New Zealand Prime Minister Jacinda Ardern today announced vaccination will be mandated in any workplace that requires a certificate of vaccination for entry.
Last week the government announced details of its Covid-19 Protection Framework last week, involving the roll-out of a “traffic-light” system once all district health boards (DHBs) hit 90 percent full vaccination rates.
Ardern told media the government wanted everyone to move towards the new system announced and urged vaccination rates to increase.
She said this was the “best way to give certainty to business and to our communities”.
“We need to ensure vaccination rates lift. So please don’t wait until cases come to your town or your city, get vaccinated now,” she added.
Under the new traffic light system, hospitality, hair dresses and gyms can operate at all levels if they ask customers for vaccine certificates.
The government had already mandated vaccinations for people working at the border, and in the health and education sectors.
“If customers must be vaccinated, then so too, must the workers,” she said.
“The timing of this coming into force will depend on when we move to the Covid-19 Protection Framework.”
Watch the media briefing
Today’s media conference. Video: RNZ News
Ardern said the requirement would ensure staff and customers were treated equally, and it would play a “big part in helping to minimise the spread of the virus in the highest risk venues by reducing the potential for covid to enter the business”.
The prime minister rejected suggestions the new requirement constituted government overreach and said the move had a public health basis, which balanced the rights of workers with the rights of business clients.
Minister for Workplace Relations and Safety Michael Wood said the current orders in place covered 15 percent of the workforce.
“Our estimate is that those workplaces covered by covid vaccine certificates are potentially around about 25 percent of the workforce,” he said.
“So, that would bring it to about 40 percent in total, noting that other workplaces would still have access to the simplified risk management framework.”
New Zealand has reported 79 new community cases of covid-19 today.
Of the new cases, 75 are in Auckland and four are in Waikato. Forty six of these cases are linked, including 24 household contacts, and 33 remain unlinked.
The Vanuatu covid task force has confirmed that two arrivals from New Caleldonia have covid-19.
But the organisation says Vanuatu remains free of any community transmission of the virus.
Health officials are endeavouring to trace contacts from the airport to the Ramada Hotel where the two positive ni-Vanuatu nationals are now currently being quarantined.
They were part of a group of 18 ni-Vanuatu who were repatriated from New Caledonia last Friday.
Of the 18, eight had already contracted the virus in New Caledonia, but had been treated and the task force says are no longer presenting any symptoms.
All 18 remain in isolation at the Ramada Hotel in Port Vila.
Prime Minister Bob Loughman has called on the people to get vaccinated to protect themselves and their families.
He also asked people not to disseminate incorrect information through social media, because of the panic it would cause within Vanuatu communities.
This article is republished under a community partnership agreement with RNZ.
This content originally appeared on Asia Pacific Report and was authored by APR editor.
There are now 287 unlinked cases from the past 14 days.
There are 50 people in hospital, including four people in intensive care. The ministry said the average age of those in hospital is 44.
Yesterday the Ministry of Health reported 104 community cases of covid-19 — the second highest number in the current delta variant outbreak.
The two new cases in Waikato — one in Te Awamutu and one in Hamilton — remain unlinked, along with five other cases in the region.
Waikato region testing
The ministry said the Waikato District Health Board (DHB) was continuing to carry out testing throughout the region to help determine any undetected community spread of covid-19.
“We are urging anyone in Waikato — in particular, people in Te Awamutu — to get tested if they have any symptoms that could be covid-19.”
One of yesterday’s cases was in Blenheim. The person tested positive after arriving on a flight from Rotorua via Wellington.
This is the first community case of covid-19 in the South Island in a year.
The ministry said today that the covid-19 positive case in Blenheim was unvaccinated, but that two household contacts had returned negative results.
The ministry is still asking residents in Marlborough, Nelson and Tasman with symptoms — no matter how mild — to get tested, even if they are vaccinated.
“This individual was tested as a close contact of the previous cases confirmed yesterday.”
Triple figures for three days
Until today the number of community covid-19 cases reported has been in triple figures for three days running, with 129 cases reported on Friday and 102 cases on Thursday.
There have now been 2572 cases in the current outbreak, and 5278 since the pandemic began.
There were 42,482 vaccinations given yesterday — 11,777 first doses and 30,705 second doses.
“It remains our number one protection against covid-19,” said the ministry.
“The Pfizer vaccine is safe, will help stop you getting seriously ill, and could save your life.”
The next media conference will be held on Tuesday.
This article is republished under a community partnership agreement with RNZ.
With most of its eligible adult population covered, Fiji’s covid-19 vaccine rollout for teenagers is gaining pace.
The Health Ministry said 28,965 children aged 15 to 17 had received a first vaccine dose — and 3892 teenagers had received a second.
The rollout was recently extended to this age bracket after vaccination rates covered almost all of Fiji’s eligible adult population aged 18 and over — 95.9 percent of them have received their first vaccine dose, and 84.4 percent have had a second.
Papua New Guinea’s biggest referral hospital has reached a crisis point as the covid-19 pandemic positivity rate surged drastically to 85 percent yesterday.
Port Moresby General Hospital chief executive officer Dr Paki Molumi in the National Capital District (NCD) has revealed that three children with covid-19 had died three days ago.
He also said yesterday that the hospital had recorded the highest deaths on arrival — 50 on Monday, 40 on Tuesday and 30 on Wednesday.
This was a sign that the hospital was reaching a crisis point with services teetering on collapse unless they are immediately given more support.
“PMGH now we have reached a crisis point. The first surge we were able to manage, the second surge we were able to manage but this third surge which is the delta variant is very aggressive, and we are reaching a very critical term,” he said.
“Aggressive means in the first surge we saw a lot of older people getting infected, and so with the second surge.
“This one, we are getting very young people — we lost three kids three days ago. This surge is not discriminating with anyone, its affecting everybody.”
Another dilemma
The hospital is also faced with another dilemma — this time over dead bodies that urgently require money and paper work to be completed to pave the way for their burial.
The deceased include a staggering 300-plus dead bodies with many of them covid-19 related cases and the hospital does not know where it will put the new bodies that are coming out from its covid-19 wards.
Dr Molumi also said 94 of their medical staff were infected with the virus, 52 medical and 42 nursing staff of the hospital had been infected by the virus. They must be given days off for home isolation, further reducing manpower.
“We are faced with a crisis where cobvid patients are presenting in large numbers with shortness of breath requiring manpower to assist,” he said.
“The few staff left are overworked and fatigued and we need to recruit more staff urgently.
“Our staff are facing unprecedented mental health challenges, as we witness death tolls never seen in the history of our hospital.”
“Our AusMat triage tent in front of the PMGH is full, emergency department is full, the isolation ward is full, the covid ward is full and all other beds in different sections, including the maternity wing allocated to covid are also full with covid-19 patients.
‘Dying before reaching hospital’
“People are dying without reaching the hospital. Our mortuary recorded 50 deaths on admission on Monday, 40 deaths on admission on Tuesday and 30 deaths on admission today, with more expected tonight.
“We have never recorded such a high number of deaths on admission.
“The morgue is filled, with bodies packed on top of one another. Right now, 300 plus bodies are at the morgue.
“Three more refrigerated containers have been installed to store dead bodies, but this is not enough. Some bodies were left outside for days because we just don’t have space in the morgue.
“A mass burial of 200 bodies is being planned this week to create more space. The bodies are both covid positive and unclaimed non-covid,” he said.
“So we as the city’s hospital serving over a million population in the national capital district, Central Province as well as parts of Gulf — we are reaching a crisis point.
Matt Cannon, chief executive of St John Ambulance, also said the service was in crisis.
“I think it’s fair to say that the ambulance service at this stage is in a crisis level,” he said.
“Challenges they need to cater for increasing number of patients… our ambulance service is also seeing a stretch!”
Gorethy Kennethis a senior PNG Post-Courier journalist.
Nine of today’s new cases are in Waikato, with the rest in Auckland.
Auckland remains at step 1 of alert level 3, and this will be reviewed on November 1, while parts of Waikato are also at alert level 3, to be reviewed on October 27.
“The delta variant has made it very hard for New Zealand to maintain its elimination strategy — and now we need people to be vaccinated to save lives,” reports the Ministry of Pacific Peoples.
“If you’re still weighing up whether to get vaccinated, check out our Let’s Talanoa video series.”
Open conversations
Aimed at Pacific people under 30, this video series promotes having open conversations about the covid-19 vaccine and why it is safe and important to get vaccinated.
The series is hosted by Dr Lesina Nakhid-Schuster and Rocky Lavea.
This week’s episode is “Know your Vax”, which you can view on our digital channels Facebook, Instagram and YouTube.
Visit here for a list of walk-in and drive-through vaccination locations.
Based on the advice of Professor David Skegg and the Public Health Advisory group, New Zealand’s goal is to minimise and protect.
Like the current alert level system, there will be three settings — green, orange and red — and it is designed to manage outbreaks and cases.
The New Zealand government has announced details of its Covid-19 Protection Framework, involving the roll-out of a “traffic-light” system once all district health boards hit 90 percent full vaccination rates.
A vaccine certificate will be central to the new framework.
The system will involve three settings – green, orange and red.
