The U.S. Senate recently passed the Drinking Water and Wastewater Infrastructure Act. The legislation creates a $35 billion fund that will allow states and tribes to make urgently needed upgrades to their water systems, with additional considerations made for frontline communities. This kind of commitment to commitment to environmental justice is welcome, but also long overdue.
Clean water infrastructure has experienced systemic neglect in communities across the U.S. In Jackson, Mississippi, residents recently had to boil water for drinking, and thousands lacked access to non-potable water for flushing toilets. Unfortunately, these upsetting circumstances are common, particularly in communities of color.
Millions of Americans experience the dire consequences of toxic drinking water, which negatively affects quality of life, and can lead to a lifetime of debilitating health effects.
Black and Brown communities feel the brunt of this burden. Research shows that drinking water systems in communities of color are 40 percent more likely to violate clean water standards than in non-Black and non-Brown communities. This is environmental racism. And it’s destroying countless lives.
Like most forms of racism, high-profile tragedies like Flint, Michigan, grab headlines. But often, it’s a slow, quiet and deadly progression that devastates communities of color.
A recent study found Black children of families living below the poverty line are more than twice as likely to have elevated levels of lead in their blood than white or Hispanic children living under the poverty line.
For decades, petroleum refineries along the Mississippi River have polluted local waters with cancer-causing petrochemicals. In majority-Black Louisiana communities, there are more than 150 of these refineries, located between New Orleans and Baton Rouge in what has been ominously dubbed “Cancer Alley” due to the refineries that spew dangerous chemicals into the water.
Environmental racism also persists within the vulnerable communities surrounding chemical storage and industrial sites, where toxic floodwaters caused by storms or climate-related events carry heavy metals, oils and gas into local waterways. Individuals affected by these floods often face immediate health problems, including headaches, dizziness, and irritation to the eyes and throat.
These toxic floodwaters most often impact Black and Brown communities. A report co-written by the Center for Progressive Reform and the James River Association found more than 473,000 Virginians live in communities that are both high in social vulnerability and contain flood-exposed industrial facilities. Like the harm caused by petroleum refineries, this flooding can leave communities with significant long-term health challenges.
We’ve made slow progress in addressing other forms of institutional racism, but we’re only beginning to reckon with the cost of environmental racism. Flint was a wake-up call, but not nearly enough has been done to address the root problems or hold the perpetrators accountable.
Black and Brown communities don’t have the luxury of sweeping the problem under the rug. These communities live with the consequences of environmental racism daily. The quality of life and health impacts are only beginning to be detected.
The federal government has acknowledged the peril caused by environmental racism — the Environmental Protection Agency’s (EPA) National Center for Environmental Assessment concluded that non-white communities are disproportionately put at risk of health effects from pollution. Thankfully, we now have an administration that is signaling its intention to make decisions based on truth, facts and science. President Biden has expressed that environmental justice will become a central tenet of his administration, and has prioritized clean water infrastructure investment and combating climate change impacts in his Build Back Better plan.
Yet environmental racism is a decades-long abuse in this country. Action must come now. It’s imperative that Biden continue to take immediate executive action to reverse this horrific and systemic damage. The administration must also make up for lost time by prioritizing enforcement of our environmental laws to benefit the communities whose health and well-being have too often been afterthoughts.
The Biden administration has offered signs of hope. A reversal on Bears Ears National Monument and the Keystone XL pipeline are encouraging. The appointment of Deb Haaland, the first Native American to hold a cabinet position, to lead the Department of Interior, is another good start.
But these good intentions must become a firm reality.
The Biden administration must immediately implement its own agenda, including empowering a more aggressive EPA to expedite hazardous waste remediation and cleanups in frontline communities that have long carried the burden; establishing an Environmental and Climate Justice division at the Department of Justice to ensure environmental tragedies like those experienced in Flint do not occur again and that environmental lawbreakers are held fully accountable for the violence they unleash on their victims; overhauling and empowering EPA’s External Civil Rights Compliance Office with more staff and resources and a directive to focus on environmental justice to protect communities from climate change; and mandating stricter monitoring. A more fully engaged Office of Environmental Justice would also help address these urgent and necessary changes.
There’s too much at stake for Black and Brown communities. Too many lives have been expected to cede priority to the profits of polluters. Just look at Flint, or the other marginalized communities where something so vital as drinkable water is not guaranteed.
Enough is enough.
Clean water is a human right. It’s time to start treating it as such.
Bananas, balaclavas and banners … these were stock-in-trade for human rights activists of the New Zealand-based Coalition for Democracy in Fiji who campaigned against then Colonel Sitiveni Rabuka’s original two coups in 1987 and the “banana republic” coup culture that emerged.
Many of the original activists, politicians, trade unionists, civil society advocates and supporters of democracy in Fiji gathered at an Auckland restaurant in Cornwall Park to reflect on their campaign and to remember the visionary Fiji Labour Party prime minister Dr Timoci Bavadra who was ousted by the Fiji military on 14 May 1987.
Speakers included Auckland mayor Phil Goff, who was New Zealand foreign minister at the time, and keynote Richard Naidu, then a talented young journalist who had emerged as Dr Bavadra’s spokesperson — “by accident” he recalls — and movement stalwarts.
The mood of the evening was a fun-filled and relaxed recollection of coup-related events as about 40 participants — many of them exiled from Fiji — sought to pay tribute to the kindly and inspirational leadership of Dr Bavadra who died from cancer two years after the coup.
