What is Philippine President Rodrigo Duterte’s solution to vaccine hesitancy among Filipinos? Threaten them with jail time.
Duterte, in a meeting with pandemic task force officials yesterday said he would order the arrest of people who refused to get vaccinated.
“Kung ayaw mo magpabakuna, ipaaresto kita at ang bakuna, itusok ko sa puwet mo. Putang ina, bwisit kayo,” said an irate Duterte in edited footage of the meeting aired on television.
(If you don’t want to get vaccinated, I’ll have you arrested then I’ll inject a vaccine into your buttocks.)
“Magpabakuna kayo or ipakulong ko kayo sa selda (Get vaccinated or I’ll jail you in a cell),” he added.
He has also threatened to inject them with the version of anti-parasitic medicine Ivermectin intended for animals.
Duterte said his justification for such a drastic measure as arrest was the state of national emergency he declared over the country due to covid-19 and the dangers posed by unvaccinated people as possible “carriers” of the disease.
He conceded it was a “strong-arm” tactic for which he would find a legal way to enforce.
“I will think it over very hard, legally of course, in pursuance of a policy of crisis, this health issue,” said Duterte.
The President also said he would tell local government officials to “find” those who were unwilling to get vaccinated.
“I will order all the barangay captains to have a tally of all the people who refuse to be vaccinated,” said Duterte, adding that the Department of the Interior and Local Government should supervise the effort.
The Duterte administration is already notorious for its use of barangay lists to keep tabs on suspected drug users and peddlers, many of whom have ended up killed either in police operations or by unknown assailants.
Harshest vaccination policy
If Duterte makes good on his threat, his would probably be the harshest penalty globally for people unwilling to get vaccinated against covid-19 and would likely raise human rights concerns.
In Indonesia, its capital Jakarta announced it would fine people who refused to get vaccinated.
Will coercion and threat work among a majority of Filipinos unsure about getting their jabs? A Social Weather Stations survey conducted from late April to early May found that only three out of 10 Filipinos were willing to get vaccinated.
The top reason for this unwillingness was fear of side effects of vaccines being used — the most common is the Chinese Sinovac — and the belief that the vaccines were not safe or effective, according to SWS.
Lawmakers and civil society organisations have called on the government to ramp up its vaccination information drive to counter vaccine hesitancy.
Pacific Media Watch reports that the Philippines has logged at least 1.35 million infections and over 23,500 deaths since the pandemic began, but under 6 percent of its roughly 108 million residents have been inoculated with at least one dose.
The republic has now secured the delivery of 113 million doses from five vaccine manufacturers: Sinovac with 26 million doses, Sputnik V with 10 million doses, 20 million doses from Moderna, 17 million doses from AstraZeneca — and now a deal for 40 million doses from Pfizer.
Pia Ranadacovers the Office of the President and Bangsamoro regional issues for Rappler. While helping out with desk duties, she also watches the environment sector and the local government of Quezon City. Rappler articles are republished by Asia Pacific Report with permission.
Health Secretary Dr James Fong said the man’s death was being investigated by his doctors to determine if it would be classified as a covid-19 death.
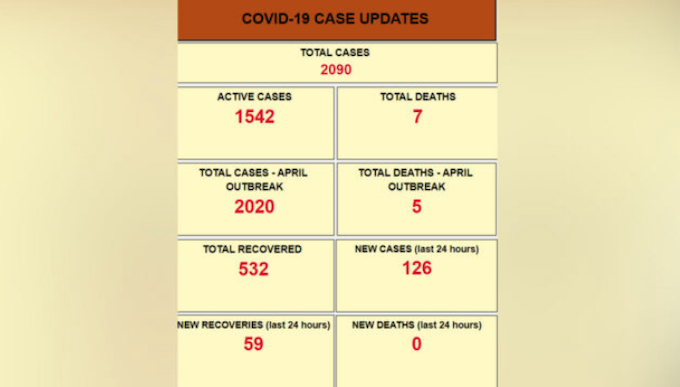
Dr Fong said 59 recoveries had also been recorded and there were now 1542 active cases in isolation.
He added that the number of covid-19 cases recorded since April this year had increased to 2020.
This meant that the total cases recorded since Fiji registered its first case last year stood at 2090.
Dr Fong said to date there had been 532 recoveries and seven deaths due to covid-19 in Fiji.
Five of the deaths were recorded during the current outbreak with eight covid-19 positive patients haing died from pre-existing non-covid-19 related illnesses.
The Health Secretary said one death was currently under investigation.
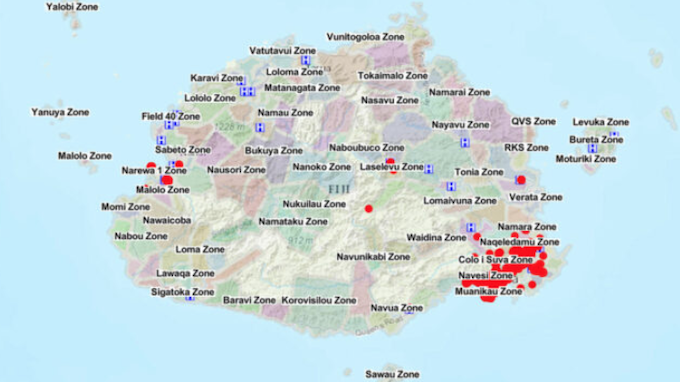
Fiji covid-19 clusters on Viti Levu as cases continue. Image: FBC/Fiji govtFiji covid-19 statistics as at 21 June 2021. Image: FBC/Fiji govt
Red Cross Covid-19 coordinator Lauren Bird, who is based in Suva, said many people felt back in April there was light at the end of the tunnel.
But she said this recent outbreak had reset the clock.
The bulk of cases were in the Suva-Nausori corridor, where about a third of the population is based, Bird said.
Community transmission big concern
“The community transmission is a big concern and this is also happening on the back of Fiji already suffering with the borders closed for the year, people had already lost income of livelihoods.”
RNZ Pacific correspondent Lice Movono, who is in Suva, said the Fijian government was reluctant to go into a national lockdown.
“To explain it very simply, they can’t afford the national lockdown,” she said.
“They’re saying that restricting people from being able to go back to work and re-open businesses means from a public perspective they can’t take their health into their own hands, in terms of being able to put food on the table.”
To respond to the unfolding situation, the New Zealand government signed off an additional support package.
“The assistance includes up to $5 million for the government to deliver covid-19 operations, and $5 million to local civil society organisations working directly with households to mitigate poverty risks, including through the provision of food rations,” said Foreign Affairs Minister Nanaia Mahuta.
New Zealand is sending two medical specialists to join Australia’s medical assistance team (AUSMAT) in Fiji.
Seven days in MIQ
“They will spend some seven days in MIQ and then a 28-day assignment which helps do two things, effectively support the on the ground response, but also undertake a bit of assessment about what else is required,” Mahuta said.
An anaesthetist was part of the six-member Ausmat team that arrived tonight.
Mahuta said a Defence Force infectious disease specialist will be deployed in the near future.
As Fiji grapples with the outbreak, the Health Ministry is continuing its vaccine roll-out, with another 50,000 doses of the AstraZeneca vaccine arriving on Saturday as part of the Australian government’s support of one million doses.
New Zealand has pledged half a million doses, which Mahuta said was expected to arrive from July.
However, Prime Minister Jacinda Ardern noted AstraZeneca was yet to be approved by Medsafe.
“Until they’re approved in New Zealand, we are unable to pass on those doses, so instead we have been working with Australia, who are able to help them with doses sooner into Fiji,” she said.
Fiji now has more than 1500 active cases in isolation since this outbreak in April. Five people have also died since then.
This article is republished under a community partnership agreement with RNZ.
Fiji’s covid-19 cases continue to escalate as medical authorities have recorded another record breaking 166 new people now infected with covid-19 and a death at the Colonial War Memorial (CWM) Hospital in the capital Suva.
The Fiji government has stopped providing information about where the case increases are and the Health Secretary Dr James Fong admitted that community transmission was now “broad”.
The latest death is a 77-year-old man detected by a CWM screening team at his home where he had been bed-ridden for several months.
Despite that he had pre-existing medical conditions, doctors assessing clinical data have attributed the cause of death to covid-19. He represents the seventh to die from the virus, the fifth in this outbreak alone.
Cases in the small township of Lami just outside the capital continues to increase and so measures to ensure safe passage of people from affected containment zones to safe areas on the main island Viti Levu and to other islands is a focus of the government.
“The current priority is therefore to prevent the export of cases into the other non-containment zones. As such any request to move outside of the Central Division to other areas of Viti Levu and from Viti Levu to Vanua Levu and the Maritime zone needs to be strictly regulated,” Dr Fong said.
“Pre-departure swab tests and Quarantine capability are being expanded and strengthened to reduce the risk of spread within and beyond the main island, Viti Levu.”
Dr Fong said the majority of the weekend’s new cases were linked to existing clusters so the government would post heat maps on its digital platforms “to delineate case distribution within the Central and Western divisions.”
He added everyone should practise Covid Safe measures when they left their homes irrespective of where they lived or were going.
Vaccination roll-out continues The Ministry of Health vaccination teams continue to roll out as another 50,000 doses of Astrazeneca arrived in Fiji on Saturday night as part of the Australian Government Support.
Vaccination now moves onto the outer islands of the Northern and Eastern Divisions of the country.
Fiji’s vaccine of choice remains AstraZeneca despite the fact that the Australian government, from which it receives the majority of its supply, has recommended the discontinued use of the vaccine for its under 60-year-olds.
Australian Health Minister Greg Hunt announced earlier this week the AstraZeneca vaccine would be recommended for use in people over 60 and those under 60 would now be offered the Pfizer shot.
The Australian federal government accepted advice from the Australian Technical Advisory Group on Immunisation (ATAGI) after two women died from an extremely rare blood clotting disorder and 60 Australians out of the 3.8 million who got the shot developed blood clots.
Meanwhile the Australian government has provided Fiji with 250,000 Australian-manufactured AstraZeneca vaccines as part of its commitment of 1 million vaccines to its Pacific neighbour.
In response to concerns about Australia’s change of vaccine policy, the World Health Organisation Representative Office in the Pacific and the Ministry of Health Fiji put out a joint statement to say that after vaccinating 256,018 people (44 percent of the adult population) with one dose of AstraZeneca and administering two doses to 17,990 people, there were no confirmed cases of serious adverse effects.
Effective response measure
The WHO/MOH said covid-19 vaccination remains one of Fiji’s most effective response measures.
“Australia’s decision does not change the approach for us here in Fiji. Given the current community transmission and Covid-19 variant, all unvaccinated individuals are at risk from the virus.”
“It is also important to remember that serious adverse events following immunization with the AstraZeneca vaccine remain rare events.”
Further, the WHO continues to recommend Oxford-AstraZeneca vaccines “for individuals aged 18 years and over. These vaccines have undergone the strictest safety and quality control trials and have reached the exacting standards of safety, purity, and effectiveness. Nothing is left to chance,” the statement said.
This article is republished under a community partnership agreement with RNZ.
The Papua New Guinea Council of Churches (PNGCC) has declared its support for the covid-19 vaccination rollout, following a conference in Port Moresby.
Papua New Guinea recorded 72 new covid-19 cases on Thursday, increasing the total number of cases to 16,933 with 173 known deaths.
In a statement, the PNG Council of Churches said: “We pledge our complete support to assist the government of Papua New Guinea and local communities to address community concerns, to work with all partners to ensure that all people are reached and vaccinated consistently.
“We define ourselves as churches, living and working together for the common good of people and society, therefore we affirm our support for the covid-19 vaccination and declare our trust in the safety and efficacy of covid-19 vaccination as a lifesaving tool which protects human from severe sickness and death due to covid-19,” said the PNG Council of Churches in its statement issued on Friday.
“Our affirmation is guided by the theology of ‘Love for Neighbour’ to reach out to others and the ‘theology of liberation’ to reduce the suffering of our neighbours inflicted by the covid-19 pandemic.”
The PNG Council of Churches also said that most of PNG’s health workers, frontline workers, essential workers, people with underlying illnesses and the aged population were not turning up en-masse for vaccination despite being more at risk of dying from the virus.
The churches also noted that much misinformation was being circulated through the social media that was leading to public hesitancy over the vaccine, thereby endangering the lives of millions of people in PNG.