“If you want to be guaranteed that no matter the setting that we are in, that you can go to bars, restaurants and close-proximity businesses like a hairdresser, then you will need to be vaccinated,” Prime Minister Jacinda Ardern told media today.
She was accompanied by Deputy Prime Minister Grant Robertson, Covid-19 Response Minister Chris Hipkins and Associate Health Minister Peeni Henare as the government also announced enhanced:
financial support for businesses and those families struggling under restrictions, and
a new $120 million fund to boost Māori vaccination rates and protection of communities.
Ardern said the vaccination certificates would allow businesses to be able to open and operate at any level.
Associate Health Minister Peeni Henare outlines the $120 million plan today to boost Māori vaccinations as part of the new national covid-19 protection framework. Image: TVNZ screenshot APR
Targeted local lockdowns
If cases start to climb in areas with lower vaccination rates in lower-income communities, much more highly targeted and localised lockdowns could be used if needed, she said.
The red setting would allow hospitality to open with vaccine certificates, but gathering limits and physical distancing, masks and other public health measures would be used.
“This will still feel like a huge amount of freedom relative to what Auckland has now,” Ardern said.
Auckland will move into red as soon as the Auckland district health boards (DHBs) hit the 90 percent vaccination target, rather than wait for the rest of the country.
The rest of the country will move all at the same time to “orange” when all DHBs around the country reach the 90 percent target.
At orange, gathering limits can lift. Places that choose not to use vaccination certificates will either be closed or have public health measures in place.
Green is when there are some covid-19 cases in the community but at low levels. Fully vaccinated people can enjoy all events and hospitality and gatherings by showing a vaccine certificate.
Premises choosing not to use certificates will face restrictions similar to the current alert level framework.
New tools system
Ardern said the reason for changing from the current alert level system was because the country needed a system that made use of the new tool of vaccines and vaccine certificates.
“On 29 November, Cabinet will review the progress that Auckland has made and the rest of the country to see if anything needs to change. We are open to moving the South Island before the rest of the country if all DHBs in the south hit their targets before others,” she said.
Ardern emphasised covid-19 cases in the community would rise.
“But because we won’t take this step until we are at 90 percent vaccination, we will also have higher levels of protection that limit covid’s impact,” she added.
The PM said that if any member of the public was not vaccinated, there would be things they would miss out on and people who wanted to get out and enjoy summer should do so.
Detail would be progressively added to the system as time went on. The country would move all at the same time to “orange” when all DHBs around the country reached the 90 percent target.
Ardern said the focus on elimination had kept New Zealand free from covid-19 for much of the past 18 months when the population was vulnerable.
World-leading response
“We can rightfully be proud of what our world-leading response has achieved, but two things have changed since then,” she said.
“The first is that delta has made it very hard to maintain our elimination strategy … but as our long-standing strategy was challenged we also had a new tool.
“That tool is the vaccine. The vaccine we are using in New Zealand is safe and effective … it also helps protect everyone. The more people who are vaccinated, the harder it is for covid to spread through communities quickly.
“Protection means that we won’t just treat covid like a seasonal illness, we will protect people from it with vaccination, management, and a response that focuses on minimising the health impacts.”
Financial support An enhanced business support package was also unveiled. It included a significantly boosted Covid-19 Resurgence Support Payment.
It will rise from $1500 per eligible business and $400 for each full-time employee (50FTEs maximum), to $3000 per eligible business and $800 per FTE. This will apply from 12 November.
The enhanced support will be paid fortnightly until Auckland has been able to move into the new protection framework.
The wage subsidy will continue to be available on the current criteria while areas of the country are still in alert level 3.
A $60 million fund for business advice and mental health support in Auckland was also announced. Businesses will be able to apply for up to $3000 for advice and planning support, and up to $4000 to implement that advice.
There will also be support for low-income households.
From 1 November income limits for assistance will rise to 40 hours at the minimum wage, or $800 per week and $1600 per week for a couple with or without children.
Finance Minister Grant Robertson told media the approach New Zealand had taken had, along with sustaining one of the lowest mortality rates in the world, also led to strong economic growth, low unemployment and one of the lowest levels of government debt in the world.
But said he was acutely aware of the impact of restrictions on businesses.
“To date we have paid out about $4.8 billion in support … that exceeds the new operating spending we would have for the whole year for the whole country in most Budgets.”
This article is republished under a community partnership agreement with RNZ.
Pacific leaders say offering “visas for vaccinations’ would be the ultimate incentive for New Zealand overstayers to get the covid-19 jab, as Auckland struggles to stop delta variant infections spreading through the community.
It comes as epidemiologists say the government needs to pull out all the stops to get people vaccinated amid rising case numbers.
The Ministry of Health reported a record 102 community cases today, the first time the number of new cases has reached triple figures.
Director-General of Health Dr Ashley Bloomfield said on the current trajectory there could be up to 180 cases a day within two to three weeks. The number of these cases that ended up in hospital would depend on how many had been vaccinated, he said.
The latest modelling showed there was not a large amount of undetected cases, and the numbers being found were what would be expected, he said.
Plea for an overstayer amnesty
The Pacific Leadership Forum is calling for an overstayer amnesty through a parliamentary petition, which won support from the Employers and Manufacturers Association.
The forum’s Pacific Response Coordination Team chair Pakilau Manase Lua said that adding in an immigration incentive to that amnesty would be very effective.
“I would guarantee that probably 99.9 per cent of overstayers would come out of the woodwork and get vaccinated if that was their pathway to residency or amnesty to get their papers to be legal here,” Lua said.
“They’re desperate. It was hard enough before covid arrived for these people to survive – they have to work, they have to find a way to make ends meet.
“Moving from house to house and at the whim of the family and friends who are sheltering them. And that’s a risk to themselves and to others if they’re not vaccinated”
Among an estimated 14,000 overstayers, the highest numbers without valid visas are from Tonga and Samoa.
A fifth of the current active covid-19 cases are among Pacific people, and their fully vaccinated rates are lower (at 59 percent) than the national average (67 percent).
‘They fear authority’
If the government was concerned an amnesty would be unpopular, it needed to make sure politics did not trump public health, said Lua.
“The optics don’t matter, it’s life or death – in a pandemic, what are optics compared to human lives? We’ve got a virus raging in South Auckland among our communities where most overstayers are living.
“And despite all the reassurances to go out and test and to get vaccinated, we know that many have yet to be vaccinated – some have gone in, but the majority have not.
“Rightfully, they fear authority – these are people who are hiding from authority because they’ve got deportation orders or other things that are hanging over them.”
Tongan Manase Lua, an overstayer as a child during the Dawn Raids era before an amnesty gave his family a permanent future, said launching a similar reprieve now would also recognise the reality that no-one could be deported back to the Pacific Islands while there was a risk of them spreading covid-19 there.
It was mind-boggling that the government was disregarding the risk, as well the contribution overstayers make, he said.
“They’re resourceful, they work hard, they often do the work that nobody else wants to do on the front lines — while we’re working from home and in the safety and security of home, they’re out on the front lines picking fruit, cleaning the floors, mopping the hospital floors and all the hard work that we take for granted.
“So they would love this opportunity to be a person, be a human being in the country that says it’s kind.”
This article is republished under a community partnership agreement with RNZ.
A Pacific public health expert says a premature transition of covid-19 restrictions in New Zealand could be lethal for Māori and Pasifika communities.
The government is under increasing pressure to ease restrictions in Auckland with National saying it would set a six-week deadline for ending lockdowns and that a target of 85-90 percent vaccination rates were “do-able” within that timeframe.
Prime Minister Jacinda Ardern on Monday revealed the city would remain in alert level 3, step 1, and signalled the government would reveal a covid-19 protection plan on Friday.
But Auckland University public health associate professor Collin Tukuitonga said easing restrictions before vaccination rates among the most at risk communities of Māori and Pasifika were high could be a death sentence.
“It is abundantly clear that Māori and Pasifika people will have more infections, more of them will go to hospital and more of them will die,” he said.
“Fortunately we haven’t had the deaths here that has been apparent in other countries. But clearly if we move prematurely the people at risk will pay the price.”
Hospitals ‘not ready for covid-19 tsunami’
Meanwhile, an Auckland emergency nurse and nursing union delegate told RNZ Morning Report today that overworked nurses feared hospitals were not ready for the “covid-19 tsunami” – and often thought about quitting.
Hospital admissions have climbed to 43, and Middlemore Hospital expects to see 20 cases a day through its emergency department next month.
The nurse, who works in one of Auckland’s emergency departments (ED), said many of her colleagues finish shifts wondering if they would come back for the next one.
“The nurses are really, really feeling it – feeling really anxious. They feel like there’s a tsumani coming. They can see it coming … and what do they do? Do they run towards it or do they back off?”
Her own ED was often short by three or four nurses, or a couple of health care assistants, a shift, she said.
“On a daily basis we are getting texts to say, ‘can you pick up this shift?’. It is becoming a dire situation right now,” she said.
It was made worse because staff regularly needed to isolate because they were case contacts, she said.
The nurse, a delegate for the Nurses’ Organisation, said that if they could not staff the shifts, it made for a high pressure day for those left behind, she said.
This article is republished under a community partnership agreement with RNZ.
There were also two cases reported at the border today.