Participants agreed that it was a tragedy that Dr Bavadra had died such an untimely death at 55, robbing Fiji of a new style of social justice leadership that stood in contrast with the autocratic style of the current Fiji “democracy”.
Naidu, today an outspoken lawyer and commentator, spoke via Zoom from Suva about Dr Bavadra’s unique approach to politics, not unlike a general practitioner caring for his patients, a style that was drawn from his background as a public health specialist and trade unionist.
He referred to Johns Hopkins University in the United States — “the bible of global statistics about covid-19 pandemic in the world” — and remarked that Dr Bavadra had gained his public health degree at that celebrated campus.
Covid and Dr Bavadra
Naidu asked how, if he had been alive today and still prime minister, Dr Bavadra might have approached the Fiji covid-19 crisis with 46 new cases of infection being reported last night.
Fiji has now had 360 cases in total since the first case was reported in March 2020, with 161 recoveries and four deaths.
A shadowy “banana republic” … protesters imitate the seizing of Fiji parliamentarians at gunpoint by hooded soldiers in response to the first coup on 14 May 1987. Image: David Robie screenshotPrime Minister Dr Timoci Bavadra ousted in Fiji’s first coup on 14 May 1987. Image: CDF
Naidu described the current leadership in Fiji in response to the covid pandemic as unresponsive and lacking in direction. He believes Fiji is in a worse position today than it was in 1987 and poverty and food shortages were a growing problem.
The challenge for Fiji was a lack of consultation with grassroots organisations and a “bubble” mentality among the key leaders of Voreqe Bainimarama’s government that refused to see the suffering on the ground.
“Everything was bad in Fiji before 2006 [when Bainimarama staged his coup],” he said, reflecting the leadership’s mantra. “Everything good in Fiji is after 2006.”
Lawyer Richard Naidu speaking about Dr Bavadra’s legacy and the reality of Fiji today. Video: David Robie/FB
Naidu referred to a social media posting in relation to the Samoan constitutional crisis when he commented: “ Australia and New Zealand must be wondering: Is Samoa ‘21 just a rehearsal for Fiji ’22.” The question is what would happen if Bainimarama loses the election next year.
In spite of his fears for the future, Naidu said he still remained optimistic because of the young leadership and committed civil society that was emerging in spite of the barriers.
‘Have we won?’
Looking back 34 years, Naidu asked the audience: “Have we won?”
With a negative response, he challenged the participants to keep working for a better Fiji.
Auckland mayor Phil Goff speaking at the Bavadra reunion last night. Image: David Robie/FB
Mayor Phil Goff said that after the 1987 coups, New Zealand did not just have a “trickle of migration, we had a flood of migration, and I think something like 20,000 or 30,000 people came from Fiji in the wake of the coups”.
And, he added, “that was a huge benefit to our country, it strengthened our country. But it was a huge drain on Fiji because these were the people with skills and energy and they could have been contributing had Fiji been a welcoming country, if everybody had first class citizenship.
“But they didn’t see that future for themselves in Fiji and I understand that and they came to make a better life in New Zealand.”
Goff called on those present to keep campaigning for human rights.
“Criminals go free in Fiji” … an image on display at the Bavadra event in Auckland last night. Image: David Robie screenshot
Union and NFIP days
Trade unionist Ashok Kumar recalled when he had worked for the Fiji Public Service Association and Dr Bavadra had been president at the time and he had inspired many people with the Nuclear Free and Independent Pacific movement, “which had been a big issue for Fiji”.
Trade unionist Ashok Kumar speaking. Video: David Robie/FB
Other speakers also spoke of their admiration for a “forgotten” Dr Bavadra and how they hoped to “keep his memory alive”.
Former National Federation Party MP Ahmed Bhamji said it was hoped that the Bavadra lecture event would become an annual one and he declared that they were already planning for the 35th anniversary of Rabuka’s first coup next year.
Bhamji was a sponsor of this year’s event and among his fellow organisers were Nikhil Naidu, Rach Mario and Maire Leadbeater, who was MC for the evening.
Friends of CDF …James Robb, Maire Leadbeater, Rach Mario and David Robie at the Bavadra event in Auckland last night. Image: David Robie/APROrganiser Nikhil Naidu … thrilled with a successful Bavadra night. Image: David Robie/APRFormer National Federation Party MP Ahmed Bhamji … engaging with Richard Naidu over Fiji’s future. Image: David Robie/APRAdi Asenaca Uluiviti (left) and Del Abcede at the Bavadra memorial event last night. Image: David Robie/APRSome of the CDF group and supporters at the Bavadra memorial event in Auckland last night. Image: David Robie/APR
COMMENT:By Fred Wesley, editor-in-chief, The Fiji Times
Bula.
The big announcement last night must be a very firm reminder for us all in Fiji about what we are dealing with. Permanent Secretary for Health and Medical Services Dr James Fong confirmed 46 new cases.
That must inch out some concern if it hasn’t already done so. It must force a rethink of what we do today and moving forward. So what were the key takeaways from this latest announcement?
Aside from the staggering figure, it has to be the fact that people are still engaging in unsafe behaviour! They are still attending large gatherings.
Understandably there are emotional aspects to consider, however, the fact remains, the virus moves when we move!
Think about what Dr Fong said: “This increase was not unexpected, but it should serve to show how easily this virus is transmitted and why restrictions are in place.”