The churches also recognised the negative social and economic impact that covid-19 had caused in PNG, resulting in the loss of lives and livelihood of Papua New Guineans.
A group photograph of the participants of the conference, themed “Am I my brother’s keeper?”, organised by the PNG Council of Churches which comprises seven mainline churches. Image: PNGCC
The church leaders also said that the PNGCC had thoroughly examined the covid-19 vaccination rollout from the Christian theological, cultural, social, academic, medical and political perspectives, and had specifically analysed the doubts and suspicions that were raised.
Solidarity, duty, safety, access and communication Based on this knowledge as well as from the information provided by trusted medical experts, the PNGCC has decided to adopt the five principles of the covid-19 vaccination which are – Solidarity, Duty, Safety, Access and Communication:
Solidarity: The PNGCC strongly affirm global and national call and support for protecting humankind and protecting the people from serious illness and deaths from Covid-19 infection and that these protective measures fully confirm with Christian principles.
Duty: The PNGCC accepts that this is the duty of all persons who are eligible for immunization to join our nationwide ‘Sleeves Up Campaign’ to help stop Covid-19 in PNG to protect themselves and their loved ones from severe sickness and death. It is the duty of the government to provide critical health and social support to uphold the welfare of its citizens.
Safety: The PNGCC acknowledge, based on advice from credible, recognized and reputable medical experts, the safety and effectiveness of all covid-19 vaccines, and that countries with high immunisation rates are beginning to see a decline to almost zero of serious cases and deaths due to covid-19 infection; and that common side effects are not severe and normal.
Access: The PNGCC acknowledges that deadly diseases like Covid-19 can only be controlled and stopped by vaccinating most of the population, especially high-risk groups. It therefore appeals to all responsible departments, agencies and organizations to ensure that full access to covid-19 vaccine is provided to all Papua New Guineans especially the high-risk group in all provinces. The PNGCC calls on local communities and their leaders to work with respected Christian organisations to ensure adequate awareness, access and uptake of covid-19 vaccinations.
Communication: The PNGCC appeals to the media, communities, and key leaders to seek the correct information, and not to spread misinformation and rumours that can cause confusion among our communities and ultimately endanger the lives of millions of people. The PNGCC calls on the media to fully engage the national and international religious leaders and medical experts and institutions to address community concerns about covid-19 vaccinations.
The PNGCC is a Christian ecumenical council in Papua New Guinea, and its members comprise the Anglican Church of PNG, the Gutnius Lutheran Church (affiliated with the Lutheran Church-Missouri Synod), the Union Baptist, the Roman Catholic Church, the Evangelical Lutheran Church of PNG, the United Church in PNG and the Solomon Islands and the Salvation Army.
This article is republished under a community partnership agreement with RNZ.
Fiji’s Health Secretary Dr James Fong confirms that the country has recorded 150 new cases in the 24-hour period ending at 8am June 19 as authorities prepare for deployment of a medical team with specialists from Australia and New Zealand.
One hundred and seventeen cases are from known clusters.
Two cases presented to the Fiji Emergency Medical Assistance Team (FEMAT) field hospital at the Vodafone Arena are under investigation and four cases are under investigation from Totogo police.
Dr Fong said the Colonial War Memorial Hospital (CWMH) cluster had 32 new cases.
“A new cluster has been identified at the Nasese Medical Centre with one new case reported today, adding to the six cases already in this cluster.
Seven cases are primary contacts of other cases – this includes 3 cases from Charles Street in Toorak.
Twenty-three cases are currently under investigation and considered as cases of community transmission.
Death investigations complete
Investigations into the death of a 49-year-old at CWM Hospital reported on Friday are now complete.
The patient’s doctors at the hospital have determined that his death was a result of the severe non-covid-19 pre-existing medical condition that he was receiving treatment for during his admission at the hospital and not covid-19.
Twenty-one more covid-19 patients have recovered, which means there are now 1311 active cases in isolation.
There have been 1728 cases during this outbreak that started in April.
Fiji has recorded a total of 1798 cases since the first case was reported in March 2020.
There have been 473 recoveries and six deaths due to covid-19, with four of the deaths during the outbreak that started in April 2021.
A total of eight covid-19 positive patients have died from pre-existing non-covid-19 related illnesses.
So far 124,264 samples have been tested since this outbreak started in April 2021, with 167,125 tested since testing began in early 2020.
NZ and Australia medics to be deployed to Fiji At the request of Fijian medical authorities, the Australian government has approved the deployment of a medical team to assist the country.
A media statement issued by Australia’s Minister for Foreign Affairs Senator Marise Payne with Minister for Health and Aged Care Greg Hunt and Minister for International Development and the Pacific Senator Zed Seselja, confirmed that the Australian Medical Assistance Team (AUSMAT) would be in Fiji for an initial 28-day period.
Senator Payne did not say how many people would form the AUSMAT team but explained the members were from Australia and New Zealand and from various specialities in medicine.
AUSMAT is similar to Fiji Emergency Medical Assistance Team (FEMAT), which are emergency medical teams globally verified by the World Health Organisation (WHO) as being able to provide a broad range of medical and emergency services in the field in times of crisis.
FEMAT had set up field hospitals in Lautoka, when the city’s hospital was locked down earlier in this current outbreak, and at the Vodafone Arena at Laucala Bay in the capital Suva.
Earlier this week Dr Fong said the Fijian government had requested AUSMAT support with scenario planning.
“We have extra space to deploy for field hospitals and we have extra critical care capacity we have yet to activate. They come to help us plan beyond that,” he said.
Doctors, nurses and paramedics
The Australian version deploys doctors, nurses, paramedics and logisticians to provide medical care in the Asia Pacific region including after Severe Tropical Cyclone Winston in February 2016.
AUSMAT teams are drawn from state and territory health services, but this time includes New Zealand nationals.
“The team will work with the Fijian Ministry of Health and will provide immediate support for health system management and infection prevention control, as well as assessments of Fiji’s priority health needs,” Senator Payne said.
“Australia has also sent 1.3 tonnes of personal protective equipment, medical supplies, including 500 thermal guns for health screening teams, testing equipment and laboratory consumables since the beginning of the current outbreak in April 2021,” she said.
“The health security of our near neighbours is a critical priority for Australia.”
The support is part of the Australian government’s covid-19 support to Fiji worth A$83.5 million for 2021.
Meanwhile, the Asian Development Bank (ADB) and the United Nations Children’s Fund (UNICEF) have supplied more than 1.6 million urgent medical supplies and 9450 diagnostic testing kits to support Fiji in the ongoing detection and containment of the coronavirus disease pandemic.
This article is republished under a community partnership agreement with RNZ.
Dr Fong said 1 case was also identified during screening at Nadi Hospital.
Investigations were underway to determine any links to known cases.
Twenty one cases have been identified as primary contacts of previous cases and are under investigation by the contact tracing teams to determine if there is a cluster link.
Two cases from Naqio settlement, Rewa, 1 case from Nadave, 7 cases from Nausori Village, 4 cases in Naulu, 1 case in Omkar Rd, Narere, 1 case in Valenicina, Lami, 1 case in Verata, Nausori, 1 case from Milverton Road, Raiwaqa, 2 cases from Qauia, Lami, 1 case from Naduru Road, Nausori and 1 case from Fiji Pharmaceutical and Biomedical Services are under investigation to determine if they have links to other cases.
Community transmission
Dr Fong said these cases were currently considered cases of community transmission.
The majority of the cases announced were related to existing clusters of transmission or to localities where significant transmission had occurred.
A 49-year-old man has died at the Colonial War Memorial Hospital (CWMH).
Dr Fong said he had been admitted for almost a month and was being treated for a severe non-COVID pre-existing condition.
He tested positive for covid-19 during his admission, and his doctors are currently investigating to determine if this is a covid-19 death.
Pre-existing illnesses RNZ Pacific reports that to date there have been 6 deaths but another 7 covid-19 positive patients have died of pre-existing illnesses.
There are 1182 active cases in isolation, with Fiji having recorded 1578 cases since the latest outbreak started in April 2021.
Dr Fong said since April, 121,193 samples had been tested, with average daily testing now at 3443.
In terms of vaccinations, “43 oercent of Fijians 18 and older have received their first dose, and 2.1 percent are fully vaccinated. That is a total of 252,791 who have received at least one dose and 12,246 who are fully vaccinated,” he said.
Vijay Narayan is news director of Fiji Village News.
This content originally appeared on Asia Pacific Report and was authored by APR editor.
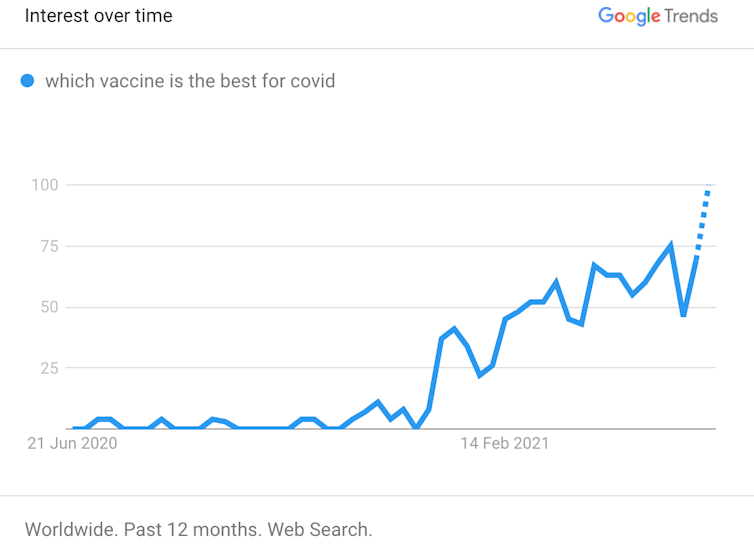
With the rollout of COVID-19 vaccines accelerating, people are increasingly asking which vaccine is best?
Even if we tried to answer this question, defining which vaccine is “best” is not simple.
Does that mean the vaccine better at protecting you from serious disease? The one that protects you from whichever variant is circulating near you? The one that needs fewer booster shots? The one for your age group?
Even if we could define what’s “best”, it’s not as if you get a choice of vaccine. Until a suite of vaccines become available, the vast majority of people around the world will be vaccinated with whichever vaccine is available.
That’s based on available clinical data and health authorities’ recommendations, or by what your doctor advises if you have an underlying medical condition. So the candid answer to which COVID vaccine is “best” is simply the one available to you right now.
Still not convinced? Here’s why it’s so difficult to compare covid vaccines.
Clinical trial results only go so far
You might think clinical trials might provide some answers about which vaccine is “best”, particularly the large phase 3 trials used as the basis of approval by regulatory authorities around the world.
These trials, usually in tens of thousands of people, compare the number of COVID-19 cases in people who get the vaccine, versus those who get a placebo. This gives a measure of efficacy, or how well the vaccine works under the tightly controlled conditions of a clinical trial.
According to Google Trends, more and more people want to know.
And we know the efficacy of different COVID vaccines differ. For instance, we learned from clinical trials that the Pfizer vaccine reported an efficacy of 95% in preventing symptoms, whereas AstraZeneca had an efficacy of 62-90%, depending on the dosing regime.
But direct comparison of phase 3 trials is complex as they take place at different locations and times. This means rates of infection in the community, public health measures and the mix of distinct viral variants can vary. Trial participants can also differ in age, ethnicity and potential underlying medical conditions.
It’s tempting to compare COVID vaccines. But in a pandemic, when vaccines are scarce, that can be dangerous.
We might compare vaccines head to head
One way we can compare vaccine efficacy directly is to run head-to-head studies. These compare outcomes of people receiving one vaccine with those who receive another, in the same trial.
In these trials, how we measure efficacy, the study population and every other factor is the same. So we know any differences in outcomes must be down to differences between the vaccines.
For instance, a head-to-head trial is under way in the UK to compare the AstraZeneca and Valneva vaccines. The phase 3 trial is expected to be completed later this year.
How about out in the real world? Until we wait for the results of head-to-head studies, there’s much we can learn from how vaccines work in the general community, outside clinical trials. Real-world data tells us about vaccine effectiveness (not efficacy).
And the effectiveness of COVID vaccines can be compared in countries that have rolled out different vaccines to the same populations.