Authorities also reported that three positive covid-19 cases staying at an Auckland managed isolation facility allegedly escaped last night — and one was still at large.
There were two escapes involving three people who were staying at the Holiday Inn Auckland Airport managed isolation and quarantine (MIQ) facility in Māngere, South Auckland.
Twenty-two of today’s 60 cases are yet to be linked to earlier cases. There are 166 unlinked cases from the past 14 days.
43 people in hospital
There are 43 people in hospital, including five in intensive care.
The number of community cases connected to the current outbreak is now 2158 and there have now been 4854 cases in this country since the pandemic began.
In announcing today’s new covid-19 case numbers, Director-General of Health Dr Ashley Bloomfield said infections were still expected to rise and daily numbers would bounce around.
He continued to encourage New Zealanders to get tested for the virus.
“Of the four new cases today in Waikato, two of those are close household contacts who were already in a quarantine facility and the other two were also known to have likely links to existing cases.”
The total number of cases in Waikato was now 56, 10 of whom have now recovered.
Dr Bloomfield again urged people in Waikato to get tested
“Yesterday, New Lynn’s Shadbolt Park was classified as a location of interest. It’s now been reclassified as an exposure event and has been taken down from the Ministry of Health website.
“Having looked further into the event, which was being managed by a PHU elsewhere in the country it is now being assessed as an exposure event with a small number of people who are contacts.
“They are all known, have all been contacted and are now isolating.”
42,809 vaccine doses given
There were 42,809 vaccine doses given yesterday — 10,392 first doses and 32,417 second doses.
He said health teams in Auckland had moved away from using suburbs of interest as part of their testing regime because the infections are widespread across the city.
Testing instead was going to be focused in areas where there was a higher test-positivity rate, where the risk of unidentified cases is considered potentially higher.
“People with symptoms and even if they are mild symptoms, even if you are vaccinated in New Lynn and the North Shore suburbs of Rosedale, Redvale and Bayswater please do go and get tested as soon as possible,” Dr Bloomfield said.
He said it was important to determine whether there were undetected cases in those communities.
Dr Bloomfield also said from Thursday healthcare employees working into quarantine and isolation facilities would be allowed to work in other healthcare facilities without the need for a 48-hour stand-down period and negative test requirement.
“This will allow greater flexibility in using that MIQ workforce and of others being able to supplement that workforce and reduce some of the real pressure that is under that workforce,” he said.
Third dose for some
He said information was going up on the Health Ministry’s website soon relating to the third dose of the Pzifer vaccine for immuno-compromised people.
It would include the inclusion criteria, including how this small group of people would be identified and when they would receive their third vaccination.
“You will not be able to book a third vaccine on the Book My Vaccine website … details will be up on the website later this afternoon,” he said.
Police said the man had been charged with failing to comply with an order (Covid-19) under the Covid-19 Public Health Response Act and Alert Level 3 Order and is also appearing before the court for breach of bail conditions.
Police have also laid charges against four people in relation to organising and attending mass gatherings in the upper North Island on 16 October.
This article is republished under a community partnership agreement with RNZ.
New Zealand’s Associate Health Minister Peeni Henare today thanked all Māori providers, iwi, hapū, practitioners, vaccinators and district health board (DHB) staff for their efforts, and warned that “covid-19 is on the doorstep of your houses”.
“Do not let it enter,” he added.
“You’re efforts are indeed seen,” he said as he fronted a media briefing today with Prime Minister Jacinda Ardern and Director-General of Health Dr Ashley Bloomfield.
Henare said that over the past two weeks, prior to Super Saturday, he had travelled to a number of DHBs and saw great work but identified a number of challenges.
He asked those who were not on board for their help.
“Our whānau need you and to many of them you are the trusted person that will be key to them making an informed decision about the vaccination,” he said.
Significant funding had already been provided to Hauora Māori to support and build capability for the vaccine programme, he says.
He said that if they needed support to make their decision, get their information from official sources or they could speak to kaumātua and kuia who were currently leading vaccination rates among Māori communities.
An announcement would be made later in the week regarding support for the Māori vaccination effort.
“We’ve seen the threat that this current covid-19 outbreak is to the wellbeing of Māori communities with a total of 560 Māori cases recorded.
Watch the covid-19 update
Covid-19 update: Video RNZ News
“In the last two weeks, Māori have made up 45.7 percent of total cases vs 28 percent throughout the entire outbreak. Although sobering, these numbers reinforce why vaccinating our communities is so important,” he said.
“So I say to the Māori people, covid-19 is on the doorstep of your houses, do not let it enter and the best course of protection still remains for us to vaccinate our people.”
94 community cases
New community cases of covid-19 jumped to 94 today — the highest total in the current outbreak, the Ministry of Health reports.
Of today’s cases as at 10am, 41 are linked — 26 of which are household contacts — and 53 are unlinked, the ministry said in a statement.
There are 38 people in hospital – eight in the North Shore, 12 in Middlemore, and 18 in Auckland.
Five people are in ICU or HDU.
The total number of cases in the outbreak is 2099. That is made of 2030 cases in Auckland (1360 of whom have recovered); 52 in Waikato (seven of whom have recovered); and 17 in Wellington (all of whom have recovered).
And 183 cases from the past 14 days remain unlinked.
The ministry said there were 2039 contacts.
A total of 16,921 tests were processed around the country yesterday, 12,688 being in Auckland.
Vaccination numbers
In terms of vaccination numbers to date, 6,387,870 vaccines have been administered: 3,582,822 (85 percent) first doses, and 2,805,048 (67 percent) second doses.
Of those, 379,563 (66 percent) Māori have had their first dose and 258,018 (45 percent) have had their second dose.
And 231,295 (81 percent) Pasifika have had one dose of the vaccine while 171,818 (60 percent) are fully vaccinated.
In Auckland, 89 percent of the eligible population has had one dose of the vaccine and 72 percent has had both doses.
Epidemiologist Professor Michael Baker says his biggest concern is that the spread of the delta variant of covid-19 in New Zealand is an “outbreak of the unvaccinated”.
The country’s largest city Auckland has now been living with tough restrictions for two months.
Asked why the city is still experiencing so many cases (57 today – plus three in Waikato) Professor Baker said “lockdown fatigue” was undoubtedly a factor.
“We hear a lot of anecdotal reports of that. Also, the rules were relaxed a bit in terms of more social gathering outdoors and outdoor gatherings on the face of it should be relatively low risk because there’s better ventilation, but of course, it does provide more opportunities for mixing and they may turn into indoor parties and so on,” he told RNZ Checkpoint tonight.
“So I think we are seeing those effects.”
He said on the plus side, as the number of people vaccinated increased, the reproduction number would decrease.
Hurting Māori and Pasifika
However, the outbreak could still get out of control, hurting Māori and Pasifika in particular.
“The unvaccinated are increasingly Māori and Pacific people. So we do run the risk of this becoming a very unequal outbreak, and I think that’s a really critical factor that government needs to look at, at the moment.”
Professor Baker also said a level 4 lockdown may still be necessary, depending on the outbreak’s movement.
“I don’t think that we can rule out the need for some kind of circuit breaker lockdown in the future, but at the moment, it looks like the system is managing these numbers.”
He said if the country could reach 90 percent vaccination coverage, it would be reasonable to move to level 2.
He said Auckland’s border could be dropped by Christmas “potentially” if there was uniformly high vaccine coverage across Aotearoa.
“This is where I think we could definitely move down to alert level two, which actually puts very few barriers in the way of the virus, in practice, and in addition, we could have the schools open again.
“So I think that would be a good point to make that move.”
But it was critical that high vaccination coverage included Māori and Pasifika demographics, for dropping the border to be safe, he said.
The government will announce a new “covid-19 protection framework” on Friday for when the country is at a higher vaccination rate.
On Wednesday, Covid 19 Response Minister Chris Hipkins will provide up-to-date advice on schools reopening.
Northland will move to level 2 at 11.59pm on 19 October.
Parts of Waikato in level 3 will remain there with a review on Friday.
Auckland will remain in level 3 with current restrictions for another two weeks.
For Auckland, Ardern acknowledged that it had been a long time to be living with restrictions.
“But those restrictions have made a huge difference, they’ve helped us to keep case numbers as low as possible while we continue to vaccinate people,” she said.
Ardern said non-compliance with level 3 rules had been one of the biggest contributors to new cases.
This article is republished under a community partnership agreement with RNZ.
Inside the Goroka Provincial Hospital, in stark contrast, the gloom of death hangs in the air.
Sister Lynnette Babah has never seen anything like this before in her entire nursing career.
The past few weeks have been the most difficult in her life, testing her mettle, her physical willingness, her mental resolve.
Death is everywhere.
The Angel of Death
It seems like the Angel of Death, with a sickle, has swept into the Eastern Highlands and has a bed at the door of the hospital.
Death pervades the wards, the beds — even the cleaning agents cannot mask the stench of cadavers, and life here, even for the caretakers of the sick, is a misery, pockmarked by tears of grief.
It is easy to see why. Covid-19 and its delta strain are draining every ounce of life out of the victims.
The covid that every Papua New Guinean thought they are immune to is finally wreaking havoc with a rising death toll in Goroka, Mt Hagen and the capital Port Moresby.