This was Fred Wesley’s editorial yesterday before the announcement of 46 new cases.
EDITORIAL:Doing this together
In his announcement at 5.14pm yesterday [Friday], the Permanent Secretary for Health and Medical Services Dr James Fong confirmed 22 new cases of covid-19.
By 7.31pm, there were six more new cases added to this number, taking the total to 28 new cases yesterday.
Breaking down the cases in the earlier announcement, one was a resident of Kinoya with no links to other cases at the early stage of investigation, two were connected to the Queen Elizabeth Barracks cluster, seven were connected to the Navy cluster and 12 were residents of Vunivivi in Nausori.
They were connected through a common exposure event — a funeral!
In the late announcement, four cases were connected to the Muanikoso cluster and two to the Vunivivi cluster.
The rising number is surely going to attract interest.
In fact, it is going to raise concern as well.
There will be a great sense of apprehension, uncertainty, great fear, doubt, insecurity, frustration and anger.
It is not unusual that Fijians will look up to the powers that be for reassurance.
They will seek that and hope the powers that be are accommodating.
They will look to them for guidance, and to give them confidence to move forward.
They will need to be reassured enough to not panic in the face of the rising numbers daily.
So lest we forget though, let’s not panic right now.
Understandably it would be encouraging to get some semblance of order first up.
However, perhaps we can be buoyed by the fact that with the exception of one, all the other cases are actually connected to known clusters.
Whatever your take is on the growing numbers, we may take comfort in the fact that the outbreak right now is in the Suva-Nausori area.
Most of the new cases in recent days were discovered through contact tracing investigations for known cases.
This, according to Dr Fong, is an indicator that our contact tracing efforts are effective.
Now for the serious bit! The revelation that significant escalations in daily case numbers have been largely driven by the fact that recent cases have been linked to large households or workplace groups, funeral gatherings and the associated grog sessions in big groups is obviously a major concern.
Then there is the connection to a common exposure event — a funeral!
There can be no doubts about what we must do moving forward.
There can be no social gathering! In fact we should just stay home, within our little safe bubbles.
The virus will not move if we stay still. Thousands of Fijians are already doing their bit for the greater good of our nation. They are staying home.
They are staying within their bubbles. They are adhering to physical distancing rules. Together we must stay on course.
The Fiji Times editorial, 28 May 2021.
This content originally appeared on Asia Pacific Report and was authored by APR editor.
“Today has not been an easy day, nor do I expect that the days ahead will get any better. Many of you have questions. I hope to answer some now and I am assured that a press conference will be organised soon to answer more questions,” Dr Fong said.
Funerals seen as spreader events Calling attention to what he described as the troublesome nature of final rites, Dr Fong said funerals were the spreader events of the current outbreak of the B1617 variant of Covid-19.
The health head called on Fijians to adjust funerals and while he acknowledged it was a difficult time for all involved, he asked that people adjust activities to suit the current situation.
Authorities have restricted funerals to graveside services with only 10 people in attendance at the cemetery and lead up events.
“Everyone should recall that this latest outbreak gained momentum when one person who contracted the virus in the border quarantine area attended a funeral, yet funeral gatherings continue to be sources of spread,” he said.
“The deceased must be buried, and we must pay our respects and accompany them during their last hours on earth, but we must temporarily find new ways to do this.
“Families are urged to limit graveside services to 10 people and to limit gatherings before or after the burial to 10 people or less. Our investigations indicate that in some instances, funeral gatherings of 100 were split up into 5 so-called “bubbles” of 20 people.”
Existing clusters
Meanwhile, forty-three of the new cases are linked to existing clusters which had been under investigation and were detected through contact tracing and targeted screening.
Of the 43 new cases, 28 are from Nadali in Nausori town and 3 are from Navosai near Nausori which are linked to the Narere funeral cluster. Two are from the Muanikoso cluster which stems from a staff of Extra Supermarket in Suva city where an outbreak occurred a fortnight ago.
Meanwhile, nine more naval officers are confirmed positive, nine of whom are from Kinoya in Nasinu town and 1 is from Nadonumai in Lami which had previously been covid-19 free.
One cluster is linked to a Samabula household where a funeral had taken place a week ago.
The remaining three new positive cases are not yet linked to other cases and were still being investigated.
The Nadali red zone is 29 into a targeted lockdown while Muanikoso is on day 6.
“It is important to note that the majority of these cases have been found as a result of our extensive contact tracing effort and are linked to known clusters. This increase was not unexpected, but it should serve to show how easily this virus is transmitted and why restrictions are in place,” Dr Fong said.
Testing aggressively “We expect the number of cases to rise because we are testing aggressively in areas where we know the virus is spreading. We have a number of prominent locations under investigation including Government buildings and Kadavu House.”
The permanent secretary said covid-19 had spread within containment zones but assured medical authorities would be “exercising extra vigilance to ensure that there is no spread outside those containment zones”.
Enforcement of covid-safe restrictions including restrictions on movement and gatherings will be strengthened along with enforcement of mask-wearing, physical distancing among other measures, Dr Fong added.
The MOH has in the past week administered 19,348 AstraZeneca vaccines in the Suva-Nausori corridor and 24,042 in all of Fiji.
“To date, 18.5 percent of the targeted population have received at least one dose and 3117 individuals have had 2 doses.
“An additional 50,000 doses are due to arrive in the country by the end of the week. Once these doses are deployed, at least 260,000 persons will have got their first dose,” Dr Fong said.