For instance, the latest data from the UK show both Pfizer and AstraZeneca vaccines have similar effectiveness. They both reliably prevent COVID-19 symptoms, hospitalisation and death, even after a single dose.
So what at first glance looks “best” according to efficacy results from clinical trials doesn’t always translate to the real world.
What about the future? The covid vaccine you get today is not likely to be your last. As immunity naturally wanes after immunisation, periodic boosters will become necessary to maintain effective protection.
There is now promising data from Spain that mix-and-matching vaccines is safe and can trigger very potent immune responses. So this may be a viable strategy to maintain high vaccine effectiveness over time.
In other words, the “best” vaccine might in fact be a number of different vaccines.
Variant viruses have started to circulate, and while current vaccines show reduced protection against these variants, they still protect.
Companies, including Moderna, are rapidly updating their vaccines to be administered as variant-specific boosters to combat this.
So, while one vaccine might have a greater efficacy in a phase 3 trial, that vaccine might not necessarily be “best” at protecting against future variants of concern circulating near you.
The best vaccine is the one you can get now It is entirely rational to want the “best” vaccine available. But the best vaccine is the one available to you right now because it stops you from catching covid-19, reduces transmission to vulnerable members of our community and substantially reduces your risk of severe disease.
All available vaccines do this job and do it well. From a collective perspective, these benefits are compounded. The more people get vaccinated, the more the community becomes immune (also known as herd immunity), further curtailing the spread of covid-19.
The global pandemic is a highly dynamic situation, with emerging viral variants of concern, uncertain global vaccine supply, patchy governmental action and potential for explosive outbreaks in many regions.
So waiting for the perfect vaccine is an unattainable ambition. Every vaccine delivered is a small but significant step towards global normality.
Anti-vax misinformation is throwing a spanner in the works for covid-19 vaccination programmes in Papua New Guinea and Solomon Islands, with the prime ministers of both countries firing warnings at those spreading it.
PNG Prime Minister James Marape issued a blunt statement this week, saying his government had done everything possible to provide the vaccine during a time of global demand, and that if people did not get themselves vaccinated and then felt sick or died, they only had themselves to blame.
The tally of confirmed cases of vovid-19 in PNG has grown at 16,000 cases in four months, and almost 17,000 people have tested positive for the virus so far. Yet the rate of infections has tapered off from the highs of March.
The government has declared the situation under control, but is anxious to use its supply of AstraZeneca doses before they expire. About 100,000 doses sent through the COVAX programme facility need to be used within a month or they will go to waste.
A little more than 41,000 people in PNG have now had the vaccine, mostly essential workers and about 7000 health workers. But the figures are a drop in the bucket compared to the total population of 9 million people.
Professor Glen Mola, the head of obstetrics and gynaecology at Port Moresby General Hospital, said the government could be more vigorous in quelling misinformation from anti-vaxxers.
“It’s just ridiculous that we spend hundreds of hours out of our precious health worker time countering the ridiculous conspiracy theories of a few people. They spend all their days on social media spreading all this fear,” he said.
“The Controller has powers under the National Pandemic Act, to declare people a threat to public safety… and give them a warning and lock them up if they don’t heed the warning.”
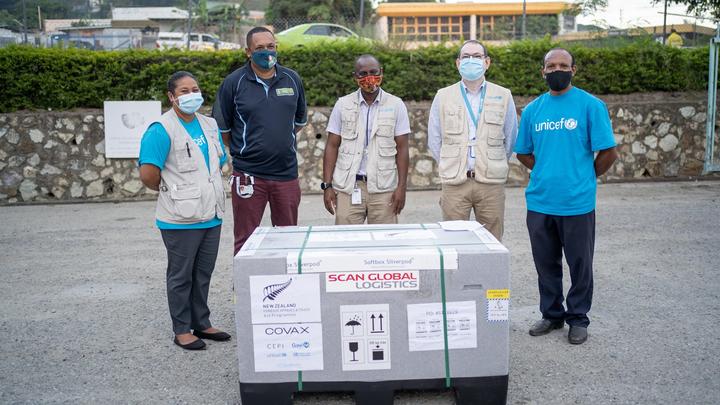
This week 146,000 doses of the AstraZeneca vaccine, bought by the NZ government, were delivered to PNG. Image: RNZ/PNG Department of Health
Hesitancy, social media and antivaxxers Many of PNG’s nurses initially refused to get the vaccine when first offered in late March and early April, asking for clear information about its safety and efficacy.
A Port Moresby nurse (who asked not to be named) this week told RNZ her colleagues had been working their way through the information about the vaccine that had since been made available to them, but she was not yet convinced about it.
“The frontliners are not well informed of all those things, so most of us are still in suspense. But we are just trying to read around and search online, and see for ourselves what it is.”
Professor Mola said his team of doctors had all lined up for the jab, but more work was needed to be put into the campaign to vaccinate as many health workers as possible.
“They’ve had their first shot, and some have had two shots now — that’s the doctors in the maternity side. And we have not had a doctor go down with covid since we started vaccinating.”
One prominent anti-vaxxer in PNG with almost 7000 Facebook followers offers multiple daily commentaries on what she described as a global project to kill and maim millions.
Gladys Habu, a pharmacist and former Miss Solomon Islands, getting her second dose of covid-19. Image: RNZ/Solomon Islands Ministry of Health
The information shared included “terrifying” reports from an alternative UK media source, denigration of organisations which support the vaccine rollout in PNG, and questions such as: “How many times do we have to tell these idiots who have allowed themselves to be injected with poison?”
The official death toll from covid-19 in PNG is 164, but as with the total confirmed cases, the real figure is likely to be much higher, as testing for the virus and reporting of deaths have been limited.
Health workers feature prominently among those in PNG confirmed to have caught the virus so far, and systemic staffing shortages were placing great strain on the workers who continued on the job.
The Port Moresby nurse spoken to by RNZ said she believed there were hospital staff infected with the virus who continued to work in the hospital.
“Maybe they are just trying to normalise the coronavirus like any other diseases,” she said.
Solomon Islands health workers warned In Solomon Islands, Prime Minister Manasseh Sogavare spoke out in a nationwide address criticising a small group of health workers who had promoted misinformation about covid-19 vaccine safety and effectiveness.
He said it was extremely sad that the group had ignored evidence that vaccines were vital to break the cycle of the pandemic, and instead promoted misleading information to the public.
“While I respect individual points of view, I will not allow deliberate misinformation to scare people that wish to protect themselves from covid-19.
“If such deliberate misinformation continues, those involved will be held accountable in accordance with provisions of the relevant regulations.”
Counting on demographics Professor Mola said drily that the upshot was that PNG was relying on the natural protection in a youthful population to mitigate some of the impacts of covid-19.
“Seventy five percent of our population are under 30. And by and large (among) under-30s only one out of 1000 gets seriously ill, and one out of 2000 dies. So we’re going to rely on the protection of youth.”
PNG Health Minister Jelta Wong said officials were doing what they could to vaccinate the priority groups, and while there were ongoing “issues” with reaching all healthworkers, the vaccinations were now been extended to the elderly.
Six infants who tested positive to covid-19 are in stable condition at Lautoka Hospital in the west of Fiji.
Health Secretary Dr James Fong confirmed this to The Fiji Times this week. The infants and their mothers were from a community in lockdown in Nadi.
They were recently assisted with basic supplies by the Foundation of the Rural Integrated Enterprises and Development (FRIEND). A post on the FRIEND Fiji official social media page said they responded to a request for assistance from the community in lockdown in Nadi.
FRIEND Fiji then facilitated the request after a donor purchased baby essential packs.
The packages were delivered to the mothers in need last Thursday.
“We pray for the speedy recovery of infants and their mothers,” FRIEND Fiji said in a recent Facebook post.
“Please keep them in your prayers.”
Mothers, babies transferred
Meanwhile, Dr Fong also confirmed that some mothers and babies from the Colonial War Memorial Hospital’s (CWMH) Neo-Natal Intensive Care Unit in Suva had been transferred to Lautoka Hospital because of escalating covid-19 cases at the CWMH.
While he could not confirm the numbers, he said, however, that the ministry had activated that contingency protocol.
RNZ Pacific reports there have been 121 new covid-19 cases confirmed in Fiji as health officials identify two new clusters.
The total number since the outbreak started in April is now 1373.
Dr Fong said a new cluster had been identified within the Rewa Emergency Operations Centre, possibly linked to the Vunimono cluster.
A new cluster is also at the Town House Hotel in Suva where Colonial War Memorial (CWM) Hospital and Incident Management Team (IMT) staff are being accommodated.
Two key issues
In an editorial about lockdowns and sticking to the covid rules, The Fiji Times stressed that two issues stood out in the face of the announcement of new covid-19 cases.
While there was great importance placed on the announcement of the daily figures, other issues had also been raised on different platforms, the Times said.
“For instance, the Head of Health Protection, Dr Aaalisha Sahukhan, said lockdowns [had] not contained the spread of covid-19 in the Lami-Suva area,” the newspaper said.
While it was an important tool, Dr Sahukhan had pointed out, it had had a socio-economic impact on the population.
She had shared her view during a webinar on covid-19 organised by the Fiji National University.
“We’re coming to a point now where from the health perspective, yes lockdowns are an important tool, but also we have come to a limit of applying those lockdowns because of the impact on the community,” Dr Sahukhan said.
The capital had gone through periods of extreme lockdowns “which we call curfew lockdowns [lasting] as long as four days.
“Unfortunately, even this level of lockdowns and our containment efforts has not contained the effect within the Lami-Suva area.”
Ten people have died in Fiji after testing positive for covid-19 — but only four had their deaths attributed to the coronavirus.
The Health Ministry said six other patients had died from existing chronic conditions they had while being admitted at the country’s main hospital in Suva.
This has raised some concern among Fijians who are calling for an explanation over what constitutes a covid-19 death.
Health Secretary Dr James Fong said the four patients had since died with illnesses directly related to their covid-positive status.
Six patients died at the Colonial War Memorial Hospital (CWMH) since an outbreak at the facility was announced on June 1.
Of the 860 covid cases currently in isolation, more than 150 have been from the CWMH.
Dr Fong said each of the non-covid deaths were due to other serious medical conditions which the patients had been admitted to hospital for.
Covid-19 infection ‘incidental’
The finding of a covid-19 infection was incidental, he said.
On June 8 however, Dr Fong announced the death of a man who had tested positive for the virus upon his admission at the hospital.
But he said the doctors “determined that he died due to complications of his chronic medical condition”.
The inconsistency has led to public confusion and given rise to conspiracy theories as people took to social media to raise their concerns.
Many are calling for an explanation over what constitutes a covid-19 death.
The World Health Organisation (WHO) classifies a death due to covid-19 as one that is “resulting from a clinically compatible illness, in a probable or confirmed covid-19 case, unless there is a clear alternative cause of death that cannot be related to the covid disease (e.g. trauma).
There should be no period of complete recovery from the virus between illness and death, the WHO said.
Comparative definition
“A death due to covid-19 may not be attributed to another disease (e.g. cancer) and should be counted independently of pre-existing conditions that are suspected of triggering a severe course of covid-19.”
By comparison, Public Health England changed its definition of covid deaths in August 2020 as being anyone with a “laboratory-confirmed positive covid-19 test and died within (equal to or less than) 28 days of the first positive specimen date will now be reported.”
Fiji health officials Dr Aalisha SahuKhan (left) and Dr James Fong. Image: RNZ/Facebook/Fiji govt
Fiji’s Head of Health Protection and the person in charge of covid-19 testing in the country, Dr Aalisha SahuKhan, confirmed Fiji’s case count per day was now higher than both Australia and New Zealand.
“So we are now at about 60 cases per day, which is if you’re looking at our population, that’s about 68 per million population, which is a high number. To put that in context, neither Australia nor New Zealand got to this level of cases per day.”
Dr SahuKhan said authorities had also noticed that despite the high number of cases per day, there has not been a corresponding increase in severe cases and deaths yet.
“I’m saying yet, because what we do expect from what we see around the world is that we will see that wave come in,” she said.
“So far during this outbreak, we have reported two deaths that we’ve attributed to covid-19.
“So as everyone in Fiji knows that our largest hospital, the CWM Hospital has been affected by this virus, we’ve had an outbreak there.
“Unfortunately, the first wards that covid-19 hit were the acute medical wards. So these were where the people were managed.