Despite warnings, despite calls to vaccinate, many victims, both educated and illiterate, have fallen victim to the virus.
Last week, I was one of few journalists from Port Moresby that accompanied a team to visit Goroka.
I can tell you, it was nothing like normal. I’d be lying if I said I wasn’t scared.
Goroka Provincial Hospital … now at Ground Zero in PNG’s fight against the covid-19 outbreak. Image: PNG govt
A shocking reality
In all of my reporting career, this is the first major ground zero medical emergency I have walked into and I was shocked into reality by what I was witnessing.
In Papua New Guinea, it is common to be drawn to a moment of euphoria or sadness; you see a mother or a child crying in a flash of gladness or sadness, your tears will follow that emotional outpouring.
You know when you find a hardened nurse tear up, you instinctively know something is not going right.
The loss of lives, desperation of the situation, sleepless nights, lack of rest, lack of medicine, equipment, even the simplest things like a pillow, they all add up to melting the heart of a helper.
Our arrival with the Team Sana medical team sort of sparked the built-up emotion in Sister Lynette and she burst out in tears.
She was comforted by the doctors and as she gained strength, she said with tears in her eyes: “It’s heartbreaking to see my patients struggle and die every day.
“In one day, we have 9 to 15 patients pass away and in one day we also struggle to save a life, it is really heartbreaking for me as a nurse to see them die in pain every day.”
A distraught mother
Outside, a distraught mother, Mary Anoixa (pronounced Anoiya), and her 10-year-old daughter, Josephine, are covered in black charcoal and have been camping outside of the Goroka Hospital morgue for two weeks.
Their home is a long way away in Lufa district.
They are here hoping to see her elder son’s face for the last time before he is put into the coffin and taken away for burial.
Her 29-year-old nephew, Nicky Anoixa, passed away two weeks ago from a severe attack of the covid-19 at the Goroka Hospital.
She shed a tear as she remembered the last time, she saw her nephew and held him before he was taken to the critical covid-19 ward at the Goroka Hospital on September 30.
She has camped at the site for the last two weeks, hoping to catch a glimpse of son’s body but as covid-19 nurses and doctors have advised her, it will never be possible.
They told her she would only be able to see her son being taken out of the morgue and placed into his coffin before the ambulance takes him away for burial.
The closest the family will get to see will be his coffin driven by the ambulance to his burial site.
Managing the virus surge
Governor Peter Numu said his province was managing the covid-19 virus surge despite all the struggles they were facing financially and socially.
Numu said he was thankful that he had allocated an approved budget of K1.5 million (NZ$605,000) to help with the covid-19 operations in the province, hence he was appealing to all other leaders to lend a helping hand.
He said September 30 was a day in his political life that he would never forget — he witnessed 10 people die of the coronavirus and received a phone call that 10 more of his family, officers and supporters had also died.
Numu urged people to change their attitudes so that they could better address the surging pandemic virus.
“Covid-19 is real, I made a visit there to the hospital and I saw for myself people dying,” he said.
“Like one day, I will never forget that day, 10 people died, five at Goroka Hospital, two dead upon arrival, and three deaths from Kainantu – a total of 10 reported cases.
“But on that day, I also received a lot of phone calls that about five or six people, unreported, died and these are healthy people I am talking about, some are my coordinators, some my supporters, some even my family members… many people died leading to this day.
“We want a complete lockdown for a period of 14 days; I know the people will say it is against their constitutional right and that we are suppressing them, but these so-called constitutional rights are qualified rights, which must also be consistent with other laws, like in this case we have the Pandemic Act, so when you want to exercise your right, you must know that the Pandemic Act is there to control the spread of Covid-19.
“Any measures put in place are law under the Pandemic Act.”
A strange stench
It is 11am as we enter the Goroka Hospital and the strange stench of the dead can still penetrate through the medicated disposable masks we are wearing.
And as if this is not bad enough, no one wants to talk to us as everyone we come across is “running” (not walking) to and from every ward and every building in the hospital.
Further, the feeling of entering a contaminated hospital is something one would not even dream of or dare do, but how can we as journalists avoid that?
But what is worse is the sound of the ambulance sirens going in and out of the hospital – some coming in with patients in critical condition and others carrying dead bodies, while others carry coffins out for burial.
And this has been the norm for the last two weeks– every 30 minutes, 20 minutes and 10 minutes.
The front of the hospital is piled up with all kinds of medical supplies from donor partners, organisations, students and others.
At the back of the hospital, there is a gate that never closes – opens 24/7 because buses, cars, and even ambulances come in every interval to bring in patient
A Highlands social media posting by Chloe Mandrakamu in Papua New Guinea. Image: FB CM
s, some dead-on-arrival, while others make it to see another day, while the rest die from shortage of oxygen or have arrived late and not in time to be saved.
The clock is ticking
Everywhere in all these wards, someone is struggling to breath; an oxygen cylinder has run dry, a patient is screaming, families are begging for doctors to save their loved ones and next door someone has just passed on — there is wailing all over
The minute chores, hourly chores and a day’s chores are all about covid-19, staff are all dressed in PPEs — some quite worn out; everyone is masked and many are in complete apparel and rushing to and from every corner of the covid wards, emergency and morgue like zombies … the clock is ticking and they have to race against time in order to save a life.
Around the morgue area, family members sit in anticipation, hoping to see their loved one’s face for the last time – even knowing very well they cannot open those body bags.
There is wailing and mourning, people covered in black soot, some turn up with the best blankets to cover their loved ones stored away in those two big, refrigerated containers.
And one thing is for certain, the heartbreak they are going through is nothing compared to that of a normal dead – for the last time they see their loved ones is when they bring them to the wards, when they pass on, relatives cannot even say goodbye — they do that after they have been put in a coffin and driven away in their ambulances — that has been the norm.
A seven-member team of PNG’s National Emergency Medical Team (EMT) — Team SANA — was deployed to Goroka on a 14-day mission to support the Eastern Highlands Province covid-19 response.
Eastern Highlands — now a high-risk highlands province — is currently experiencing a surge in critical covid-19 cases, and Team Sana’s presence on the ground is proving vital in helping the province manage its situation, while providing temporary relief to staff on the ground.
The team has been working with the provincial health authority to build capacity on the clinical management of severe covid-19 patients, incorporating safety and infection prevention control measures, isolation, conducting hands-on training for severe patient management and vaccine advocacy among health workers and patients.
According to the John Hopkins University covid-19 dashboard, Papua New Guinea has 24,041 confirmed cases and 266 deaths, but experts say the real toll is far higher. Only 0.7 percent of the country’s nine million people are fully vaccinated.
Gorethy Kenneth is a senior PNG Post-Courier journalist who accompanied the Team Sana mission.
This content originally appeared on Asia Pacific Report and was authored by APR editor.
Director-General of Health Dr Ashley Bloomfield said the record-breaking numbers provided a “huge boost” to New Zealand’s fight against the coronavirus.
“People across the motu embraced Super Saturday like their communities’ lives depended on it. It was inspiring to witness as we know the Covid-19 vaccine is key to our efforts to control the virus,” he said.
Dr Bloomfield said Auckland did “incredibly well” with 41,081 people vaccinated there yesterday, including 9,039 first doses and 32,042 second doses.
“They’ve hit 89 percent of their eligible population who have had their first dose and are tantalisingly close to reaching 90 percent,” he said.
‘Get vaccinated asap’ plea
“I continue to urge everyone in Auckland who hasn’t received their first vaccination to get vaccinated as soon as possible. And remember, we’re not stopping at 90 percent – the higher, the better for everyone.”
There has now been a total of 6314,182 doses given in New Zealand – 3,565,822 (85 percent) first doses and 2,748,360 (65 percent) second doses.
Epidemiologist Professor Michael Baker today called for more mass vaccination events, saying the first one united the country.
The Super Saturday Vaxathon final numbers – 130,002. Source: RNZ/Ministry of Health
In its statement, the ministry said two of the Waikato cases were linked to earlier cases and they are investigating any links the other two may have.
“One lives in Hamilton and the other has an address in Kihikihi. It is possible that the Kihikihi case is the source of the wastewater detections in Te Awamutu, however this has not yet been confirmed.”
23 cases remain unlinked
It said 28 of today’s 51 cases were linked, of whom 18 were household contacts, and 23 remained unlinked with investigations continuing.
The ministry also said it could also confirm that there was one household in the area Wellsford with cases, after two positive detections in wastewater.
“Wellsford residents are urged to remain vigilant and get tested if they have any symptoms.”
Things were looking very bad three months ago for both Papua New Guinea and Fiji. The two Pacific countries were each looking very vulnerable to the covid delta variant, albeit in different ways.
On July 10, PNG recorded its first official delta case, and the nation’s health professionals were soon warning the combination of very low testing rates, high percentage of positive tests and an extremely slow vaccine rollout provided a “recipe for a major spread”.
Fiji was already in the thick of it at the time. After the deadly delta strain entered the country via a quarantine breach in April, per capita infection rates became the highest in the world in the middle of the year.
By contrast, PNG is in the grips of a major wave, with less than 1 percent of the total population fully vaccinated. PNG is trailing much of the world.
Why have two Pacific countries, which share Melanesian cultural connections, handled their vaccine rollouts so differently?