Restrictions in West and North Dr Fong said the information from the Western Division where gateway town Nadi and port city Lautoka was good but authorities would exercise caution and continue surveillance work.
Restrictions in the Western division are being reviewed and changes to the containment measures there and in the Northern Division would be announced soon.
“We will need to maintain restrictions on movement from Viti Levu to Vanua Levu in order to ensure that Vanua Levu remains transmission-free. We will be exploring and announcing soon protocols of movement that will allow persons who have not been home for long to return home.
“This virus has kept families apart and has caused undue social suffering. Our response has been firm and has proven successful in the western division and in specific locations in the Central Division,” he said.
This article is republished under a community partnership agreement with RNZ.
A new wave of COVID-19 is hitting Thailand. Its daily tally has increased from less than 100 in early April to more than 2,000 a month later. The country now surpasses China in total COVID-19 cases. What comes as a shock to many is recent outbreaks in prisons nationwide which saw more than 10 thousand inmates infected.
This prison cluster is not surprising, however. Prison and detention centres in Thailand are notoriously crowded. Available official statistics suggest that prison population has tripled from 2010 to 2021. As of May 2021, the country has roughly 311,000 inmates nationwide, but the normal prison capacity is about 200,000. Several studies suggest that Thailand’s prisons have inadequate access to medical treatment, insufficient food and water, poor sanitation facilities, and severe budget constraints. Even before the COVID-19 pandemic, transmission of HIV/AIDs and other infectious disease such as tuberculosis and measles are common. Therefore, large COVID outbreaks in prisons are only a part of a bigger problem in terms of the state overlooking the welfare of prisoners.
Why are prisons in Thailand overcrowded? As of April 2021, 81% of all inmates are being held for drug-related offenses. From 2018 to 2021, while the number of convicted prisons for drug offences has been more or less the same, the number of those who are pre-trial/unconvicted has increased by 50%. Harsh drug laws are viewed as a major contributor to overcrowding in Thai prisons.
A recent study by the Thailand Institute of Justice cites changes in two legal standards that explain Thailand’s prison overcrowding. In 2002, by amendment of the Narcotics Act B. E. 2522 (1970), the threshold amount for presumption of intent to sell methamphetamine (known in Thai as ya ba) was dramatically reduced from 20 grams to 375 mg. This threshold is relatively low compared to other countries including Australia and Singapore.
Another legal contributor is the Rehabilitation of Drug Addicts Act B.E. 2545 (2002). This Act allows some of those found using or in possession of drugs to receive compulsory treatment instead of prison. The amount of drugs involved must be small in order to qualify for diversion. Those in possession of methamphetamine of more than five units or 500 mg are not eligible for diversion. After a short period of reduction, the number of people incarcerated on drug-related offences has since dramatically increased, from about 100,000 inmates in 2008 to more than 250,000 inmates in 2020. This may be in part due to an increase in the amounts of drug possessed, driven by falling methamphetamine price in East and Southeast Asia.
These reinvigorated drug laws were a part of the “war on drugs” campaign which was officially launched in February 2003 by Prime Minister Thaksin Shinawatra. This “tough on drugs” policy resulted in a large number of extrajudicial killings in a matter of three months. While the prime minister proclaimed victory, this campaign caused many, including the UN Human Rights Committee, to be concerned about violations of human rights . This is not to conclude that such draconian drug laws failed to eradicate drug problems and protect the Thai community; however, the resultant prison overcrowding has a cost to shoulder.
Many organisations (e.g., Thailand Institute for Justice, International Federation for Human Rights, and Human Rights Watch) have long called on Thailand’s Department of Corrections for urgent prison reforms to reduce population congestion. But how can an under-resourced prison system be expected to safely vet prisoners for early release? Thailand could widen the criteria for early release to include more prisoners, such as those in pretrial detention for nonviolent offences. Of more than 300,000 prisoners currently detained nationwide, about 20% are not convicted; either pending appeal, awaiting trial, or awaiting investigations. They could be released with electronic monitoring (EM) equipment. For the past few months, many countries (i.e., Indonesia, Iran, and Turkey) have temporarily released large numbers of prisoners. In the case of Thailand, since prisoners convicted of offences against drug laws form the largest group of the prison population, minor drug offences should be prioritised.
The benefit of such a program would not just reduce congestion in prisons in the time of the pandemic. Intriguing studies in Argentina, Australia, and France have found that electronic monitoring has a long-lasting effect on recidivism, thereby lowering the possibility of overcrowding in the future.
But reducing the prison population does not seem to be the first option. The Justice Ministry’s current priority is to vaccinate inmates and correctional officers. A sluggish vaccine rollout casts doubt on how the Thai authorities allocate the limited amount of vaccine between vaccinations in prisons and the mass immunisation drive (for adults aged between 18 and 59) to be started in June. Whether it is mandatory for prisoners to get COVID-19 vaccine is yet to be discussed.
Another unanswered question related to general prisoner welfare is how those who have COVID-19 are treated. The current outbreak in prison suggests that measures for COVID-19 prevention implemented by the Corrections Department are ineffective. At the time of writing, it is unclear how many field hospitals are set up for COVID-19 prisoners. More importantly, it is unknown whether these field hospitals have the required medical staff and facilities (beds, ventilators, etc.) because the healthcare sector has already been overwhelmed with increasing COVID infections. Many hospitals are short of beds and even have limited testing capacity.
