultry plants is based on methods the USDA uses, using the agency’s routine sampling data to calculate positivity rates — that is, the number of positive tests compared with all salmonella tests taken at the facility — for each type of poultry a plant processed. ProPublica also calculated the high-risk salmonella rate for plants, determining the percentage of samples at the facility that tested positive for one of the 30 salmonella types theCDC has foundto be most associated with human illnesses.
The USDA inspection data was also used to compare the number of samples found to contain salmonella infantis and salmonella Kentucky with the total number of routine samples taken each year to determine the rate at which each was occurring in the sampling program across all plants and poultry types.
In a statement, the ministry said the two Christchurch cases were expected and linked community cases, both from a single household linked to the cases identified earlier this week.
The ministry said 13 close contacts of the four Canterbury cases were isolating and will undergo further testing.
There was also one new case in Northland and four in Waikato, with the remaining 118 in Auckland.
Three of the Waikato cases are still to be linked, but the Northland case was not unexpected, as they were a household member of a case and were already isolating.
Fifty-one of the new cases are still to be linked. There have been 289 unlinked cases in the past 14 days.
Three new border cases
There were also three new cases and one historical case identified at the border.
There are 39 people in hospital with the coronavirus, including four in intensive care.
The ministry said the rise in case numbers was a reminder of the infectiousness of covid-19.
“With over 30,000 tests processed nationwide yesterday, these results aren’t unexpected,” it said.
There were 44,779 doses of the covid-19 vaccine given yesterday, including 12,780 first doses and 31,999 second doses.
One of the four new cases reported in the Waikato today has been linked to existing cases. Three of the new cases were in the Te Awamutu/Kihikihi area and one in Ōtorohanga.
The number of community cases linked to the current outbreak has risen to more than 3000, with 3046 cases in this outbreak — more than half of the 5764 in total since the pandemic began.
This article is republished under a community partnership agreement with RNZ.
This content originally appeared on Asia Pacific Report and was authored by APR editor.
The New Zealand government revealed changes to MIQ (managed isolation and quarantine) today, with stays halving from 14 to seven days, followed by isolation at home for three days.
Covid-19 Response Minister Chris Hipkins and Director-General of Health Dr Ashley Bloomfield gave today’s update on the government’s response to the Delta outbreak.
Under the new MIQ regime, which will begin from November 14, arrivals must be fully vaccinated and will be tested on days 0, 3 and 6 and undertake a rapid antigen test before leaving MIQ, before a day-9 test at home.
He said this would free up about 1500 rooms a month in MIQ. Some of this would be taken up by community cases but some would go into the booking system for travellers from overseas.
Pacific border travel
The second step will be to reopen the border to low-risk travellers from Samoa, Tonga and Tokelau without isolation.
This one-way quarantine-free travel will begin from November 8.
The third step will allow more people to isolate at home, available to increasing numbers of travellers in the first quarter of 2022.
He said changes at the border will be linked to the traffic light system.
“The faster New Zealanders get fully vaccinated so that we can move to the traffic light system, the faster we’ll be able to open the border.”
He said New Zealanders will also understand that the government does not want to accelerate the spread of covid-19 around the country by lowering restrictions before we reach very high levels of vaccination.
Kiwis first priority
Hipkins said the first priority for allowing people into New Zealand was Kiwis and people who already had visas, followed by other groups like international students.
“Tourists are more of a challenge … what you will see though in the first part of next year will be quite different from the way we’ve been managing it over the past 18 months.”
Hipkins said stopping covid-19 at the border had been a priority and New Zealand’s ability to do so had led to levels of freedom over the past year and a half which were the envy of many other nations.
“As a country we owe a massive vote of thanks to our front-line MIQ and border workers,” he said.
Hipkins said in the meantime, the message to all New Zealanders was very simple – get vaccinated.
Indonesia’s popular tourism islands of Bali opened for tourism last week, while Thailand announced that from November 1 vaccinated travellers from 19 countries will be allowed to visit the kingdom including its tourism island of Phuket.
Both those countries’ tourism industry, which is a major revenue earner, has been devastated by more than 18 months of inactivity that have impacted on the livelihood of hundreds of thousands of people.
India and Vietnam also announced plans to open the country to vaccinated foreign tourists in November, and Australia will be opening its borders for foreign travel from mid-November for the first time since March 2020.
Countries in the Asia-Pacific region — except for China — are now beginning to grapple with balancing the damage to their economies from covid-19 pandemic by beginning to treat the virus as another flu.
The media may have to play a less adversarial role if this gamble is going to succeed.
October 11 was “Freedom Day” for Australia’s most populous city Sydney when it came out of almost four months of a tough lockdown.
Ironically this is happening while the daily covid-19 infection rates are higher than the figure that triggered the lockdowns in June.
‘It’s not going away’
Yet, New South Wales Premier Dominic Perrottet told Sky News on October 11: “we’ve got to live alongside the virus, it’s not going away, the best thing that we can do is protect our people (by better health services)”.
He added, “each time we tighten up, businesses are further disrupted, workers lose jobs, children are deprived of a proper childhood and school life”.
Singapore is coming out of lockdown when it is facing the highest rates of daily infections since the covid-19 outbreak.
Both Singapore and Australia adopted a “zero-covid” policy when the first wave of the pandemic hit, quickly closing the borders, and going into lockdown.
Both were exceptionally successful in controlling the virus and lifting the lockdowns late last year with almost zero covid-19 cases. But, when the more contagious delta virus hit both countries, fear came back forcing them back into lockdowns.
However, PM Lee told Singaporeans that lockdowns had “caused psychological and emotional strain, and mental fatigue for Singaporeans and for everyone else. Therefore, we concluded a few months ago that a “Zero covid” strategy was no longer feasible”.