Not a matter of geography or vaccine supply Fiji’s daily infection rate today is 4 percent of what it was at the peak, and it’s falling. Less than 50 new cases are currently being reported on average each day.
In PNG, the official infection rate is now averaging just under 300 new cases a day, but this drastically understates the reality of what is happening in the country.
It’s not simply a vaccine supply issue. At this stage of the global crisis, PNG, like Fiji, has received substantial vaccine deliveries — principally from Australia, New Zealand and the COVAX vaccine delivery initiative.
In fact, thousands of PNG’s early deliveries went to waste because the health authorities were unable to use them. The PNG government has recently made the best of a bad situation by re-gifting 30,000 vials donated by New Zealand to Vietnam.
Our #PacificHub leader @CainTess comments on the challenges #PNG faces in its #Covid-19 vaccine rollout after having to transfer donated vaccines to Vietnam
PNG’s geography does present some challenging physical barriers to distributing vaccines – its legendary mountainous terrain and the remoteness of many of its inhabitants are well known.
But companies from Digicel to South Pacific Brewery manage to penetrate the most inaccessible areas with their products despite these difficulties. And the authorities manage to deliver the vote across the nation every five years in what is one of the world’s most extraordinary democratic exercises.
With its own rugged terrain and dispersed populations across multiple islands, Fiji has also faced major physical impediments to its vaccine rollout.
The major difference: leadership and belief We get closer to the problem when we think in terms of trust, understanding and belief.
Fijians have embraced the vaccination rollout almost as one, following the guidance of their medical authorities and falling in line with the firm “no jabs, no job” policy of its prime minister, former military commander and coup leader Voreqe Bainimarama.
In PNG, the term “vaccine hesitancy” understates the problem. One survey earlier this year showed worrying low willingness to take the vaccine, and another survey of university students showed a mere 6 percent wanted it.
These dramatically contrasting pictures cannot be explained fully through differences in education standards, or the quality of medical advice and attention.
To be sure, Fiji leads PNG in these respects — Fiji has 99 percent literacy compared to just over 63 percent in PNG, according to the latest available figures. And while Fiji’s medical system has its challenges, the decline in PNG’s health services due to chronic lack of investment puts it in a very different category.
In PNG, trust in leadership has flagged following decades of frustration with growing wealth inequality and concerns over governance and transparency.
I know how quickly Papua New Guineans tap into what’s happening in neighbouring Australia, too. They will have seen how the public debate in Australia has dented confidence in the AstraZeneca brand — the mainstay of their own vaccine supply.
But perhaps most troubling of all is the sense that many Papua New Guineans have developed a fatalistic belief that covid is just another health challenge to add to the litany of other serious problems facing the country, among them maternal mortality, malaria and tuberculosis.
It’s almost as if they believe this is all somehow PNG’s lot. But it doesn’t need to be.
Half of Papua New Guinea’s parliamentarians are still not vaccinated despite widespread calls from the government, the business community, churches and civil society for people to get vaccinated.
A Post-Courier survey over the past few weeks showed that only 57 Members of Parliament out of 109 — two MPs have died — have been fully vaccinated.
The survey carried out by the paper and published in the weekend edition indicates the following:
National Alliance – all 9 MPs fully vaccinated
Pangu Party – 22 vaccinated out of 38 MPs
United Resource Party – 5 vaccinated out of 8 MPs
Social Democratic Party – 2 of their MPs fully vaccinated
Our Development Party – 2 of their MPs fully vaccinated
People’s National Congress Party – 3 out of 14 MPs vaccinated
United Labour Party – 1 out of 8 MPs recorded being vaccinated
Most of the two-men and one-man party members have also received their vaccinations, while others have refused, or have not been reachable.
It was confirmed that most of the party leaders have been vaccinated, but their MPs have not.
When asked what their reasons were for refusing the vaccination regimes, their answers varied.
Some MPs ‘scared’, some read ‘too much’ social media
Some members told the Post-Courier they were scared, others said they were still sceptical of getting jabbed, some said they were still deciding, while a few said they read too much on social media and were not sure.
Three others joked they did not want to “turn into beasts”.
This comes as the nation is hesitant in its vaccination drive and the country’s National Control Centre and government struggle to administer its approved vaccinations.
The results also come as the Control Centre now battles a surge in covid-19 cases and the Delta variant with 10 provinces now declared high risk — including Western, Chimbu, Sandaun (West Sepik), Enga, Western Highlands, Hela, Eastern Highlands, Jiwaka, Morobe and Southern Highlands.
Some of the leaders from these high risk provinces have not been vaccinated, according to the Post-Courier survey.
The newspaper has a list of all the MPs that have been jabbed and those that have not been vaccinated to date.
Aotearoa New Zealand is well over halfway to the government’s “Super Saturday” day-long goal of 100,000 vaccine doses today, with more than 70,000 doses given out by 1pm.
By 2.39pm, there had been a total of 90,616 doses across the country, according to the Ministry of Health.
Vaccine clinics are open across the country as health workers target a 90 percent vaccination milestone.
Prime Minister Jacinda Ardern and Director-General of Health Dr Ashley Bloomfield were going around the Wellington region, as they joined the drive to get people vaccinated.
There was no media conference today. In a statement, the ministry said there were also two new cases in managed isolation.
It said 20 of the community cases were linked, and 21 remained unlinked with investigations continuing.
There were 124 unlinked cases from the past 14 days.
One of today’s new cases was in Waikato. The ministry said the case was a household member of two existing cases and was already in a quarantine facility in Auckland.
There are now 31 people in hospital, all in Auckland, including six in intensive care.
More than 120 extra vaccination sites will be open for New Zealand’s ‘Super Saturday’ event tomorrow, with the Ministry of Health saying vaccines remain the country’s “number one protection against covid-19”, reports RNZ News.
The event will run from 12pm to 8pm on Saturday and will be broadcast on multiple platforms, including TV3, Māori Television and on Hahana’s Facebook page.
Well-known celebrities, influencers and health professionals will front the live broadcast to help capture the atmosphere and experiences of those receiving their first or second vaccine.
RNZ will be providing on air and online coverage, including a live blog, from across the nation.
There was no media conference today. In a statement, the ministry said 34 of these cases were linked, 10 were household contacts, and 31 remained unlinked with investigations continuing.
There have been 107 unlinked cases in the past 14 days.
While the cases were all in Tāmaki Makaurau, a second test for covid-19 in Te Awamutu’s wastewater returned a positive result.
The sample was taken on Wednesday, after detection of covid-19 in wastewater on Tuesday.
As part of the effort to get everyone in Aotearoa vaccinated against COVID-19, a dedicated team has been put in place to support people with disabilities to access the vaccine. Read more about these important services here: https://t.co/qMzckiq0Wepic.twitter.com/Kp68QQojYQ
— Ministry for Pacific Peoples (@Pacific_Peoples) October 12, 2021
This article is republished under a community partnership agreement with RNZ.
National Māori Pandemic Group Te Rōpū Whakakaupapa Urutā co-leader Dr Papaarangi Reid has supported a return to a level 4 lockdown over the covid-19 virus crisis, saying she is concerned about the trajectory of the outbreak in Auckland.
“We’re at a very, very dangerous time in this outbreak in Auckland especially,” she said.
Professor Reid told RNZ Morning Report the group supported calls for a level 4 circuit breaker lockdown in Auckland to give Māori a chance to increase vaccination rates.
“… a circuit breaker would be ideal, to go back to a sharp level 4 conditions to buy us some time to increase vaccination rates and to decrease the spread that’s obviously happening in the community in Auckland,” she said.
There was no media conference today. In a statement, the ministry said 34 of these cases were linked, 10 were household contacts, and 31 remained unlinked with investigations continuing.
There have been 107 unlinked cases in the past 14 days.
There was also one new case in managed isolation.
Thirty-four people are in hospital, with six in intensive care.
Politics ‘promoted over health’
Dr Reid was concerned politics were being promoted over public health, adding that a 95 percent vaccination rate would help everyone.
“Because if anybody, any group is getting sick at a disproportionate rate, they will be taking up places in hospital, they will be taking up beds in ICU, that when our friends and whānau have a heart attack or have a car crash they won’t be able to access, get surgery done.
“It is in the best interest of the whole community that no subgroup in the community is left behind.”
Yesterday, Health Minister Andrew Little said the capacity of ICU and HDU beds nationwide could be surged to 550 beds.
“If we had to provide additional surge capacity to convert beds for ICU-level care then as a result of the work that started at the end of last year the DHBs tell us they can surge that up to 550 beds — that would be at the cost of other treatment and other patient care.”
Reid said some people were also taking longer to decide whether to get the vaccine.
“Different groups have different experiences, so for some people it’s not relevant, they don’t think covid is real.
‘Don’t believe it is relevant’
They don’t believe it’s relevant in their lives. We see those people gathering at protests.”
She put it down to the lack of suitable housing, mental health and addiction issues, and others who could not follow rules because they were in the cash economy and not subsidised by MBIE.
“… and that disproportionately falls on Māori. So whether or not you believe in how it was designed, we’ve got a different distribution of the population who are more likely to take longer to go through that decision-making process,” she said.
“That is beginning to change, but we still are several weeks behind in our catch up and we need that time.”
This article is republished under a community partnership agreement with RNZ.