Long standing chronic conditions
“They are already very sick, they have long standing chronic conditions that they were admitted for and because there was an outbreak in the hospital, they also tested positive for covid.”
Dr SahuKhan said Fiji’s testing capabilities, enhanced with donations of equipment from Australia, New Zealand and the European Union had made it possible for them to track the alarming increase of the current outbreak.
“Our test positivity per day, looking at over an average of seven days, is a better measure to see what the trend is.
“So we started very low, it was about 0.2 percent of our all our tests per day were testing positive, and now we’ve come up to 2 percent which is high. The thresholds we’re using is a WHO-base threshold.”
Dr SahuKhan said that while high test positivity per day in a country could mean that authorities are not testing enough or testing only in high risk communities, Fijian authorities are confident their testing samples are an accurate illustration of the situation in Fiji.
“We have a very broad category, a spectrum of testing, and we’re still seeing that test positivity is increasing. So that indicates that we are seeing increasing cases of community transmission, but we’re still keeping up that high level of testing,” she said.
Fiji now has over 1100 covid-19 cases since April, including 89 new cases confirmed last night.
This article is republished under a community partnership agreement with RNZ.
Papua New Guinea’s Prime Minister James Marape is appealing to people to take the covid-19 vaccine before doses expire.
This comes as the number of covid cases in PNG has climbed by around 1000 a week since February.
A little over 40,000 people in PNG have received their first dose of the AstraZeneca vaccine. Of this number, 6500 are health workers, the rest are essential workers and a small number of people with co-morbidities.
But PNG authorities are grappling with vaccine hesitancy, and are anxious to use up tens of thousands more Astrazeneca doses before they expire.
The prime minister, who was the first in PNG to take the jab back in March, has appealed to people to take the vaccine that was made available despite a global shortage.
Marape, who took his second dose of Astrazeneca last week, has moved to dispel rumours about the vaccine, saying it was safe and represented the best opportunity for people to protect themselves against the virus.
He told local media that he had not experienced any form of side effects from the first dose and that now, with the second dose, he was on the path to acquiring 80 percent immunity against covid-19 after 40 days.
100,000 doses in storage
But even with the government’s vaccination awareness campaign, more than 100,000 doses remain in storage and in danger of going to waste.
Many of the doses, made available to PNG through the Covax facility, are due to expire in either mid or late July.
Marape said his government was doing everything possible to have the vaccine available and that if people did not get themselves vaccinated and then felt sick and maybe died, then they only had themselves to blame.
With the government opting not to make vaccination compulsory, the prime minister emphasised that it was a choice that citizens had to make.
He said PNG was lucky to have access to vaccines earlier this year, thanks to partners such as the World Health Organisation, the Covax facility and the Australian government.
Meanwhile, PNG’s Pandemic Response Controller reported 40 new covid-19 cases yesterday, increasing the country’s total cases to 16,682 while the death toll is 164.
To date, more than 126,000 people have been tested for the virus in a population of almost 9 million. All 22 provinces including the Autonomous Region of Bougainville have reported cases.
This article is republished under a community partnership agreement with RNZ.
Fiji’s Health Ministry has announced 105 new covid-19 cases as the pandemic crisis worsens.
Health Secretary Dr James Fong said 98 of the cases recorded yesterday were linked to existing clusters, while links to seven more cases were still under investigation.
He said new cases recorded at Grantham Rd and Tacirua were under investigation to determine whether they had links to other cases.
He confirmed two patients admitted at the Colonial War Memorial Hospital (CWMH) for pre-existing severe illnesses had died.
“With the ongoing outbreak at the hospital, both patients tested positive for covid-19 during their admission,” he said.
“However, their doctors have determined that their causes of death are related to the pre-existing illnesses for which they were admitted and receiving treatment for at the hospital.
“These are not covid-19 caused deaths.”
Review of cases
Meanwhile, a review of cases from Nadi found that one case tested positive twice.
Fiji has recorded 1048 cases since the outbreak in April this year, with eight recoveries.
There are now 796 active cases in isolation.
Fiji has recorded a total of 1118 cases since the first case was reported in March, 2020.
There have been 312 recoveries and 4 deaths because of covid-19 and a total of 6 COVID-19 positive patients have died from pre-existing non-covid-19 related illnesses.
The leader of Fiji’s opposition National Federation Party has condemned the government’s strategy for dealing with the coronavirus pandemic as having “failed” and warns it will lead to “catastrophic results”.
“The government plan is complacent and short-sighted,” said Professor Biman Prasad in a statement tonight in response to the “ominous total” of 1000 covid-19 cases, 700 of them currently active.
“The government thinks that the situation Fiji is facing now will stay the same. It is not planning for things to get worse.
“Yet every lesson, from every country in the world, should tell it otherwise.”
Dr Prasad’s statement followed a claim by Prime Minister Voreqe Bainimarama yesterday that Fiji could not afford a lockdown, reports The Fiji Times.
The prime minister has shut out calls for a complete 28-day lockdown of Viti Levu, saying that would spell “economic disaster and miserable isolation”.
“And I cannot allow that to happen. I will not,” Bainimarama said.
‘Disaster without a lockdown’
Dr Prasad said: “The opposite is true. There will be health, economic and social disaster without a lockdown.”
The government believed in its containment strategy, he said.
“It could not keep the virus in the Suva-Nausori containment area when the numbers were low. The virus still escaped to the West. It is now multiplying there.
“If the containment strategy is working, how did the virus come to Naitasiri?
“Now, with more than 700 cases, the government’s strategy is to hope and pray that nothing else will go wrong. But even in well-run operations, things go wrong. And then what will the government do?
Dr Prasad said Fiji was now putting lives at risk.
“Most importantly the lives and health of our frontliners – doctors, nurses, health workers – is at risk,”he said.
‘Limited trained staff’
“We have only a limited number of trained health staff who can manage this crisis. What happens when they are taken out of action?
“Right now my greatest fear is for these people, who have been working long hours, at ever greater risk to themselves, to execute a politicians’ plan they do not believe in. Why isn’t the government thinking of them and listening to them?
Every day we delay a lockdown, we simply prolong the crisis. We know the coronavirus kills people. We now know that for many who survive, their long-term health is permanently damaged.”
If the government continued to be stubborn and blind, “we will end up in a crisis we can no longer handle by ourselves”.
“Australia and New Zealand will be forced to intervene to save Fiji from a health crisis that has become too big for it.
“And how many lives would have been lost by then, all because of the stubbornness and arrogance of this government?”
Yogendra Reddy raises his concerns at the Nawaka Tramline settlement lockdown checkpoint in Nadi. Image: Reinal Chand/Fiji Times
A plea for food protest in Nadi The Fiji Times reports that residents currently on lockdown in a few settlements located beside Nawaka, Nadi, had taken to the streets yesterday to voice their frustration and their need for basic food items and groceries.
Police officers from Nadi stepped in to control the situation and reminded people their act was unlawful.
Food rations from the government arrived a few hours after the protest was staged by the concerned residents.
Meanwhile, in a virtual conference on covid-19, heads of political parties have called on the government to pull its resources together to ensure people in lockdown areas are being assisted.
UN help sought amid covid, climate crises RNZ Pacific reports that Fiji has called on the United Nations to use its convening power to align affordable, accessible and efficient development finance to help the government address the covid-19 crisis and climate emergency in the country.
Attorney-General Aiyaz Sayed-Khaiyum made the plea during a virtual meeting with the UN Assistant Secretary-General, UN Development Programme (UNDP) assistant administrator and director of the UNDP Regional Bureau for Asia-Pacific, Kanni Wignaraja last week.
During the discussion, Sayed-Khaiyum highlighted Fiji’s response to covid-19 and potential areas of support that the UNDP could provide to enable swift and inclusive post-covid recovery.
He said Fiji intended to encourage public-private investments in economic diversification by creating a sustainable ‘blue economy’.
A disaster is unfolding in Fiji as covid-19 cases continue to escalate – 94 cases in the last 24 hours, the highest recorded daily number to date.
That is the highest ever daily total for the country, and health experts have told 1 NEWS the country is on the brink of losing control.
A Fiji government media statement released late Tuesday night shows a medical system under stress and unable to cope with the dramatic rise in numbers.
Suva’s emergency field hospital set up at Vodafone Arena with the main hospital having become a “closed” covid-19 pandemic institution. Image: APR screenshot TVNZ
It says due to the high number of those testing positive with covid-19 and constraints on quarantine capacity, all new positive cases will be isolated at home where feasible.
But in the Lami-Nausori containment zone a serious crisis is emerging where all resources will be solely directed at those seriously ill with covid-19.
“We are preparing to shift into a mitigation phase that ensures that healthcare resources are focussed on caring for patients who develop severe illness as a result of the virus,” the statement read.
Suva’s main Colonial War Memorial Hospital (CWMH), now closed because of a raft of cases from there, is now being used as a covid-19 care facility.
The Valelevu Health Centre also closed this afternoon after two patients recently discharged from hospital went there to be tested and returned positive results.
So far there have been three covid-19 related deaths in the last few day, but authorities are refusing to count them as such, stating that they died of complications from underlying conditions.
Health Secretary Dr James Fong said the rest of the cases were linked to existing clusters: Colonial War Memorial Hospital (CWMH) – 6; Nawaka, Nadi – 35; Vunimono – 2; the government’s Covid-19 Incident Management Team (IMT) – 4 and Waila – 1.
Dr Fong said another case was a primary contact of an active case, and the connection to a cluster was being determined by the contact tracing teams.
He said the two unknown cases were from Raiwai in Suva, and Nakasi in Nausori.
Dr Fong also announced the death of an individual who was admitted at the Colonial War Memorial Hospital and then tested positive for covid-19.
Medical complications
He said the patient’s doctors had determined that he had died because of complications of the serious medical condition that led him to his admission in hospital.
“The ministry expresses our condolences to his family,” Dr Fong said.
Thirty nine cases were reported on Thursday, and Dr Fong said the outbreak remained primarily centred in the Lami-Suva-Nausori Containment Zone.
He said 22 patients had recovered with 684 active cases in isolation while 900 cases were recorded during the current outbreak that started two months ago.
There have been 970 cases recorded in Fiji since the first case was confirmed in March 2020, with 278 recoveries and four deaths.
Four other covid-19 positive patients have died from pre-existing illnesses and are non-related to the virus.
This article is republished under a community partnership agreement with RNZ.
Five police officers are among 39 new cases of covid-19 in Fiji while the government announced late last night that 32 of the latest cases are from existing clusters.
Another 11 cases were reported from the country’s main hospital in the capital Suva.
Health Secretary Dr James Fong said the ministry’s mitigation strategy was to isolate cases, treat seriously-ill patients and ensure the success of its vaccination rollout programme.
But he said they were concerned that Lami and the police barracks in Nasinu, both clusters outside Suva, may see increasing numbers of cases.
Teams are tracing and testing known contacts and are isolating positive patients to prevent further spread of the virus, Dr Fong said.
“In the near-term, we are concerned that Lami may see increasing numbers of cases.
“We also anticipate more cases from the cluster at the Police Barracks in Nasinu.
“Our stationary and mobile screening teams are tracing and testing known contacts and are isolating positive patients to prevent further spread of the virus.”
Police tried their best
Acting Police Commissioner Rusiate Tudravu told local media the force had tried its best to prevent the spread of the virus among its officers.
Initially three officers from the Nasinu Police Station had tested positive for the virus and another 15 were swabbed earlier in the day.
Neither Tudravu nor Dr Fong provided information on how the officers were infected.
“I’m not surprised because we are classified as high mobile risk because of our job, it requests us to be on the front line,” Tudravu said.
“Having said that, we have tried our best not to have anyone in the force to have the virus.
“We are there in the front line and we are vulnerable to that.”
The infected police officers are on home isolation and monitored by the Ministry of Health and guarded by police officers, Tudravu added.
Latest cases
The other latest cases included six from Nawaka, Nadi; three from the warehouses of the Fiji Independent Commission Against Corruption-FICAC, two from the Republic of Fiji Military Forces Naval Division, two from Waila in Nausori, one from Naitasiri, one from Caubati outside Suva and another case from the Covid-19 Incident Management Team at the Health Ministry’s headquarters in Suva.