While international organisations including Human Rights Watch and Amnesty International Thailand have voiced growing concern over recent the prison cluster and called on the Thai authorities to ensure adequate protective measures and healthcare in detention facilities, the Office of the National Human Rights Commission of Thailand is silent. It would be embarrassing if the timely protection of rights among prisoners cannot be upheld because of its lack of authority.
Nobody should be left behind during the pandemic. People deprived of their liberty are already vulnerable to infectious disease, but it gets worse in overcrowded prisons. It is now time for the Thai authorities to make every effort to solve this long overdue issue.
As Indonesia pushes forward with its COVID-19 vaccine rollout, the nation faces substantial obstacles. Trying to administer vaccines to an archipelagic population of 260 million people spread over 6000 islands is no small task. But logistics and resources aside, Indonesia is facing a further hurdle: vaccine hesitancy.
In January 2021 polls suggested that 27 percent of Indonesians were hesitant to receive the vaccine; this hesitancy rate has risen to around 30-40 percent (https://saifulmujani.com/kepercayaan-publik-nasional-pada-vaksin-dan-vaksinasi-COVID-19/)
What is behind this vaccine hesitancy? To uncover the reasons, we conducted on-the-ground research in Sumatra, interviewing 50 women in the first few months of 2021 who had key vulnerabilities: 20 of these women were living with HIV; 20 were pregnant during the last 12 months; and 10 were front line health workers.
Our interviews revealed four key factors behind vaccine hesitancy: concern that the vaccine is not halal (permissible in Islam); fears over Sinovac as it comes from China (and has imagined links with Communist contagion); vaccine coercion; and belief in alternative ways of safely and effectively guarding against COVID-19 such as good hygiene practices.
The vaccine is not halal
I do not want to be vaccinated because the vaccine is from China, and there are pig parts in the ingredients. It is haram (forbidden) to put pig parts into my body. We will go to hell if we do it. (Yaya, a 50-year-old housewife) (all names are pseudonyms)
Indonesia has a relatively high acceptance rate of regular immunisation regimes. Indeed, around 80 to 90 percent of all babies under the age of one receive immunisations. Mothers we talked to noted that prior to COVID they would travel some distance and stand in long lines at public health centres to ensure their babies were fully immunised. This account suggests that Indonesia is a vaccine-accepting country. Furthermore, the current MMR (measles, mumps, and rubella) vaccine is made in India and is widely suspected to contain pig products. Yet there has been no large-scale refusal of this vaccine in Indonesia, despite it not being certified halal.
But there is heated debate in Indonesia currently around the Sinovac vaccination, which is the main vaccine administered in Indonesia at the moment for COVID-19. Sinovac was developed by Chinese biopharmaceutical company Sinovac and is now made in partnership with Indonesian state-owned pharmaceutical firm PT Bio Farma. While AstraZeneca, Novavax and Pfizer have publicly stated that there are no pork products in their vaccines, Sinovac has refused to reveal whether its vaccine contains any pork products.
Given Indonesia is home to the largest population of Muslims in the world, not being able to confirm the halal status of the vaccine worries many. This worry persists despite Vice President Ma’ruf Amin, an influential Muslim leader, declaring that in emergencies such as a global pandemic, the vaccine does not need to be certified as halal to be permissible. But fear continues, and it continues despite other widely accepted vaccines (e.g. MMR) not being declared halal. We suggest, therefore, that it is not halal status on its own that is provoking vaccine hesitancy. Hesitancy is also due to the fact that there is suspicion of China.
Fear of Sinovac and China (and imagined links with Communism)
As far as I know, China bought vaccines from Europe, and Indonesia bought vaccines from China. Think about it! (Nay, 33-year-old working mother)
Part of the reason for vaccine hesitancy is that people are not convinced that the Sinovac vaccine is effective. As Nay suggests above, consumers are suspicious of why China would import a vaccine from Europe if their domestically produced one was effective.
But hesitancy also comes from a general distrust of China, including health products made by Chinese companies. This distrust extends from Indonesia’s long standing tension with Communism, which continues to be banned in Indonesia. Rumours thus circulate that China might be waging a proxy war against Indonesia by delivering a vaccine that might have fatal consequences.
Further, women told us they felt China was pushing a vaccine (of dubious efficacy and with potentially deleterious side effects) just to make money. This again taps into harmful stereotypes in Indonesia that Chinese businesses want to make a profit at any cost. Added to this profit discourse is the widespread belief that people from mainland China are coming to Indonesia to take away local jobs. There is thus a kind of grass-roots collective resistance against China and Chinese products, including vaccines, as Nika, a 29-year-old mother summarises:
The efficacy of the vaccines has not been proven with evidence. It could turn out to be medical malpractice. We hesitate then to take the vaccine and wonder if it is a vaccine or if it’s just vitamins. And where did the virus come from? And where is the vaccine made? Both in China! So maybe COVID-19 vaccines are just made for economic reasons to benefit China. China, you know, they are Communists. We have become experimental subjects, yes, guinea pigs (kelinci percobaan, literally test rabbits). For me, it is better to maintain our health, trust our body, and if we can maintain our health, then what is the COVID-19 vaccine for?