This content originally appeared on Asia Pacific Report and was authored by APR editor.
A coalition of Māori health organisations in Auckland is urging the New Zealand government to return to a covid-19 elimination strategy, saying many Māori will die if it does not.
They say the government’s move to relax restrictions while the number of cases among Māori are rising and the vaccination rate is still low painted a picture of Māori as “acceptable collateral damage”.
The coalition of Hāpai Te Hauora, Te Whānau o Waipareira Trust, Te Hā Oranga and Raukura Hauora o Tainui said the elimination strategy had acted as protective korowai while the vaccination programme caught up, but it had now been dropped.
“That will no doubt result in loss of lives, with Māori being a major casualty,” they said in a statement.
The general manager of Ngāti Whatua provider Te Hā Oranga, Boyd Broughton, said he was incredibly frustrated with the way the pandemic was panning out.
Nearly two weeks after Auckland was moved to alert level 3, the number of cases was steadily growing.
Running vaccination centres
His organisation had been busy across Auckland, running vaccination centres, setting up mobile clinics, helping get in contact with hard-to-reach communities.
Things were catching up, he said, which was what made the shift especially frustrating.
“It’s very disappointing when there’s a shift from the elimination strategy to a suppression strategy and it comes at a time when Māori case numbers are rising, our vaccination rates are still lower,” Broughton said.
“So that’s why we’re left with the impression that Māori are an accepted collateral damage from this government, and this government making decisions.”
Health Minister Andrew Little rejected that assertion.
“No not at all,” he replied when asked on RNZ Midday Report.
“That’s why we have the level 3 restrictions in place for the length of time that we have in Auckland, and we went into level 3 for Waikato and Northland when we thought there were risks there.”
Selah Hart, chief executive of public health service Hāpai Te Hauora … “We want to ensure that … the system doesn’t turn its back on the forgotten people once again.” Image: Hapai te Hauora/RNZ
Elimination more equitable
But public health service Hāpai Te Hauora chief executive Selah Hart said trying to eliminate covid-19 would be more equitable, as suppression would still see the virus in vulnerable Māori communities.
“We as a country have missed many marks in being able to get us on track to ensuring that those who are always most underserved across any health statistics aren’t going to carry the weight of this pandemic on their shoulders,” Hart said.
Hart said it was particularly disheartening to see what Māori health experts had warned about for nearly two years being borne out.
“We want to ensure that those people don’t get forgotten about, that our communities that are now bearing the brunt of this thing are not forgotten about and that the system doesn’t turn its back on them once again,” she said, saying a familiar pattern of history was now repeating.
Broughton said he understood patience with the lockdown was wearing thin, and it was a feeling held by many Māori whānau too. But he said it would be different if there was better support for vulnerable whānau to be able to stay home.
Little said the government was putting significant effort into the vaccine rollout.
“We’ve seen an amazing surge of vaccinations for Māori and Pacific in the last couple of weeks,” Little said.
“That’s great, we want to continue that.”
Restrictions won’t be relaxed
He said restrictions won’t be relaxed further until the government saw sufficient levels of vaccination in all groups, including Māori.
But Broughton said he had little faith.
Māori health providers called for a different type of vaccine rollout early this year, but they were rebuffed and were now playing catch up. He said he had warned that static vaccine clinics would not reach Māori, and now they were having to play catch up with mobile clinics.
Now, he said Māori providers were being dumped in an avoidable catch-up position yet again.
“We raised these issues that where they’ve put things doesn’t work, how they’re delivering doesn’t work, the messaging doesn’t work.
“But the decision-makers are non-Māori and we’re having to tidy up, essentially.”
He was worried the government had buckled too early, putting whānau at great risk.
In the coalition statement, the head of Whānau o Waipareira Trust, John Tamihere, had a warning for the government.
“If Māori lives are lost because of this denial, we will take civil action in manslaughter,” Tamihere said.
This article is republished under a community partnership agreement with RNZ.
All 252 people reported to have died in Papua New Guinea from the covid-19 pandemic have been unvaccinated, says Health and HIV/Aids Minister Jelta Wong.
He also said that 99 percent of covid-19 patients in hospitals around the country were also unvaccinated.
He told Parliament yesterday that “100 percent of the patients are in critical care and requiring oxygen”.
“Official cumulative numbers of those affected by covid-19 stand at 23,365, with 252 lives lost,” he said.
“But the official figures are nowhere near the actual numbers in the provinces.
“Just like other developing countries which have [gone through] a third wave of the covid-19 delta variant surge, the undeclared number of infections and deaths is much higher.”
Wong said some people had died in villages.
Cause of death ‘likely unknown’
“It is unlikely that the cause of their deaths will be known and will not be recorded,” he said.
He said the healthcare system had been underfunded for decades and Papua New Guinea was still a developing country “facing the challenges of data collation”.
Wong pointed out that the increasing number of sick or dead people now was motivating many to get vaccinated.
“Demand is rising considerably,” he said.
“So much so that while a few months ago we had vaccines expiring, now the government [wants] to bring new doses before the end of the year.
“There is a significant amount of personal protective equipment distributed to the provinces.
“But the lack of visibility on usage and remaining stockpiles is proving a challenge and better data and feedback systems are being developed.
“It includes the Health Department building a dashboard to better monitor this data.”
The World Health Organisation (WHO) has developed guidelines on covid-19 therapeutics which is regularly updated, he said.
Miriam Zarrigais a reporter for The National. Republished with permission.
The plan for New Zealanders with covid-19 to isolate at home suggests the government believes the spread is wider than had been thought, epidemiologist Professor Rod Jackson says.
Covid-19 Response Minister Chris Hipkins said home quarantine would be introduced “fairly soon” as a necessary step to prevent MIQ spaces being limited even further for people coming to New Zealand from overseas.
“Last night, there were 75 unlinked cases in Auckland. What that means is there’s a lot more cases out there.”
He said the speed of the spread of delta variant makes this outbreak worse than any previous one.
“I think the government’s clearly signalling that MIQ is going to be overwhelmed, the next thing is hospitals are going to be overwhelmed, everything’s going to be overwhelmed,” he said.
“We’ve just got to got to slow it down as much as we can.”
‘Huge risks’ with home isolation
There were “huge risks” involved with home isolation, he said, “but to me, it suggests that … they believe this problem is much much wider than we thought”.
“We are in a race against time to get everyone vaccinated, we just have to use everything in our power to slow [the outbreak] down as much as possible.”
Dr Jackson said vaccination should be mandatory for more sectors.
“I think it has to be the police, it has to be supermarkets. The other thing is that businesses are crying out for the licence to introduce their own mandates.”
With more than 80 percent of eligible New Zealanders having had at least one vaccine dose he said “the tide was turning” against those who were not vaccinated.
Covid spreading among rule breakers Dr Jackson said he had supported the move to level 3 for Auckland last month, and believed returning to a period of level 4 lockdown may have little effect on the growth of cases.
“Covid is spreading among a group of people who are breaking the rules,” he said.
“You can be really hard on them, but you’re probably not going to ever stop them.”
University of Auckland public health associate professor Dr Collin Tukuitonga is sceptical level 3 had made little difference to the outbreak.
“That’s a very narrow view,” he said.
“The people who don’t obey the rules is only a subset of the total number of people who are likely to move around and spread the virus.
“Yes, these are people that are at most risk of spreading it but if you permit people to move around more than we did before you will no doubt transmit the virus around.
“I can’t see how you can say that level 3 and level 4 are the same risk.”
The drop to level 3 was premature and very risky for Māori and Pasifika where vaccination rates remain low, he said.
“I was on the record as saying tired Aucklanders and business people got the louder voice this time, and those of us in public health had a quieter voice.”
The government should be prepared to go back to level 4 if things got really tough, he said.
Home quarantine ‘not for everyone’ Dr Tukuitonga told Morning Report isolating at home would not be suitable for those living in crowded multigenerational households.
“It’s not for everyone,” he said.
“You’ve got to be quite clear about the criteria, you got to have a group of people you can trust to do the right thing, you need to make sure they have a good understanding of the risks, the facilities at home have got to be up to scratch.
“It can’t be a small state house with three bedrooms and 12 people.”
Dr Tukuitonga said anyone isolating at home must understand the risks involved, could be relied on to follow the rules, and have a suitable home.
He said some may think the move was risky, but it’s going to have to happen with cases growing.
“I know some of my public health colleagues will say ‘absolutely not, this is a highly, highly risky measure’, but as I say, you’ve got to be pragmatic,” he said.
“When we run out of facilities we’ve got to look at different options.”
This article is republished under a community partnership agreement with RNZ.
For me and many others in prison, COVID-19 has been an emotional roller coaster. The Delta variant wave is just one more ride. I made it through the first round, will I make it through this one?
I’m 53 years old and I’ve spent 35 years of life in prison. I’ve long since come to grips with the powerlessness that is every prisoner’s lot. But COVID has taken that powerlessness to another level.
Many of us don’t know if we are going to live long enough to finish our prison sentence no matter how short it is. The vaccine, for those of us who have gotten it, has reduced the risk of death drastically. Many haven’t gotten the vaccine due to lack of trust in the government. But I got it, because after what I have witnessed during the first wave, I felt it may be my only way to get out alive.