The ministry is yet to determine the source of infection for seven other cases — four from Lami Town, one from Toorak a suburb adjacent to the central business district of Suva, one from Nasinu Town and one from Reservoir Road near the city.
Meanwhile, the government’s vaccination rollout programme continues with 228,030 people having already received at least one dose of the AstraZeneca vaccine.
Officials reported 50,000 doses of the vaccine had arrived in the country from Australia this week.
“The vaccine administration in Nadi had been temporarily halted due to a case among the administration teams,” Dr Fong said.
“Relevant personnel have since been cleared and vaccine administration in Nadi has resumed.”
Seven patients had recovered and there were now 656 active cases in Fiji.
There have been 849 cases since this outbreak began two months ago and 919 cases since March 2020.
This article is republished under a community partnership agreement with RNZ.
Fiji police man checkpoints into Suva … infected police officers are on home isolation and monitored by the Ministry of Health, and guarded by police officers. Image: Fiji Police/RNZ
This content originally appeared on Asia Pacific Report and was authored by APR editor.
The Papua New Guinean government should protect women accused of practicing “sorcery” from violence and hold the attackers to account, says the advocacy group Human Rights Watch.
At least five women have been attacked in the past three months since March 2021 — one of whom was killed.
“The Papua New Guinea government should urgently investigate all cases of violence following sorcery accusations, and prosecute those responsible,” Stephanie McLennan, senior manager of Asia initiatives at Human Rights Watch, said in a statement today.
“Gender-based violence is a persistent problem in Papua New Guinea, and the government is doing very little to stop it.”
Violence following allegations of sorcery is common in Papua New Guinea, with the most recent reported case on May 7 in Hela Province.
Mary Kopari was accused of sorcery following the death of a young boy in her village. She was tied up and burned alive in Komo-Magarima District.
The attack was recorded on video and reported by Papua New Guinea television. Although the police know the identity of some of the attackers, no arrests have yet been reported.
Surge in covid cases
Because sorcery accusations often arise in response to an unexpected death or illness in a community, the increase in such violence may be related to a surge in confirmed cases of covid-19 in Papua New Guinea.
On or around March 30, in Goroka, Eastern Highlands, a 45-year-old woman and her 19-year-old daughter were accused of causing the woman’s husband’s death, believed to be from covid-19.
They were held captive by the husband’s relatives and tortured with hot iron rods. Police rescued the pair.
On April 25, police rescued two women after a group of about 20 men tortured them in Port Moresby. The men accused the women of practising sorcery and killing a woman who had recently died.
The women were treated for severe burns and knife wounds.
“The Papua New Guinea government should address the root causes of sorcery accusations, including the lack of basic knowledge among the public about health problems,” McLennan said.
“The authorities should act swiftly and effectively to correct misinformation about deaths from covid-19 to prevent more sorcery accusations and attacks.”
Most attacks target women
While there are past cases of violence based on accusations of sorcery targeting men, the majority of these attacks target women. Such attacks are part of the larger problem of high rates of gender-based violence and impunity for the abusers in Papua New Guinea.
A larger problem of high rates of gender-based violence and impunity for the abusers in papua New Guinea. Image: PNG Report
In November 2020 a coalition of Parliament members convened the country’s first national summit on gender-based violence. A special parliamentary committee on the issue held its first hearings on May 24 and 25, and will continue its inquiry until June 30.
Dr Fiona Hukula, gender specialist for the Pacific Islands Forum, testified at the May hearings about violence against women accused of sorcery, saying that they are are “often tortured, often cut, sexually violated, their clothes are removed and they are often kept in captivity”.
As Human Rights Watch has documented, greater resources and increased political will are needed to respond to all forms of gender-based violence in Papua New Guinea. At the recent parliamentary hearings, East Sepik Governor Allan Bird said “there are 1.4 million cases of GBV [gender-based violence] every year in PNG … and only 100 convictions achieved”.
Papua New Guinea will participate in November in the UN Human Rights Council’s Universal Periodic Review process under which member countries review the human rights situation in the country.
The Human Rights Watch submission for that process highlighted the issue of gender-based violence and violence following accusations of sorcery.
“Papua New Guinea’s leaders should order the police to take gender-based violence seriously, provide sufficient resources for officials to prosecute these crimes, and provide all survivors with medical treatment, shelter and access to support services,” McLennan said.
“The parliamentary inquiry should lead the way in exploring options for early warning, protection, and dispute resolution mechanisms that can help prevent such crimes.
“If our frontline workers stayed home, there would be no response to this outbreak. And there would be nobody left to care for sick patients whether they have covid or not. They protect themselves as best as they can.”
Dr Sahukhan said some of the staff from the Incident Management Team (IMT) had been impacted on by the virus recently.
“This concern is understandable and I know what you’re thinking. How are they getting infected?
“Aren’t they following the advice that they are giving us? First of all, covid-19 is a highly transmissible and contagious virus. It spreads very easily in crowded spaces.”
Dr Aalisha Sahukhan said the frontline healthcare workers were swabbed twice a week because of the nature of the work they did.
She said most of them have not seen their families for weeks as they pushed on with their groundwork in testing and swabbing Fijians.
Health authorities reported 35 new cases of covid-19 yesterday for a total of 880 and four deaths since the virus first impacted on Fiji.
A new daily record of covid-19 cases has been announced in Fiji as 94 new cases in 24 hours have been confirmed.
The Fiji government is now unable to isolate cases at its facilities, sending positive people home instead.
It has announced it was preparing to focus on caring for severely ill patients as opposed to its current strategy. It had hinted at this scenario early in this outbreak in the event the public health system would become overburdened.
Dr Fong, himself a primary contact of a colleague in the government’s Covid-19 Incident Management Team (IMT) who tested positive, said the majority of new cases was from transmission in closed indoor spaces.
Nine more members of the IMT have since tested positive too.
“Due to the high number of cases and constraints on quarantine capacity, new positive cases are being entered into home isolation, where feasible. Specific guidance has been provided for these individuals to ensure they do not have contact with other members of their households,” Dr Fong said.
“It is vital — particularly in multi-generational households — that the ministry’s home isolation protocols are strictly followed. While we will be regularly checking up on these individuals, adherence to our home isolation protocols within the household is critical at all times,” he said.
Shifting to mitigation
“Given the escalating numbers of new cases in the Lami-Nausori Containment zone, we are preparing to shift into a mitigation phase that ensures that healthcare resources are focused on caring for patients who develop severe illness as a result of the virus, to ensure that they can receive proper treatment and achieve the best possible outcome from the care.”
Fiji’s Health Secretary Dr James Fong … “new positive cases are being entered into home isolation, where feasible.” Image: Fiji govt/RNZ
Dr Fong, himself a primary contact of a colleague in the government’s Covid-19 Incident Management Team (IMT) who tested positive, said the majority of new cases was from transmission in closed indoor spaces.
Nine more members of the IMT have since tested positive too.
“Due to the high number of cases and constraints on quarantine capacity, new positive cases are being entered into home isolation, where feasible. Specific guidance has been provided for these individuals to ensure they do not have contact with other members of their households,” Dr Fong said.
“It is vital – particularly in multi-generational households – that the ministry’s home isolation protocols are strictly followed. While we will be regularly checking up on these individuals, adherence to our home isolation protocols within the household is critical at all times,” he said.
“Given the escalating numbers of new cases in the Lami-Nausori Containment zone, we are preparing to shift into a mitigation phase that ensures that healthcare resources are focused on caring for patients who develop severe illness as a result of the virus, to ensure that they can receive proper treatment and achieve the best possible outcome from the care.”
Meanwhile, 28 of the new cases alone are from the capital Suva’s Colonial War Memorial Hospital (CWMH), which is now a dedicated covid-19 care facility.
The other new cases include 26 from Waila near Nausori town, 14 from Navosai in Nasinu Town, eight from Nawaka in Nadi, five from the Republic of Fiji Military Forces Naval division and three from its army base and one case is from Caubati just outside the capital city.
Third hospital death
Dr Fong reported the death of a patient at the CWMH in Suva but said that although the person had tested positive for covid-19, his death was not ruled the result of the virus.
This is the third such death from the country’s main hospital in less than a week.
“This individual was admitted in the CWM Hospital’s Acute Medical Ward and died Tuesday morning as a result of the medical condition for which he was initially admitted,” he said.
“While the individual did test positive for covid-19 during his admission at the hospital, we have not classified this as a covid death based on the assessment of his doctors, who have determined that he died due to complications of his chronic medical condition,” he said.
The CWMH cluster which has been the fastest growing transmission since it was discovered a week ago now continues to concern authorities as people recently discharged from the facility turn up positive cases in other districts.
This included two patients who were detected at the Valelevu Health Centre in Nasinu, the largest municipality in the country. That facility, an important part of the government’s infrastructure, is now temporarily closed for decontamination.
Four patients have recovered taking the total number of active cases to 604. There have been 775 cases since April 2021. Since the pandemic began in Fiji, there have been 845 cases and 234 recoveries and four deaths.
“Members of the public should avoid any situation that puts them into close quarters with others outside of their household or home bubble,” Dr Fong said.
“If you see a crowding situation, avoid it at all costs. Do not add to the problem. Even when you are masked, entering into close quarters with others can place you at grave risk.”
This article is republished under a community partnership agreement with RNZ.
New Zealand’s leading daily newspaper has warned the country against complacency over the covid-19 pandemic and to look to Fiji for an example of how things can easily go wrong.
In an editorial today, The New Zealand Herald has also criticised the government over its communication strategy and failure to counter a disinformation campaign threatening the national vaccination rollout.
“Complacency is our greatest enemy, particularly while the director-general of health continues to report no community transmissions in his regular briefings and with just 5 percent of the population having received a second vaccine shot,” said the Herald.
“Fiji has discovered geographical isolation is not enough to avoid the increased transmissible variants of covid. Vigilance and adherence to official advice remains crucial as the best mechanism we have to the defeating this damned thing.
“Raising our prevention and contact tracing game after it has arrived is too late.”
From early on in the covid-19 pandemic, it was obvious that consistent communication was essential for New Zealanders to maintain compliance with key measures to limit transmission of the virus, said the newspaper.
“Now we know ‘influencers’ were deployed in Auckland’s March [2020] lockdown to push messages into social media as the government fretted about online posts undermining the pandemic response,” the Herald said.
Jeopardising NZ’s response
“It appears it was thought overly harsh critics condemning infected people for not self-isolating could truly jeopardise the country’s response. A newly released Cabinet paper said ‘social licence’ was crucial to a strong covid-19 response.
“Such hostility could undermine the overall pandemic response, wrote covid-19 Response Minister Chris Hipkins. ‘Public reaction to particular individuals who have not used the covid-19 Tracer app or otherwise failed to follow good practices suggests a possible erosion of this.’
“So, the Government sought help from social media figures who were deemed to have sway in Māori, Pacific, Indian and youth communities. Hosts from radio stations Tarana, Flava, The Edge and Hauraki subsequently posted reassuring photos and messages, using the campaign’s hashtag #stayinforit.
“Contrast this social media influencing tactic with the lack of action around countering misinformation on the vaccine.
“Most will have by now seen or heard of the leaflets put in mailboxes in a concerted campaign to raise unfounded fears about the vaccine and undermine the protection offered by mass immunity.
“The flyer was produced and distributed by a group called Voices for Freedom. Co-founder Claire Deeks ran as a candidate for Advance New Zealand at the last election, and was third on the party list.
“The group claimed to be putting out two million flyers to coincide with the government’s vaccine campaign.”
Information investigation
The Herald noted how investigative journalist David Fisher had sought any communications about what government agencies might do to address the false claims being disseminated about the vaccine and was told “the information does not exist”.
“For all its efforts and expense, Voices for Freedom failed to register as a threat.”
The government itself had not always been clear in all its communications, with some “casual contacts” of positive cases being upgraded to “casual plus” without announcement or explanation in March this year, the newspaper said.
“The Prime Minister was also accused of neglecting her own advice to ‘be kind’ when she publicly criticised a covid-infected person who continued to work at a KFC store.
“Ultimately, the government is well aware the greatest risk is the public passively drifting off the necessary precautions rather than active resistance.”
Calls for more action from the Fiji government are growing louder, as authorities appear to be losing their grip on a rapidly-growing outbreak of the covid-19 pandemic in the country.
Authorities have confirmed 147 cases in the last two days alone, and the country’s main hospital has been effectively sealed off, with Suva’s emergency department now operating from a field hospital at a stadium.