Vaccine hesitancy also stems from public distrust of the Indonesian government, which many people see as being too close with China. For instance, women noted that the government has not raised the issue of Sinovac needing to pass clinical trials and have its efficacy proven. Women mentioned that the Sinovac vaccine had not (according to their understanding) passed the Stage III Clinical Trial and they noted that the government had not transparently explained this. Women thus worried that the vaccine was not safe because it was only approved through an emergency permit granted by Indonesia’s Drug and Beverage Regulatory Agency. There is thus palpable suspicion of the vaccine in Indonesia and when this suspicion is met with a coercive vaccination program, you have a recipe for vaccine hesitancy.
Vaccine coercion
From early January 2021, there was rampant social media messaging saying “I am ready to be vaccinated.” ] Such posts were shared by community health centres, hospitals and public health departments, healthcare organisations, and health workers themselves. There was hope that people would get vaccinated in good faith.
But shortly thereafter the government imposed the threat of fines of up to Rp 5 million (AUD$450) for people who refused the vaccine or who spread anti-vaccine messages (https://www.abc.net.au/news/2021-02-19/indonesia-warns-fines-for-refusing-COVID-19-vaccine-world-first/13170826). These fines were particularly aimed as health care workers and teachers, who were first in line for mandatory COVID-19 vaccines. Presidential Decree Number 14 of 2021, verse 13A, point 4, states:
Anyone designated as a core target for the vaccine, and who refuses the vaccine, will face an administrative sanction, including postponing or stopping social aid, postponing, or stopping administrative government services; and/or a fine (https://jdih.setkab.go.id/PUUdoc/176339/Salinan_Perpres_Nomor_14_Tahun_2021.pdf)
The coercive nature of the vaccine rollout has put many Indonesians offside, as Ati, a 30-year-old nutritionist, revealed: “We cannot reject the vaccination for COVID-19. Thirty of my friends refused the vaccine on health grounds and they were interviewed by staff from the Ministry of Health and the Public Health Office. After the interview, 28 were compelled to be vaccinated; only two had their wishes not to be vaccinated upheld.”
The coercion to be vaccinated has concrete implications, as Hana, a 35-year-old woman who works in a public hospital noted: “From the bottom of my heart, I did not want to get the COVID-19 vaccine. However, we would lose our job if we did not get the COVID-19 vaccination.”
Lala, a 30-year-old nurse, also mentioned that as a health worker she was obliged to get vaccinated and that her only choice was to agree to the vaccine or to lose her job. Lala also noted: “We are also afraid of accessing the COVID-19 vaccination. We are ordinary humans, we are afraid of taking the COVID-19 vaccine, but we need to take care of our own health.”
Part of the reason that people do not trust the Indonesian government in terms of the COVID-19 response, is that health messages have been unclear and caused confusion. One of the impacts of a lack of trust in the government is that women are now deciding not to bring their children in for regular immunisations, such as for measles. Yana, a 24-year-old mother said: “I decided not to immunise my second baby, who was born during this pandemic. I am afraid that the baby will not be given the regular immunisation, and I thought my child might be given the COVID-19 vaccine. For my older children who are school age, I will ask whether they will be vaccinated for COVID-19. If they tell me the children will be vaccinated for COVID-19, I will reject it for my children.”
Belief in harmful side-effects and alternative ways of guarding against COVID-19
Some women noted that they did not want the vaccine because they were worried about adverse side effects, which were heightened among women who had comorbidities. Kanya, an HIV-positive mother told us: “I do not want to get vaccinated as I do not want to take any risks. I have asthma and HIV. I am afraid of disclosing my HIV status.” Others mentioned feared an allergic reaction. Some of the women noted disbelief that COVID-19 is real, or at least belief that COVID-19 poses no real health risk. For instance, Diah, a 29-year-old small shop owner noted: “People surrounding me did not believe in COVID-19, how come they want to access COVID-19 vaccines” (see also http://intersections.anu.edu.au/issue45/najmah2.html).
Worry and disbelief play into the promotion of alternative ways of guarding against COVID-19. Some women talked about alternative ways of protecting themselves. For instance, Anti, a 49-year-old housewife said: “I do not want to take any risk [by having the vaccine]. I feel healthy and I am in a good condition. I just need to perform the health protocols [e.g. hand-washing] and maintain my immunity by taking vitamins. I also need to maintain my health by eating nutritional food. If I feel sick and suffer from COVID-19 symptoms, I just need to take vitamins and have a rest at home, it is easier [than getting vaccinated].”
Figure 2: Mapping reasons women reject COVID-19. Source: Najmah (supplied by author)
Indonesia has a long way to go to gain public trust in its handling of COVID-19. There is little evidence that the government has implemented a national health solution, instead stoking public distrust through inconsistency and lack of transparency. To mitigate this doubt, the government should look to scientific evidence and effective communication, rather than coercive power and religious doctrine.
On a sunny April morning in Philadelphia, Tifrah Akhtar was racing the clock to pick up a rushed-printed sign. Her sign read, in bold letters: “President Biden, Do What You Promised and #FREETHEVACCINE.”
Less than 72 hours before, Akhtar had heard President Biden was coming to Philadelphia to speak at an Amtrak station. She’d seen an opportunity, and with help from her six organizer roommates and community organizations like Reclaim Philadelphia, Vietlead, and others, word spread. Approximately 70 people rallied that day to ask President Biden why he was not upholding his campaign promise to relax or cancel coronavirus vaccine patents for global distribution.
“We knew we had to act really fast,” said Akhtar. Akhtar, whose family is from Pakistan, has relatives both abroad and locally who are or have been sick with COVID-19. But while the vaccine is now readily available in Philadelphia, she says her cousins in Pakistan have no dream of getting the vaccine at present.