But that is not our only concern. An immediate concern now is how the New York Department of Corrections and Community Supervision (DOCCS) is going to respond to the new wave of the pandemic and what policies they are going to enact this time. Throughout the pandemic and long before that, DOCCS has lost trust through its actions. The pandemic only gave more proof of how cruel the prison system is.
COVID Exacerbates Abuse and Neglect of Incarcerated People
In prison, our medical care is subpar to begin with during the best of times. Since the pandemic started it has gotten much worse. The State of New York has used COVID-19 as an excuse to take away our rights and privileges as well as to abuse and assault prisoners. The state also refuses to provide necessary medical care, including in my own case.
I myself had two issues that needed addressing when the pandemic hit: a sebaceous cyst that was pushing against a nerve in my neck and was scheduled to be removed, as well as a molar tooth that broke off at the root. When the pandemic started, all outside appointments were canceled. Over 18 months later, I still have not received treatment for either issue despite multiple requests. I deal with constant untreated nerve pain and chewing my food is extremely difficult and painful.
My story is far from unique. Many people I have talked to have had their medical issues sidelined since the pandemic began. Since the Spring of 2020, all outside medical appointments and only the most immediate emergencies were seen in the prison hospital.
I am known as a guy who writes about what occurs in prison, so people talk to me about what is happening. In addition to medical issues, I hear about physical abuse at the hands of guards, which has increased as well. Neglect and physical assaults of prisoners by guards in New York State has been the worst that I’ve seen in the four states I’ve done time in over the past four decades.
In recent years, these assaults and deaths by lack of medical treatment have led to lawsuits and news stories that have brought attention to the issue. For example, in 2015, Samuel Harrell was killed in Fishkill Correctional Facility by guards known as the “beat up squad.” And more recently, Layleen Polanco died at Rikers while in solitary confinement, after the jail’s failure to treat her medical condition.
The state has placed more cameras in the facilities and mandated that body cameras be worn by some officers. The problem is that the guards know where the cameras’ blind spots are and who is wearing a body camera. They are then able to abuse people out of sight of the cameras, and I have witnessed this several times.
And I have also experienced abuse. I have been relocated to many different facilities throughout the state. The medium-security facilities are worse than the maximum-security ones. There are many more blind spots.
The main “beat down” spot in Franklin Correctional Facility is in the back of a van they use to take you to the box (solitary confinement). The driver takes the long way, and the guards in the back dump you on the floor (while you are handcuffed behind the back) and proceed to “tune you up.” This can include knees, feet, elbows and fists applied to your face, head and torso.
When it happened to me, they pulled my legs out from under me so I landed hard face first, taking most of the fall on my shoulder (by ducking my head and twisting), and then they kicked me once in the kidneys and left me there.
Maybe it was the gray in my beard and possibly my white skin that got me off light. I have heard about and witnessed the results of much worse attacks. When I was in Upstate Correctional, a special housing unit/restrictive housing facility, they put a kid in the cell next to me who had both eyes closed and what looked like a broken nose. He screamed when he used the bathroom to urinate.
As bad as you think you have it these days, try experiencing this crisis from a position where you had very little control to begin with, then having that stripped away entirely. There’s an old saying in prison: Shit runs downhill, and prisoners are at the bottom of that hill. At no time has that been clearer than now.
While things have gotten better since the vaccine was offered, DOCCS has continued to deny people basic rights and privileges. For a long time, there were no regular visits from family and friends or “family reunion visits,” which are overnight trailer visits with partners and kids. These are crucial for families to stay connected. As of September 2021, DOCCS has reinstated family reunion visits. But as a result of not having these visits for a year and a half, people had much less contact with loved ones, and this has led to increased tension, violence and mental health-related incidents.
I am very concerned about what this new phase of COVID will bring. While the Delta variant is much less deadly for those who are vaccinated, we can still get very ill if we catch the virus. Add to that the fact that a large number of people in prison are not vaccinated, partly due to the mistrust generated by DOCCS since the pandemic began.
So we will see what the next round has in store. I’m not optimistic. Just like everyone else in the world, we wonder: Will it ever end? Will I survive? But in prison, we are even more powerless to protect ourselves, especially since COVID is only one of the threats we face. We also contend on a daily basis with abuse from correctional officers and lack of medical care. The pandemic has only exacerbated the poor conditions that I’ve experienced for 35 years in prison.
More than 6 million vaccine doses have now been given in New Zealand, with the vast majority of those who have caught covid-19 during the current outbreak unvaccinated.
Speaking at today’s government briefing – where it was revealed there were 55 new cases today – Covid-19 Response Minister Chris Hipkins said three-quarters of the eligible population were either fully vaccinated or booked in to do so.
Hipkins said just three percent of those in the current outbreak were vaccinated.
He said the best thing people could do to protect themselves and their whanau was to get vaccinated.
The government announced that the current covid-19 alert level 3 response in parts of Waikato and Northland will remain for another five days.
Auckland continues to remain at step 1 of level 3.
Truck driver case
Meanwhile, the Health Ministry said the risk from an Auckland-based truck driver who travelled to Northland on Saturday and had tested positive for covid-19 was low.
At today’s briefing, Director-General of Health Dr Ashley Bloomfield said the case was currently being assessed to identify any exposure events.
He said the case investigation was still in the early stages, initial information suggested a limited scope of exposure in Northland, given alert level 3 precautions within the delivery sector.
“The person was there from 3am to 12pm delivering to a number of places most of which were closed because of alert level 3 arrangements there.”
New Zealand covid media briefing today. Video: RNZ News
Dr Bloomfield said My Covid Record is now accessible to the public via mycovidrecord.nz.
People over 16 years will be able to view their vaccination record on this website by creating a my health account.
“From later November people will be able to access two different types of vaccination certificates: one for use in New Zealand and one for travel overseas.”
Dr Bloomfield said people can also request the Ministry of Health for their vaccination status.
The numbers
There were 55 new cases reported today
Of the new cases, 29 were epidemiologically linked, 26 were yet to be linked
The government said that within three weeks the military could set up 10 intensive care units at the main Noumea hospital and treat between 30 and 60 people over several weeks.
In addition, an air bridge is being set up to France to transport five intubated patients and others needing care in order to relieve pressure on the Noumea hospital, where in the past month 1300 patients have been admitted.
An Aircalin airliner is being modified to carry out this mission.
About 90 percent of critical care units are in use amid concern that a second covid-19 wave is likely to sustain demand while the hospital needs to maintain capacity for patients suffering from other conditions.
Currently, 69 covid-19 patients are being cared for in hotels, mainly in Noumea but also in the Loyalty Islands.
Health pass now needed
The authorities eased restrictions at the beginning of this week while rolling out a health pass now needed to go to restaurants and museums or for domestic air and ferry travel.
They urge the public to be vigilant and prudent, saying the next days will be critical for how the pandemic develops.
Schools are being reopened today, with students obliged to wear masks.
There has been a rush to get the online version of the health pass, clogging and slowing the system producing it.
A demonstration against New Caledonia’s mandatory vaccination against covid-19 and against the health pass. Image: Clotilde Richalet/Hans Lucas/RNZ
However, there have also been demonstrations across New Caledonia against the introduction of the health pass.
The gatherings — sometimes exceeding crowd size limits — were held outside the Congress and government building in Noumea as well as at the SLN nickel plant.
So far 53 percent of those over the age of 12 have been fully vaccinated or just under 46 percent of the total population.
Medical personnel as well as airport and port workers must get vaccinated by year’s end or face a US$1750 fine.
This article is republished under a community partnership agreement with RNZ.
As New Zealand switches from elimination to suppression, those who argue that covid-19 will become endemic and part of our lives either do not understand or ignore what this would actually mean.
Elimination has always been a tricky word because it implies eradication. But we have only ever eradicated one human disease — smallpox — and are close with several others.
For some, the end of elimination now means we should let the virus spread. But semantics matter less than policy.
If we don’t eliminate, we must still aim to contain, mop up, reduce close to zero and thwart this pandemic.
Because we certainly cannot live with endemic SARS-CoV-2.
The delta variant spreads ominously and without controls, every infected person, on average, would infect six more, then 36, 216, 1296, 7776, 46,656 — we would get to more than twice New Zealand’s five million with three more cycles.
“Once the virus gets out and starts spreading, if you struggle to contain it… it will find the most vulnerable communities, and once it makes its way into those communities it’s really hard to stop it,” Chris Hipkins told the guardian https://t.co/Z6bkiTY43M
We must continue to either stamp out the virus or keep case numbers very low. To contain case numbers, we need to keep up border protection, mask wearing, distancing, bubbles, contact tracing, testing of people and waste water, and vaccination.
Delta is nothing like the flu Our most common endemic infections include the common cold (caused by hundreds of different viruses that circulate freely) and the flu (caused by a group of influenza viruses).
Those who dismiss a mild case of covid-19 as being “no worse than the flu” have forgotten how appalling a case of flu really is. They might also have forgotten that, even with effective vaccination, influenza has a case fatality risk of about 0.1 percent — it kills about 500 people in New Zealand each year.
Yet some seem to expect that covid-19 will learn to behave and become endemic. Some even seem to welcome this, claiming a “disease becomes endemic when it is manageable”.