New Zealand Prime Minister Jacinda Ardern has called the situation in Fiji concerning, while health authorities there say the “serious developments” are impacting on their ability to respond.
Opposition and civil society groups say the escalating number of covid-19 cases are a clear indication the government is not in control of the crisis.
Despite calls for a lockdown, Prime Minister Voreqe Bainimarama has said there is no need to declare a state of emergency.
But the National Federation Party’s Professor Biman Prasad said the government must act now to avoid a disaster.
“This is a government that has lost the ability to think straight and it appears that it’s totally stranded,” he said. “Everyone must put out a proper strategy.”
Criticism becoming louder
Across the country, criticism of the government response is becoming louder, with political opponents charging that the government lacks a clear plan.
As the country’s covid situation has spiralled increasingly out of control, Fiji’s PR-savvy political leaders, who rarely shy away from a camera opportunity, have gone increasingly quiet.
“In the middle of Fiji’s biggest health crisis since independence, its minister-for-everything finds time to talk about local government reform, attack USP, lawyers, accountants and the NGOs,” Dr Prasad said.
“When numbers got out of control, the Prime Minister issued a rambling speech about Moses and the Israelites.”
The latest outbreak started when a soldier working at a mandatory isolation quarantine facility contracted the virus from a couple who had returned from abroad.
Now, there are more than 500 active cases across the country, with clusters at the Colonial War Memorial Hospital in Suva, the navy and military, a Suva supermarket, several villages and, now, the country’s main covid management team at the Ministry of Health, which has forced senior health leaders, including Health Secretary James Fong, into isolation.
And on Tuesday, the entire parliamentary complex in Suva was shut down after a staff member was identified as a primary contact of someone who had tested positive with the virus.
Precautionary measure
Speaker Ratu Epeli Nailatikau said that as a precautionary measure the parliamentary precincts would be closed until further notice.
“Our hospitals and even the health ministry headquarters have not been spared from its onslaught. This is largely due to lack of a coherent strategy to fight the pandemic,” said former prime minister Mahendra Chaudhry, who leads the Fiji Labour Party, which is not in Parliament.
There are growing calls — particularly from some NGOs — for a sustained nationwide lockdown in Fiji to stamp out cases, something which authorities say would be incredibly difficult to pull off in Fiji.
On Sunday, while warning that high numbers could be expected for a while yet, Dr Fong said in a written statement that more stringent measures were not needed.
“Thanks to the massive step-up in the pace of our testing, we can continue to fight this virus in a targeted way,” Dr Fong said.
“A way that allows Fijians to access essential services and allows the economy to function as normally and safely as possible.”
Health Minister Ifereimi Waqainabete also said there was no need to get too alarmed at the current numbers, adding that most were coming from identified clusters.
Coming from clusters
“What we must be looking at is the numbers in which they are coming from,” he said.
“As long as they are coming from within the clusters and as long as we are not getting many new community cases, then we know that the programmes that are in place are working.”
New Zealand’s Foreign Minister, Nanaia Mahuta, said her officials were in close contact with counterparts in Fiji about what help could be offered.
“It is concerning, and we are vigilant in terms of keeping in contact with Fiji and responding to their needs as they arise,” she said.
“However, Fiji is tasked with responding to an issue which we’ve all had to, and we’ve given our commitment in terms of PPE, e-gear support and also some financing.”
Mahuta added that a donation of 500,000 doses of covid vaccine was still on track to arrive in Fiji in July.
This week, Australia will send an additional 50,000 doses of the AstraZeneca vaccine to Fiji.
Fiji has had 751 covid-19 cases since March 2020, with 515 active cases and four deaths reported.
This article is republished under a community partnership agreement with RNZ.
This content originally appeared on Asia Pacific Report and was authored by APR editor.
Fiji recorded 83 cases of covid-19 on yesterday — its highest daily figure yet, as authorities moved to cordon off the country’s largest hospital and quarantine an entire village as it battles to bring a rapidly growing outbreak under control.
Health Secretary James Fong said 11 of the cases were of unknown origin and were being treated as cases of community transmission until proven otherwise.
Dr Fong also announced that the country’s largest hospital, the Colonial War Memorial Hospital in Suva, would be sealed off from the community and become a full-time covid care facility, with tightly controlled movement.
“Access to laboratory, maternity and paediatric units will be through escalated screening protocols and package decontamination protocols,” he said in a written statement late last night.
An additional field hospital to treat non-covid patients will be set up in the hospital’s vicinity with support from Australia, Dr Fong said.
The entire village of Mulomulo, in Nadi, has also been locked down after contact tracing investigators found more than 100 people had attended a funeral, which Dr Fong said could become a super-spreader event.
Currently, funerals are restricted to no more than 10 people.
New clusters have also been confirmed in Naitasiri, to the north of Suva, including one patient who was recently discharged from the Colonial War Memorial Hospital.
“The high number of cases confirmed today signals a much larger proportion of cases in the community,” Dr Fong said. “We expect more days of high numbers of confirmed cases.
“We sadly expect more hospitalisations as more severe cases of the disease develop.”
Health Secretary Dr James Fong … “We expect more days of high numbers of confirmed cases.” Image: RNZ/Fiji govt
More than 2700 tests were carried out on Saturday, the government said, with a seven day average of 2819. Dr Fong said this was one of the highest rates in Oceania.
But with the country also contending with one of Oceania’s worst outbreaks of the coronavirus – more than 600 cases have been recorded since the latest outbreak began in April – the government has insisted that more stringent lockdown measures are not needed.
“Thanks to the massive step-up in the pace of our testing, we can continue to fight this virus in a targeted way,” Dr Fong said.
“A way that allows Fijians to access essential services and allows the economy to function as normally and safely as possible.”
The government also said an additional 50,000 doses of the AstraZeneca vaccine would be flown from Australia this week. More than 206,000 people have now received their first dose, while 4599 are now fully vaccinated.
This article is republished under a community partnership agreement with RNZ.
A Cook Islands man who has been on holiday in Rarotonga since May 21, 2021, has tested positive for covid-19, after requesting to be swabbed Friday evening.
The alert level remains unchanged and the risk to public remains low, the government said.
The man who arrived in Auckland from Egypt on May 5, 2021, tested positive on his Day 0 test when in managed isolation (MIQ) in Auckland, according to a statement issued by Te Marae Ora Ministry of Health.
The Health Ministry said the man was asymptomatic and his test was deemed a historic case. As of Saturday evening, he remains asymptomatic.
According to the ministry, a historical case means such cases are no longer infectious.
Because he needed to have a covid-19 test before returning to Egypt, he requested one late Friday and the result came back positive. The man was not showing any symptoms of the disease.
In a statement, Health Secretary Bob Williams said Te Marae Ora staff acted with urgency late last night and had taken this matter very very seriously.
Travel history
At 11.30pm Friday night upon confirmation of a positive test result, the Health Intelligence Unit was activated, and staff recalled.
Investigations took place to find out whether this person was infectious, where he had been and his travel history.
Between 1am and 6am Saturday morning the man, his wife, son, and nine close contacts were all tested and were self-isolating while the tests were processed.
The man was also tested again and again he returned a positive result.
His wife, son, and close contacts have returned negative test results, and no-one has been required to self-isolate.
“Our systems have been tested and have worked and I am confident with the results,” said Williams.
“Indications are that the positive test has reacted to an historical infection of covid-19. Overseas, people have been known to continue testing positive for the virus for some considerable time after they have recovered from it and are no longer infectious.”
“The Cook Islands police are presently investigating the matter in relation to the information the man provided in his arrival health declaration form,” Williams added.
The country remains at Alert Level 1.
This article is republished under a community partnership agreement with RNZ.
Three senior members of Fiji’s Ministry of Health have tested positive for covid-19, taking Friday’s total new cases to 35.
The three are part of the operations in the Covid-19 Incident Management Team and work in its leadership group, including senior advisers to Health Secretary Dr James Fong.
Responding to enquiries from RNZ Pacific, the Ministry of Health confirmed the reports.
It said all staff operating from Level 3 of its headquarters have been told to “stand-down”.
“The primary contacts have been identified and safely quarantined.
The services of the Covid-19 Incident Management Team will continue with contingency plans activated.
The Health Ministry is also informing the public that Dr Fong will be issuing daily statements during this period, and will provide updates on the covid situation from the Ministry of Health as and when required.”
Meanwhile, the three staff are part of 35 new cases recorded yesterday. The Ministry of Health said there were now 378 active cases in total.
The new cases include 10 more patients from the Colonial War Memorial Hospital in the capital Suva although it is not clear if they were staff or existing patients.
There are also 11 more cases from Lami which had been until last week – covid free. The other cases include 2 more from the Navy cluster, 5 from Navosai outside Nasinu Town and 1 from Nadali in Nausori.
Dr Fong said in his Friday evening statement that the Ministry of Health would continue to conduct contact tracing, screening and testing aggressively, “which is our best defence against community spread until we reach our vaccination goals.”
There have been 571 cases since the pandemic began and 501 have been from this current outbreak which began in April.
This article is republished under a community partnership agreement with RNZ.
LGBTQ communities are celebrating a joyful Pride season as COVID restrictions ease, and an end to a different epidemic is in sight — the HIV/AIDS epidemic. Unlike COVID, there is no vaccine for HIV, a virus that has shaped queer life and activism for the past four decades. Still, drugs that treat and prevent HIV are so effective at suppressing the virus that experts and health agencies say the epidemic could come to an end by 2030 if the right policy decisions are made. To reach this goal, advocates say archaic state laws that criminalize the most marginalized people impacted by HIV must be updated or repealed altogether.
HIV criminalization may sound like a thing of the past, but 32 states across the country still have laws on the books designed to punish people who have tested positive for HIV by creating or enhancing criminal penalties for various behaviors. In multiple states, people who have tested positive for HIV could face years in prison and even be registered as a sex offender if a former sexual partner accuses them of failing to disclose their status — even if they had safe sex or take medication that suppresses the virus and fully prevents transmission to others. In most states, these laws are HIV-specific. In 2020, only 11 states had laws that attempt to criminalize or control behaviors that could expose others to sexually transmitted and communicable diseases besides HIV, such as hepatitis.
HIV laws are often based on misconceptions of how HIV is spread that were disproven years ago, according to the Centers for Disease Control. In many cases, the laws are so vague that they can apply to various consensual sex acts, even though oral sex, for example, poses little to no risk of transmission. Some laws make it a crime to expose another person to bodily fluids even if no sex or injection drug use was involved, despite the fact that it is virtually impossible to transmit HIV that way. (HIV and other pathogens can be transmitted when people share syringes for injecting drugs, so it’s crucial that clean syringes are available to anyone who needs them.) In Louisiana and other states, an HIV-positive person could be charged with a felony for spitting on or biting someone else, even though we’ve known for decades that HIV is not spread by saliva. The maximum sentence under Louisiana’s law is 10 years in prison.
Enforcement of HIV criminalization laws disproportionately targets women, gay and bisexual men, injection drug users, sex workers, LGBTQ youth, and Black and Brown people in particular, according to advocacygroups. Advocates say HIV criminalization laws do not keep anyone safe; instead, they entangle people in violent criminal legal systems and create stigma around HIV that pushes vulnerable people away from treatments and services that are necessary for saving lives and ending the epidemic. Criminalization discourages people from getting tested for HIV, accessing treatment or disclosing their HIV status in the first place, according to the American Psychological Association.
Researchers at the Williams Institute at the University of California, Los Angeles have studied the impacts of HIV criminalization laws across the country. Executive Director Brad Sears said the laws were ostensibly written to prevent the spread of HIV, but they come from an era of homophobic panic about a disease that is easily treated today. Hundreds of people across multiple states, many of them Black and Brown, have been incarceratedfor years at a time as a result. Even more have been arrested and faced serious criminal charges in court, particularly in states where prosecutors are not required to prove a defendant intended to spread the virus.
“These laws weren’t really motivated on sound public health information when they were passed, and they were passed at a time when there was a lot of stigma and fear and discrimination against LGBTQ people, and especially gay men,” Sears said in an interview.