‘Living with covid-19’
Thus, Singapore has changed its policy to “Living with covid-19”.
In a Facebook posting on October 10, Australian Prime Minister Scott Morrison said: “The phenomenal response from Australians to go and get vaccinated as we’ve seen those vaccination rates rise right across the country, means it’s now time that Australians are able to reclaim their lives. We’re beating covid, and we’re taking our lives back.”
On October 8, Australia’s Federal Health Minister Greg Hunt said that though infection rates might still be a bit high, yet less than 1 percent of those infected were in intensive care units (ICUs).
Why didn’t political leaders take this attitude right from the beginning and continue with it? After all the fatality rate of covid-19 has not been that much higher than the seasonal flu in most countries.
True, it was perhaps more contagious according to medical opinion, but fatality rates were not that large in percentage figures.
According to the Worldometer of health statistics, there have been 237.5 million covid-19 infections up to October this year and 214.6 million have recovered fully (90.4 percent) while 4.8 million have died (just over 2 percent).
According to the US Center for Disease Control and Prevention (CDC) estimates, there have been between 39-56 million flu cases, about 700,000 flu hospitalisations recorded in the US during the 2019-2020 flu season up to April 2020.
They also estimate between 24,000 to 62,000 flu deaths during the season. But did the media give these figures on a daily or even a weekly basis?
New global influenza strategy
In March 2019, WHO launched a new global influenza strategy pointing out that each year there is an estimated 1 billion flu cases of which 3-5 million are severe cases, resulting in 290,000 to 650,000 influenza-related respiratory deaths.
This has been happening for many years, but, yet the global media did not create the panic scenario that accompanied covid-19.
Unfortunately, the media’s adversarial reporting culture has helped to create a fear psychosis from the very beginning of the outbreak in early 2020, which may have contributed to millions of deaths by creating anxiety among those diagnosed with covid-19.
During the peak of the delta pandemic in India, many patients died from heart attacks triggered by anxiety. Would they have died if covid-19 were treated as another flu?
In the US out of the 44 million infected with covid-19 only 1.6 percent died. In Brazil from 21.5 million infected, 2.8 percent of them died, while in India out of 34 million infected only 1.3 percent died.
But what did we see in media reports? Piles of dead bodies being burnt in India, from Brazil bodies buried in mass graves by health workers wrapped in safety gear and in the US, people being rushed into ICUs.
They are just a small fraction of those infected.
Bleak picture of sensationalism
I was the co-editor of a book just released by a British publisher that looked at how the media across the world reported the covid-19 outbreak during 2020. It paints a bleak picture of sensationalism and adversarial reporting blended with racism and politicisation.
It all started with the outbreak in Wuhan in January 2020 when the global media transmitted unverified video clips of people dropping dead in the streets and dead bodies lying in pavements. Along with the focus on “unhygienic” wet markets in China this helped to project an image of China as a threat to the world.
It contributed to the fear psychosis that was built up by the media tinged with racism and politicisation.
If we are to live with covid and other flu viruses, greater investments need to be made in public health.
In Australia, health experts are talking about boosting hospital bed and ICU capacities to deal with the new policy of living with covid, and they have also warned of a shortage of health professionals, especially to staff ICUs.
What about if the media focus on these as national security priorities? Rather than giving daily death rates and sensational stories of people dying from covid — do we give daily death rates from heart attacks or suicide?
We should start discussing more about how to create sustainable safe communities as we recover from the pandemic, and that includes better investments in public health.
We need a journalism culture that is less adversarial and more tuned into promoting cooperation and community harmony.
Kalinga Seneviratne is co-editor of COVID-19, Racism and Politicization: Media in the Midst of a Pandemic published in August 2021 by Cambridge Scholars Publishers. IDN is the flagship agency of the Non-profit International Press Syndicate. This article is republished in partnership with IDN.
National Capital District Governor Powes Parkop has announced that there will not be a total lockdown of Port Moresby.
He said the decision was made after much deliberation with key stakeholders in the city and the national government.
“Instead we will focus on maintaining and upgrading the three-pronged approach we are currently pursuing to respond to the third wave of the covid-19 pandemic,” Parkop said.
NCD Governor Powes Parkop … “we will focus on maintaining and upgrading the three-pronged approach we are currently pursuing to respond to the third wave of the covid-19 pandemic.” Image: EMTV News
NCD Metropolitan Superintendent Gideon Ikumu said it would also be a logistical nightmare for police to arrest people who breached the covid protocols because they did not have the facilities to lock up all those people.
He said city police would only encourage city residents to observe the new normal protocols of wearing facemasks, observing social distancing and other measures as part of their policing routines in the city.
Superintendent Ikumu said this as the City Hall announced on Monday that it would not enforce a complete lockdown as many people had expected, despite the rocketing number of deaths and covid-19 positive cases in the city since September.
“There is an absence of regulations to implement the specifics of the Pandemic Act 2020 and we cannot arrest someone for simply not wearing a mask as an example,” he said.
Defining legislation
A regulation is the subsidiary legislation that defines the essence of an Act.
It also provides guidelines that show the way the Act needs to be implemented.
Superintendent Ikumu reiterated Governor Parkop’s appeal to city residents that to stop unnecessary deaths and to get “us to overcome the crisis at hand, it needs everyone to step up and do their part”.
“For those who are still reluctant or afraid of the vaccine for one reason or another, the “Nupla Pasin protocols and testing must be your foremost priority on a daily basis,” he said.
“We will do our best to encourage compliance but it is up to each and every person in the city to comply.”
 (@alexwapa)
(@alexwapa)