“I’m afraid every day, glued to the family group chat and wondering what is next,” she said. “Here in Philly I just read that 400 vaccines were thrown out. This is a huge injustice.”
Akhtar is part of a movement worldwide calling for a “People’s Vaccine” — an emergency waiver by the World Trade Organization (WTO) that would open up the patents for COVID-19 vaccines so more countries could manufacture them. The movement saw a major victory on May 5 when, after months of stonewalling, the Biden administrationannounced support of the waiver of intellectual property rights.
It took direct action, open letters, engagement with local, state, and federal civil servants and an incredible cross-pollination of community organizers from public health, international solidarity, and trade justice campaigns to generate the roar of public pressure that the administration could not ignore. And yet, the fight is far from over.
“Could You Patent the Sun?”
Major advances in public health have often been brought about by public and private collaboration and funding, including with philanthropic support.
In 1955, the medical breakthrough of the vaccine for polio, which used to paralyze or kill thousands of children annually, brought a global sigh of relief. The research that led to the discovery of the vaccine by American virologist Jonas Salk was collectively funded by 80 million individuals.
When asked in an interview who owned the patent to the vaccine, Salk replied, “the people.”
“There is no patent,” Salk stated. “Could you patent the sun?” The vaccine was deemed to have been funded by the people and therefore part of the medical commons, he was saying.
But by the mid-90s, with the dawn of the World Trade Organization and a fully entrenched neoliberal economic framework, views on intellectual proprietary ownership of vaccines had become more rigid.
“This is a fight that has happened before over the decades,” said Arthur Stamoulis, executive director of Citizens Trade Campaign.
After years of activism and research, for example, functional medication for HIV/AIDS offered hope of an end to that crisis. But those drugs were only accessible to individuals — and countries — who could pay for them. For nearly a decade, entire countries couldn’t access the drugs because of intellectual property controls enforced by the WTO.
Citizens Trade Campaign, a national coalition of environmental, labor, consumer, family farm, religious, and other civil society groups that work on trade justice campaigns, were part of the fight to make HIV/AIDS medication accessible to the world.
“There was a lot of activism directed at Clinton, Gore, and George W. Bush, and there was an agreement within the WTO that said in emergency situations countries do have the right to waive intellectual property rights,” said Stamoulis. “It didn’t happen overnight, but it happened eventually.”
The Fight for a People’s COVID Vaccine
In October 2020, India and South Africa proposed a temporary TRIPS (Trade-Related Aspects of Intellectual Property) waiver of the patent rights for COVID-19 vaccines. This waiver, ifpassed in a consensusvote by all 164 WTO member countries, would allow for countries to manufacture a generic version of the vaccine at scale, without fear of legal repercussions.
More than 100 nations, most of them poorer, have supported the waiver, but several rich governmental bodies, including the EU, the United Kingdom, New Zealand, Australia — and until May 5, the United States — blocked it.
“COVID vaccines were developed with broad public support, and everyone worldwide deserves access to them,” said Arthur Stamoulis, executive director of Citizens Trade Campaign. Massive infusions of taxpayer money — the whopping $18 billion Operation Warp Speed — lowered the risk to pharmaceutical companies to enter the vaccine race in 2020, ultimately bringing several successful vaccines to market.
And while this breakthrough is one of overwhelming relief, worldwide vaccinations to date are cut starkly along lines of nationality and wealth. One in four citizens of rich nations have received a vaccine, but only one in 500 people in poorer countries can say the same,World Health Organization Director-General Tedros Adhanom Ghebreyesussaid in a recent meeting of the United Nations’ Economic and Social Council.
Citizens Trade Campaign is still in the fight. In February 2021, the organization publishedan open letterto President Biden in support of the TRIPS Waiver, signed by 400+ organizations.
“Defending monopoly protection is the antithesis to the current call for COVID-19 medicines and vaccines to be treated as global public goods,” said Yuanqiong Hu, policy co-coordinator for Doctors Without Borders’ Access Campaign, in a statement on the signing. “In these unprecedented times, governments should act together in the interest of all people everywhere.”
But even with more than 400 groups representing tens of millions of members, the Citizens Trade Campaign letter was little more than a blip in the national news. The patent waiver faced strong opposition by pharmaceutical companies such as Pfizer and Moderna, as well as from the Bill & Melinda Gates Foundation.Bill Gates had previously been against the waiver, saying that the profit incentive from licensing the vaccine is what has driven the innovation to create the vaccine. But on May 6, the Gates Foundation reversed course andannounced support for a limited waiver.
On April 22, protesters outside the Pfizer shareholder meeting in New York City held up a 7-foot-long needle. That action, says Ben Levenson, an organizer with Justice is Global, was driven by longtime HIV/AIDS advocates. A parallel protest happened outside the Moderna shareholder meeting on April 28.
Over the next two weeks, on-the-ground protests, rallies, postcard campaigns, and digital organizing have targeted the Biden administration, Congress members, Big Pharma companies, and the Gates Foundation.
“It’s a really beautiful moment for international solidarity,” said Hillary Haden, executive director of the Washington Fair Trade Coalition. Haden is part of a large informal coalition including groups like Citizens Trade Campaign, Peoples Health Movement, Global Trade Watch, Fair World Project, Justice is Global, and others that began working on the patent issue in December.