While HIV prosecutions against gay men, and especially Black men, have made headlines, HIV crime laws also disproportionately impact women, especially women of color and trans women. Many women have been arrested and sent to prison based on accusations by former partners who used HIV laws as a “tool of harassment and control,” often after the women attempted to end the relationship, according to the Positive Women’s Network. HIV crime laws put women in a terrible bind: Women are more likely to face violence from partners if they disclose their HIV status, but they can be arrested and prosecuted if they do not.
HIV crime laws are not just a tool used by abusive ex-boyfriends. Sears said researchers know the laws do not prevent the spread of HIV, but they do provide police and prosecutors with a powerful weapon against the vulnerable. After all, it’s more straightforward to prove that someone is HIV positive than whether they committed a crime. A relic of the days when an AIDS diagnosis was compared to a death sentence, HIV charges can carry hefty prison sentences or enhance sentencing for other crimes, allowing prosecutors to hang years of prison time over a defendant’s head to extract a plea deal.
In California, 95 percent of people who came in contact with the criminal legal system based on their HIV status between 1988 and 2014 were suspected of engaging in sex work, and many were entrapped or stopped by the police rather than being caught in the act, according to Sears. Black women represent only 4 percent of the HIV diagnoses in California but 21 percent of those who were arrested on charges related to their HIV status.
“One way to really address this issue is to just [end] the criminalization of sex work, and that would rapidly bring down…the enforcement of HIV criminalization laws as well,” Sears said.
In Missouri, prosecutors in St. Louis made a habit of filing HIV charges against Black men accused of resisting arrest, according to Sears. Facing an embarrassing jury trial and lengthy prison sentence for violating a state HIV law, the defendants took plea deals rather than fight charges. Like other states, Black men were targeted for HIV prosecution in Missouri more than any other group.
“You’ve got a disease that disproportionately impacts people of color and particularly Black people, layered on top of that a criminal justice system that disproportionately impacts people of color and mainly Black people, and then you make a crime out of that disease there is only one result that is going to happen,” Sears said.
Eight states have repealed or updated parts of their laws to reflect the current science on HIV, but LGBTQ advocates and public health experts say the government should not cast people with a health condition as potential criminals in the first place. Sears said HIV criminalization runs counter to efforts currently rolling out in every state to end the HIV epidemic by 2030, because the people most often targeted by prosecutors for HIV crimes come from the same marginalized communities that public health workers are trying to reach with HIV testing, treatment and prevention.
“These laws run counter to fighting the AIDS epidemic by targeting the very communities that you most need to engage right now to really bring an end to HIV: people of color, LGBT people, transgender people and people who are sex workers,” Sears said.
The head of the Fiji’s defence force has rejected claims by opposition MPs in Parliament this week and has called for an apology over the “simply, wrong” allegations.
In a statement, Commander Viliame Naupoto said there was no “factual evidence” to suggest that the defence force had caused the initial breach.
Commander Naupoto said the military was carrying its own investigations.
Health officials have also said medical and military personnel in Fiji who have been infected with covid-19 are not part of the frontline response teams.
The assurance comes amid an escalating number of cases on the main island, Viti Levu, with clusters in both hospitals and the Navy.
Health Secretary Dr James Fong said the frontline public health response teams were conducting surveillance and containment efforts in the communities.
He said the ministry screened and tested its frontline personnel for their safety and the public’s safety because “they come into contact with persons who have been exposed to the virus”.
Risk eliminated
Dr Fong said this also ensured the risk to the public from contact with their trace and containment teams was eliminated.
He said the ministry expected all frontline teams would “carefully observe the covid-safe protocol and we appreciate the feedback we get from the public in this regard”.
“Covid-safe behaviour needs to be maintained by all sections of the community, but especially those in the front line of the public health response and clinical response,” he said.
“At this time, when we have seen an escalation of cases, we wish to remind all frontline workers of the higher level of covid-safe behaviour expected by the community and our profession.
“The same is true for all community leaders and persons in leadership positions in our community in setting an example of a high standard for covid-safe behaviour at all times.”
Dr Fong said last night that 23 of the latest count (28) were linked to existing clusters.
The navy cluster began when an officer contracted the virus at a funeral and later infected members of his ship. This cluster continues to grow with 31 more cases this week alone.
The infected officers were isolated onboard three separate ships anchored in Suva.
Military headquarters locked down The military headquarters in Suva has been locked down in recent weeks after four soldiers tested positive.
Mingling between personnel at a quarantine facility in April has also been linked to cases.
The army said it was continuing to provide security services for the covid response teams.
It said two separate bubbles were already in place to contain the spread of the virus at the Queen Elizabeth Barracks (QEB).
Concerns were raised by people on social media over members of the defence forces being infected with the virus.
In Parliament yesterday, opposition MPs Lynda Tabuya and Simione Rasova criticised the military over its handling of officers who had breached managed isolation protocols at a government facility in April.
Tabuya claimed the “military officers caused the original breach and Navy officers also breached Covid borders”.
Rasova said “army and navy officers were spreading covid”.
Commander rejects claims
But Commander Naupoto rejected their claims.
He said there was no sharing of cigarettes as mentioned in the earlier press conferences by health officials, adding that one of the soldiers was in his room when the sharing of cigarettes was alleged to have taken place.
He claimed this was proven by CCTV footage.
Commander Naupoto said there was also an allegation that a soldier had come into contact with a repatriated citizen while the officer was carrying out an inspection without wearing any protective clothing, “again this was proven wrong by CCTV footage”.
“The whole border quarantine process is being reviewed by the quarantine experts in the Ministry of Health to plug any gaps that may exist in the current protocols that are being used and there are systemic issues that need to be reviewed.”
Fiji has recorded 536 cases since March 2020, 466 from the current outbreak which began in April while 349 patients remain infected with covid-19.
Four people have died.
This article is republished under a community partnership agreement with RNZ.
Fijian authorities have confirmed 28 new cases of Covid-19, taking the total number of active cases to 349.
The Ministry of Health said last night that 23 of the latest count were linked to existing clusters with 16 of them from the Navy, two from Nawaka, Nadi – one from the main hospital in the capital Suva and four from the anti-corruption commission.
Health Secretary Dr James Fong reassured the public that new cases were not military or health care workers currently engaged in community surveillance and testing.
The remaining cases include three close contacts of a case under investigation from Caubati near Suva that was announced on on Tuesday.
One case is under investigation with no known links to other cases at this stage, Dr Fong said.
The other case from Navosai, Narere was tested at the Valelevu Health Centre in Nasinu with symptoms, and an investigation is underway into any links between this case and other cases.
Dr Fong said the Colonial War Memorial (CWMH) Hospital in the capital Suva continued to operate as authorities analyse how best to secure the facility and still provide medical services to the 300,000 members of Fiji’s population it services.
Extensive swabbing
He said extensive swabbing was conducted at the hospital, and had revealed over a dozen positive cases.
“We are still in the process of evaluating the data, and the results of testing will determine the best way to secure CWMH while continuing to safely provide medical services to Fijians who access health services at the hospital,” he said.
“While emergency services, inpatient paediatrics and obstetrics services continue at CWMH, the hospital has shut down outpatient and special outpatient services as well as the Acute Medical Ward, Acute Surgical Ward and the paying wards; Beqa and ANZ.
“The Maternity Ward and Children’s Wing have developed stringent screening areas in the Antenatal Clinic area and the Children’s Outpatient Department for patients requiring urgent admission.
“All access to and from other parts of the hospital has been closed off to the Maternity and Children’s Wing. CWMH contingency plans for emergency scenarios have been finalised.”
The nearest major hospital on Viti Levu is in Lautoka, four hours away by road.
“We want to reassure the public that all the medical and security forces who have turned positive are not part of the public health team directly engaging the public in our containment and community surveillance programs.”
Navy cluster fastest-growing The ministry said more than 300 people in Fiji were carrying the Delta variant, first detected in India, and one of the fastest rising clusters was the naval division.
The navy cluster began when an officer contracted the virus at a funeral and later infected members off his ship.
This cluster continues to grow with 31 more cases this week alone, and concerns have been raised over one of the new cases announced earlier from Lami Town near the capital, which had previously been covid-19 free and is located outside of the containment zone.
Lami is now the start of a large containment zone which stretches through the capital Suva, through Nasinu and Nausori towns. That area is home to 300,000 people.
In the Western Division, Nadi Town and Lautoka City have also become one large containment zone.
Earlier, Prime Minister Voreqe Bainimarama said that areas with known covid cases (red zones) would become small containment areas where government teams could operate.
“We simply must be able to contain this virus without shutting down large parts of the country again.
‘Stop it in its tracks’
“We have accumulated a lot of knowledge about how this virus is spreading in our country and are going to put that knowledge to work not just to stop it in its tracks but also to recommence economic activity.
“From now the establishment of specific locked areas and teams made up of the ministry of health and medical services, RFMF and Fiji Police sweeping across suburbs and localities in high risk zones screening and swabbing will be a major part of the targeted surgical approach.”
Dr Fong said the increase in cases highlights the point: ‘no country is safe until every country is safe’ and he said for Fiji, “nowhere was safe until everywhere was safe.”
In response to community antagonism particularly after previously Covid-19 towns were reopened, Dr Fong said there was no “us against them” and said not having cases was not indication people were safe.
Contact tracing underway in Fiji. Image: Facebook/Fiji govt
On Wednesday, a high chief in Nadi criticised the Health Ministry’s decision to relocate people in quarantine to their province from the Central Division.
The ministry had said last week that primary or close contacts of cases that tested negative on their entry and fourth-day tests were to serve the rest of their 14-day quarantine in Nadi.
However, since the local transmission of covid-19 cases began from a quarantine facility in Nadi, Tui Nadi Ratu Vuniyani Navuniuci said there was no guarantee another quarantine facility breach would not occur.
‘Not Suva against Nadi’
But Dr Fong said: “it is not Suva against Nadi or other parts of Fiji. We are all in this together and we must combine our resources to stop the virus where we know it is spreading.”
“In the same vein, as our operations move on we will need to create more quarantine and isolation facilities. I ask that the general public help us by accepting these facilities in or near their communities and understand that these facilities are safe.
“They are carefully controlled and pose no danger. Quarantine and isolation facilities are a necessary part of our battle to be covid-contained, and we need them.”
Dr Fong said the ministry’s strategy was unchanged and was focussed on finding the active cases, locate their contacts and reduce the unnecessary movement within the containment zones – with the emphasis on covid-safe behaviour.
“Our capacity to stop this virus is really in the hands of every Fijian. It only works if the people act with extreme caution and follow the recommended protocols.”
Fiji has recorded 536 cases since March 2020, 466 from the current outbreak which began in April while 349 patients remain infected with covid-19.
This article is republished under a community partnership agreement with RNZ.
As the number of Fiji’s covid-19 positive cases continues to rise, there is obvious discomfort and great concern among many Fijians.
This is to be expected. When you consider the recent easing of border restrictions in strategic areas around the country, there will be some sense of trepidation.
We may fall back on the advice and reassurance of the Ministry of Health and Medical Services, however, it is still difficult for many people to accept the recent turn of events. The rising numbers are worrying.
They are a major concern. Interestingly, in the face of the rising numbers sits questions on adherence to physical distancing rules, and common sense.
There will be issues hovering around public transportation for instance, social gatherings, and funerals.
We learn that public service vehicle (PSV) operators are saying people need to adhere to covid-19 restrictions and social distancing requirements.
This reaction comes in the wake of concerns raised about crowding on PSVs in the Lami, Suva and Nausori containment zone.
It is frightening to note the rise in numbers. However, we can be buoyed by the fact that we know what to do to keep the virus away.
Fiji Bus Operators Association president Nisar Ali said information on social distancing protocols has been widely disseminated and people should follow them.
It was everybody’s responsibility, he pointed out, to ensure that when travelling on public service vehicles, they maintained social distancing.
Drivers, he said, could only tell the travelling public to distance themselves and enforcement was done by the Land Transport Authority and the Ministry of Health and Medical Services.
Fiji Taxi Association president Raben Singh said the same protocols introduced when covid-19 first came applied to taxis.
He said no one would be allowed into taxis without a mask and passenger numbers were now limited.
“Drivers are even selling masks to help facilitate their travel, but people should not be moving around unnecessarily.”
In the face of all these rules, police spokeswoman Savaira Tabua said they would continue to restrict movements of people despite the uplifting of borders.
“Our officers are manning checkpoints to ensure restrictions are followed,” she said.