This is not true. Being manageable is not part of the definition of endemic disease. A disease becomes endemic when it is more or less always present in a population. It does not care whether it is manageable.
Seasonal influenza has a basic reproduction number (R0) of about 1.5, meaning one infected person spreads the disease to fewer than two other people, on average. This is why it takes very little to break the chain of transmission.
The annual flu epidemic declines because we have effective vaccines and because seasonal conditions during summer are less favourable to the survival of the virus.
However, as we already mentioned, the delta variant has an R0 of at least six. This will be as low as it gets from here onward. If a new variant supplants delta, it will do so because it is even more transmissible.
There will be no season for covid-19, no breaks in transmission, no declines in infectiousness. We have been struggling worldwide with this virus for 18 months, with spikes everywhere in every season.
School and business closures part of new normal If covid-19 becomes endemic, there will not be one or two people sick in a workplace or a home. We will have waves and clusters and multiple local outbreaks.
Schools and businesses will close for days, even weeks, because too many people are sick. It will cost the world trillions — consider what it has already done to global supply chains.
If covid-19 becomes endemic, the burden on our healthcare system will be immense. It will not involve a predictable, modest increase in hospital admissions. Waves and clusters will characterise endemic covid-19 in the same way they have characterised pandemic covid-19, overwhelming local healthcare without warning.
New: The Government hasn’t increased its surge contact tracing capacity since the start of the outbreak, despite the move to suppression, and daily cases in the low triple digits could see the tracing system overwhelmed.https://t.co/6ymqvcmcD7#nzpol#Covid19#Covid19nz
— Marc Daalder Wear a Mask, Scan QRs, Vaccinate (@marcdaalder) October 10, 2021
If covid-19 becomes endemic, Merck’s new antiviral drug Molnupiravir will be an important addition to the toolkit because it will be much cheaper than monoclonal antibodies, easy to store, easy to transport and people can take it at home.
The as yet unpublished trials suggest the treatment could cut hospitalisations in half, markedly improving outcomes for those already infected. But it will not reduce the number of cases by even one.
Treatment never does — only prevention, public health measures and vaccination reduce case numbers. Those who are less sick and treated at home could spread the virus even more.
If covid-19 becomes endemic, when the healthcare system fails to accommodate the latest wave, more people will die.
Long-term costs to health and economy Even if we managed to get covid-19 down to the severity of influenza (for an individual), endemic delta — with an R0 about five times that of flu and the fully vaccinated still able to become infected and spread — would still mean thousands of hospitalisations and deaths each year.
Just four cycles of delta infection could result in more than 250 times as many cases as four cycles of flu.
If covid-19 becomes endemic, every year, many of us will know someone who dies.
If covid-19 becomes endemic, more than a third of unvaccinated cases, even the asymptomatic, will have symptoms months later.
Flu leaves little lasting damage. Long covid damages the lungs, heart, brain, hearing and vision as well as the insulin-producing cells of the pancreas, causing diabetes.
The cost of covid-19 is so much higher than that of the flu, not just because of higher case numbers, hospitalisations and deaths, but more long-term damage and disability.
If covid-19 becomes endemic, we will live with a stressed, often overwhelmed healthcare system, with schools subject to unpredictable closures, with unsafe workplaces, with a disrupted economy, with our children under threat, with death and disability at a persistently higher level than we have known — probably for decades.
We do not care what the current strategy is called as long as we persist with border protection and public health measures until we achieve close to universal vaccination.
Otherwise, many thousands of New Zealanders will be hospitalised, die or experience long COVID.
Ultimately, we will need a sterilising vaccine (one that protects people from getting infected) because we cannot live with endemic covid-19.
If New Zealand’s border restrictions are loosened for arrivals from countries with high covid-19 numbers, South Auckland will see between 1000 and 1400 cases a week — even if vaccination rates get to 90 percent, according to modelling carried out by the Counties Manukau District Health Board (DHB).
Under the modelling prepared for the DHB, if strong border controls and public health measures remained in place and the vaccination rate reached 90 percent, the Counties Manukau region would see only 40 cases and one hospitalisation per week.
This number jumps to 200 cases per week if vaccination rates reach only 80 percent.
The scenario gets grimmer for South Aucklanders if border and public health restrictions are lifted.
The DHB’s modelling shows there will be at least 1000 cases and 30 hospitalisations per week with a 90 percent vaccination rate, or 1400 cases and 45 hospitalisations if vaccination rates reach only 80 percent.
Given rates remain well below 80 percent in much of South Auckland, University of Auckland public health associate professor Dr Collin Tukuitonga said the modelling was too conservative.
“I think the vaccination rates are too ambitious and I think we will probably get more cases than 1000 a week,” Dr Tukuitonga said.
“And as a result, it will have a greater impact on Māori and Pacific people. This could get totally out of control – in terms of what we’ve experienced in New Zealand up to now.”
Pressure already immense
The pressure on Middlemore Hospital was already immense given “Māori and Pacific are most affected by the inequities in our society”, Dr Tukuitonga said.
Dr Collin Tukuitonga … “The problem for Middlemore is that they are already stretched to their full capacity, even without covid.” Image: SPC
“If the government loosens public health measures, there will be more cases, and that’s the risk people need to be aware of.
“The problem for Middlemore is that they are already stretched to their full capacity, even without covid, as they are underpowered to serve the population size that exists within Counties Manukau.”
At the opening of a mobile vaccination bus last month, Counties Manukau Health Chief Executive Margie Apa said the hospital had already been working hard to increase its capacity for covid-19 patients.
“We have done quite a lot of preparatory work to increase our ICU [intensive care unit] and high-dependency units,” she said.
“But what that does do is take bed stock out of being able to look after the rest of our non-covid patients.”
According to a DHB spokesperson, the hospital has 18 intensive care unit (ICU) beds, seven high dependency unit (HDU) beds and a special respiratory ward for covid-19 patients.
Planning capacity increase
It is also planning ways to increase “hospital capacity to care for all patients in a safe way”, the spokesperson said.
“Middlemore Hospital has been the epicentre of the covid-19 Delta outbreak with more than 1000 cases since the pandemic began in the Counties Manukau region.
The team’s experience is now being applied to how services and patient care will be provided in the future.”
A medical specialist familiar with Middlemore Hospital and its intensive care unit said given what the modelling shows and the hospital’s capacity, the implications for South Aucklanders with pre-existing conditions were “very serious”.
“When a person goes into intensive care with covid, they can spend up to 16 hours a day lying on their stomachs and are spending between four to six weeks in there.
“If every week you get just a tenth of hospitalisations going into ICU, you’re still going to get pretty overwhelmed pretty quickly.”
Lot of people suffering
An increase in covid-19-related deaths was “a reasonable assumption to make, and there will also be a lot of people just suffering, as they are unable to get the relief they were hoping to get from other interventions that had been planned but will be delayed,” he said.
Opening the vaccination rollout to all Māori and Pacific people from the start, and having it led by South Auckland providers, was the only way for the current scenario to have been avoided, he said.
“The people of South Auckland have borne the brunt of so much for so long, and you have to think they have been let down.
“They should have been listening to people on the ground but it seems they never learn.”
Local Democracy Reporting is a public interest news service supported by RNZ, the News Publishers’ Association and NZ On Air. This article is published by Asia Pacific Report in partnership with LDR.



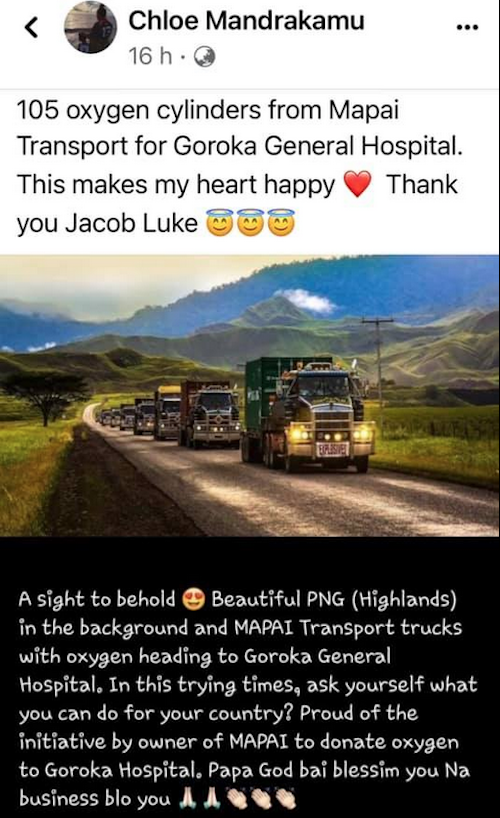
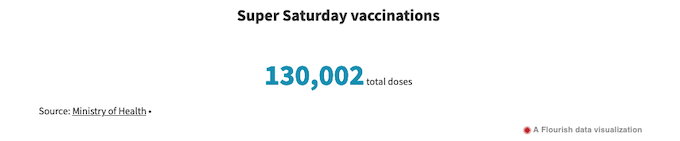

 Read more about these important services here:
Read more about these important services here: 






 Wear a Mask, Scan QRs, Vaccinate (@marcdaalder)
Wear a Mask, Scan QRs, Vaccinate (@marcdaalder)