“We would also like to encourage the public to be responsible. We will not be everywhere, therefore, their support is needed.”
The onus really is on us as individuals to make sound decisions daily. It is unfortunate that many people are not adhering to physical distancing rules when they board buses and cabs. The question is how do we ensure this is done though!
This certainly isn’t the time to be living dangerously. It’s clear that the cluster that attended a funeral recently came off as a major spreader of the virus.
It is a tough ask, but we can only hope that Fijians consider this when farewelling loved ones moving forward.
It is frightening to note the rise in numbers. However, we can be buoyed by the fact that we know what to do to keep the virus away.
The challenge is to be vigilant. Thousands of Fijians depend on us all making the right decisions daily.
The Fiji Times editorial, 3 June 2021. Republished with permission.
When Ramona Hernandez turns on her kitchen faucet in El Adobe, an unincorporated town just a few miles southeast of Bakersfield, the water that splashes out looks clean and inviting. But she doesn’t dare drink it.
“You worry about your health,” she said in Spanish as she sat in her tranquil front yard one morning early this spring, her elderly mother-in-law working in the garden behind her.
“I’m scared,” Hernandez said, “of getting sick from the water.” Drinking the tap water in this tiny community of dusty ranches and unpaved roads could expose Hernandez to arsenic. So, for years, she and her husband, Gerardo, have shuttled twice a week to the nearby town of Lamont to load up on bottled water. At a cost of about $80 a month, it’s enough for drinking and cooking. If they had the money, Hernandez, 55, would buy bottled water to shower with and use for her chickens. But given her husband’s salary as a farmworker, she says, that’s not a realistic option.
Like more than 300 communities across California, El Adobe lacks safe drinking water. Since 2008, the arsenic levels in one of its two wells have regularly exceeded the safety standards set by federal and state authorities, often by more than double. Long-term exposure to arsenic in drinking water is linked to diabetes, high blood pressure and cancer.
Contaminated drinking water affects an estimated 1 million people in California, many of whom rely on private wells or small community water systems like El Adobe’s. A majority of these residents live in the Central and Salinas valleys. These are largely low-income, rural and Latino communities, where lack of access to clean water exacerbates the health disparities that already exist due to structural inequities. Since 2012, California law has recognized that access to safe and affordable water is a human right, but action has lagged behind the language.
Arsenic levels in El Adobe’s other well are currently deemed safe, but the well can’t provide enough water to meet year-round demand. That means that many residents of the unincorporated town, including the Hernandezes, continue to pay for water they can’t drink. The El Adobe Property Owners Association charges households $125 a month for tap water, money that also covers streetlights and road maintenance (although only one road is paved). Most residents also buy bottled water at the store. Others take their chances and drink the tap water despite the risks. Many townspeople are low-income farmworkers and retirees, and buying bottled water is a significant expense.
“I can’t afford bottled water all the time,” said Kyle Wilkerson, 40, a father of three who lives on a fixed disability income. He’s also president of the El Adobe Property Owners Association, a small cadre of community members who manage the town’s water infrastructure almost entirely as volunteers.
Wilkerson said he worries about his own health as well as that of his family. “But what am I going to do?” he said. “You get to the point of, it is what it is.”
And indeed, residents in towns like El Adobe have few options. Arsenic can be removed from water, but it’s prohibitively expensive for most small towns. An arsenic treatment facility requires millions of dollars to build and another $100,000 or more per year to operate, said Chad Fischer, an engineer who works at the California Division of Drinking Water’s district office in Visalia, which regulates water in the region.
El Adobe is so small — just 83 homes — that if community residents split the cost of a treatment system, they’d spend tens of thousands of dollars each and face dramatically increased water rates. “The math is awful,” Fischer said. “It ends up being unaffordable.”
It’s possible for individual users to install an advanced filtration system, such as reverse osmosis, in their homes, usually under the sink, to remove arsenic. But these systems can cost hundreds of dollars to install and maintain. Some small water systems do install these in people’s homes, passing on the cost to consumers, but the state considers this a temporary fix. Inexpensive pitcher-type filters do not remove arsenic.
A permanent solution was supposed to be coming for El Adobe. In 2013, with funding from the California State Water Resources Control Board, El Adobe commissioned a report that concluded that the best option for the community was to connect with the larger water system in Lamont. According to Scott Taylor, general manager of the Lamont Public Utility District, the state promised to grant Lamont enough money to build the connecting pipeline, service lines and new wells needed to accommodate the increase in users and replace aging infrastructure.
“Eight years, it still hasn’t happened,” said Taylor. “I think it’s bureaucracy. For example, when we submit any kind of a document, a cost estimate, an engineering report … for whatever reason, it takes them two to three months to review it. If it took any of my staff a month to review a document, I don’t care if it’s 100 pages, I’d fire them.”
Blair Robertson, a spokesman for the California State Water Resources Control Board, said the state is still waiting for Lamont to purchase land for the new wells and drill test wells to see if water at the proposed sites is contaminated. There is currently no start date for the project, which is estimated to cost between $13 and 22 million and will likely be split into several construction phases. Formal state approval of the project will likely be in 2022, Robertson said, but there’s currently no timeframe for when El Adobe residents will have clean drinking water.
Planning and implementing a water system consolidation takes time, Fischer said, especially when the community, like El Adobe, is small and lacks a team of engineers and other professionals to manage the water supply. Lamont has its own water problems with contaminants and aging wells, which have added to the difficulties of the project, he said. Projects usually take five or more years to accomplish, he said, depending on their complexity. But it has already been eight years, and construction has yet to begin.
More Than 100 Others
Beyond those delays, dozens of other communities in California are also waiting on construction projects for clean water. Approximately 110 other out-of-compliance water systems in the state are planning or considering consolidation with another system. Sometimes, the larger communities resist appeals to absorb the smaller systems because they fear it will increase costs and strain their own water supply, particularly as droughts continue. The state often offers financial incentives to encourage consolidation, and can mandate it, if necessary. Other times consolidation isn’t even an option because a community is too remote.
In 2019, California passed a law that established a program called Safe and Affordable Funding for Equity and Resilience (SAFER), designed to help fund water improvements for communities that struggle to provide clean water to their residents. The state water board is working to complete a needs assessment to determine which water systems need help and to what extent, according to a recent report by the state’s Legislative Analyst’s Office. However, the state is still “in the very early stages of implementation,” and “much work remains to be accomplished” before all Californians have access to safe and affordable drinking water, the report stated.
Cheryl Blackhawk, 67, and her husband Edward, 69, are fed up with not having safe water in El Adobe. They moved to the town four years ago from nearby Greenfield, seeing it as a quiet and affordable place to retire. At the time, the seller assured them the water connection to Lamont would happen within a year. They’re still buying water bottles by the caseload from Walmart.
“You can’t go to the faucet to get water to drink,” said Edward Blackhawk. “You can’t cook.”
Contaminants aren’t the only problem. Like innumerable systems across California and the country, El Adobe’s wells, pipes, pumps and other water infrastructure are showing their age. El Adobe’s most critical well, the one without arsenic, was built in 1967, the same year Ronald Reagan became governor of California and labor activist Cesar Chavez initiated a nationwide boycott of the state’s table grapes. The community’s arsenic-laced well was built in 1985.
The life of a well depends on the chemicals in the local soil and water, and the quality of the well materials and construction, said Dave Warner, community development manager at Self-Help Enterprises in Visalia, which helps low-income communities access funding for water projects. But a well as old as 1967 “is really pushing it,” he said. Over time, the casing inside the well corrodes, and sand and other contaminants can get into the pump, causing it to fail. Still, drilling a new well costs more than $1 million, according to water officials. Securing state funding for it can take more than a decade, Warner said.
The precariousness of the situation is not lost on Edward Blackhawk. Without functioning wells and pumps, people’s faucets would run dry. Toilets wouldn’t flush.
“If these wells go down, we’re out of luck,” he said. “We’re out of water.”
Widespread Water Woes
Three miles down the road, Lamont has its own water struggles. Five of the town’s eight wells are contaminated with a highly toxic chemical called 1,2,3-trichloropropane, or 1,2,3-TCP. The chemical was added to soil fumigants used in agriculture during the 1940s through the 1980s. It persists in the environment indefinitely and is recognized as a carcinogen by the state of California. The state started regulating the chemical in drinking water in 2017, which meant communities like Lamont had to find a way to remove it.
Just like arsenic, 1,2,3-TCP is expensive to get rid of. A treatment system costs over $1 million per well, plus about $100,000 a year to change the filter, said Taylor. Lamont has installed treatment on four wells, using money from a settlement with Dow Chemical and Shell Oil, the companies allegedly responsible for the contamination. But two of the treatment systems are leased, and the utility district still doesn’t know how it will pay for them long-term. Two other wells still need 1,2,3-TCP and arsenic treatment systems, respectively.
Lamont’s population of 15,000 is almost entirely Latino, and many residents are farmworkers. The average per capita income is just over $13,000 a year. Plans to raise water rates last year to help cover some of the district’s expenses were delayed because of the pandemic. Even so, dozens of accounts fell into delinquency as people lost jobs and struggled to pay bills. The district is now short about $70,000 from delinquent accounts, Taylor said.
Lamont’s wells are also nearing the end of their lifespan. Last year, shortly after the district installed a $1 million filtration system for 1,2,3-TCP on a 60-year-old well, the well collapsed. Taylor said he “raised holy hell” with the state water board and obtained emergency funding to build a new well, which is now under construction. Another three wells need replacing, he said. Those new wells may also need treatment systems. Funding for that is supposed to be included in the consolidation project with El Adobe.
So far, Lamont has managed to provide clean water to residents, but that could change if another well breaks or demand increases enough to require making a contaminated well operational, said Taylor.
“It’s a little discouraging,” said district board member, Miguel Sanchez. “You’re trying to comply with all these regulations and the system is crumbling.”
A Reason for Hope?
But Californians now have a reason to be optimistic: A $2 trillion proposal by President Joe Biden to fund infrastructure improvements across the nation, including for clean water, could provide their state with more money for these types of projects. Biden’s plan — if approved by Congress — would include $111 billion dollars in clean water investments. The proposal seeks $10 billion to monitor and remediate new drinking-water contaminants and to invest in small rural water systems like El Adobe’s. The plan also requests $56 billion in grants and loans to upgrade and modernize America’s aging drinking water, wastewater and stormwater systems. Support for low-income communities and communities of color is a big focus of the proposal.
It’s not yet clear how much of the money would go to California. However, Gov. Gavin Newsom has called Biden’s plan “a game changer.”
And Warner, with Self-Help Enterprises, agreed. Right now, there’s not enough state and federal money available to efficiently tackle all of California’s water contamination and infrastructure problems, he said. Biden’s plan “gave me a lot of hope,” he said. “But it’s got to get approved.”
Meanwhile, Susana De Anda, co-founder of the Community Water Center, an environmental justice organization based in Visalia, applauded California’s SAFER program, but said communities need help faster. A short-term solution would be for the state to implement a rate-assistance program for low-income residents who are struggling to pay their water bills, including those who pay for water twice because their tap water is contaminated, she said.
“We want solutions now,” she said. “It’s a huge problem, and we have generations that have been condemned to this reality.”
In El Adobe, Hernandez worries that she may be inhaling contaminants or absorbing them through her skin when she showers. The concentration of arsenic in the water is still safe for bathing, according to state regulators, and arsenic does not evaporate into the air, but Hernandez remains distrustful, particularly since she and her husband both have lung problems.
If only officials in Sacramento could spend a day in her shoes, she said. “How would they like it?” she asked. “They don’t have to worry about having a shower, about drinking the water.”
At the edge of the community, Cheryl and Edward Blackhawk checked on El Adobe’s second well, the arsenic-laden one, and its water tank, which sits inside a small enclosure littered with tumbleweeds. Cheryl Blackhawk, who serves as financial secretary for the property owner’s association, said she fears that drought conditions this year will lead to falling water levels that result in higher arsenic concentrations in the well.
Her husband, standing quietly beside the aging pump, confessed he’s beginning to doubt the connection to Lamont will actually happen.
“There’s a lot of people out here who think it’s dead in the water,” he said softly. “And it’s not just us. There are hundreds (of communities) like us in the state.”
This story was supported by a grant from The Water Desk, with support from Ensia and the Institute for Nonprofit News’s Amplify News Project.