One speaker at an April 30 rally in Seattle was Hassan Khan, a tech worker, human rights advocate, and volunteer with the Coalition for Seattle Indian Americans, who recently lost a 38-year old cousin in India to COVID-19. There, the virus has inundated the country’s health care system in a matter of weeks. Booming case loads, spurred on by a new, fast-spreading variant, have overwhelmed hospitals and communities, with no end in sight.
“When humanity is at stake, we must lower the barriers that are erected to protect the margin of rich pharma companies,” Khan told a crowd at the “Rally to Demand Biden and the Billionaires End Vaccine Apartheid!” which was held outside the offices of the Bill & Melinda Gates Foundation.
“Money is not everything,” said Khan. “People’s lives are what matters.”
Beyond moral arguments of addressing medical apartheid, vaccinating the world is ultimately what is required to end the pandemic, proponents of the TRIPS waiver say. The longer the pandemic, the more opportunity there is for dangerous new variants to emerge, like the B.1.617 “double mutant” variant whichcould be more resistant to vaccines.
New alliances forged through the shared vision for vaccine access have given this movement some momentum. The trade coalition co-organized the rally with the Coalition of Seattle Indian Americans and other groups, and also worked with Seattle City Councilmember Kshama Sawant on a resolution in support of the waiver — the first of its kind in the country.
Stamoulis at the Citizens Trade Campaign was surprised at how quickly the movement gained steam. “It’s a testament to the power of cross-sector, cross-border organizing.”
Biden’s support of the TRIPS waiver is a clear victory for the movement, because of the prominent role the United States has in driving WTO agendas. Still, the next phase will require continued pressure, as the exact parameters of the waiver are negotiated — a process which could take months.
“Our hope is that other opponents of the waiver quickly lift their blocks against it,” Stamoulis said. “Our movements need to continue pressing for a speedy and robust waiver deal, as well as follow through by the administration on financing, info sharing and other production support.”
In Seattle, in front of the doors to the Gates Foundation, a woman came up to the mic with her parai drum, a traditional instrument in India, often associated with grief and resistance.
“‘Parai’ means ‘say,’” she told the crowd, before beginning to play. “Say it out loud. Say it until you are heard.”
Black Americans’ COVID-19 vaccination rates are still lagging months into the nation’s campaign, while Hispanics are closing the gap and Native Americans show the highest rates overall, according to federal data obtained by KHN.
The data, provided by the Centers for Disease Control and Prevention in response to a public records request, gives a sweeping national look at the race and ethnicity of vaccinated people on a state-by-state basis. Yet nearly half of those vaccination records are missing race or ethnicity information.
KHN’s analysis shows that only 22% of Black Americans have gotten a shot, and Black rates still trail those of whites in almost every state.
Targeted efforts have raised vaccination rates among other minority groups. Hispanics in eight states, the District of Columbia and Puerto Rico are now vaccinated at higher rates than non-Hispanic whites. Yet 29% of Hispanics are vaccinated nationally, compared with 33% of whites.
While 45% of Native Americans have received at least one dose, stark differences exist depending on where they live. And Asian vaccination rates are high in most states, with 41% getting a shot.
The analysis underscores howvaccine disparitieshave improved as availability has opened up and Biden administration officials have attempted to prioritize equitable distribution. Still, gaps persist even as minority groups have suffered muchhigher mortality ratesfrom the pandemic than whites and are at risk of infection as states move to reopen and lift mask mandates.
Despite these lingering gaps, the CDC said last week that those who are fully vaccinated don’t need to wear masks in most indoor and outdoor settings or physically distance. Only 38% of Americans arefully vaccinated.
“Every day we do not reach a person or a community is a day in which there is a preventable covid case that happens and a preventable covid death in these communities,” said Dr.Kirsten Bibbins-Domingo, chair of the Department of Epidemiology and Biostatistics at the University of California-San Francisco.
KHN requested race and ethnicity data from the CDC on people who have received at least one dose of a covid vaccine since mid-December for all 50 states, the District of Columbia and Puerto Rico. The data covers shots as of May 14 given to 155 million people that were administered through federally run programs and federal agencies as well as by state and local authorities.
Eight states — Alabama, California, Michigan, Minnesota, South Dakota, Texas, Vermont and Wyoming — either refuse to provide race and ethnicity details to the CDC or are missing that information for more than 60% of people vaccinated. Those states are excluded from the KHN analysis, though the CDC includes all but Texas in itspublished national rates.
Some states display race and ethnicity for vaccine recipients separately, making it difficult to compare rates for Hispanics to non-Hispanic whites, for example. But the CDC data allows for direct comparisons. It reports numbers for Hispanics, who can be of any race or combination of races, as well as numbers for non-Hispanic people of single-race or multiracial categories.
The data for Native Hawaiians and other Pacific Islanders is unreliable, making it difficult to draw conclusions on the vaccination rate in that population.
Dr.Georges Benjamin, executive director of the American Public Health Association, wasn’t surprised that Black Americans’ vaccination rates werestill lagging, citing a complex combination of access issues, hesitancy and structural inequity.
Benjamin pointed to the early challenges in securing an appointment online and the initial placement of vaccination sites — which he noted the Biden administration had worked to improve.
“We’re going to be judged whether or not we did it equitably at the end of the day,” he said. “Right now, I still think we’re failing.”
Dr.Utibe Essien, a health equity researcher and assistant professor of medicine at the University of Pittsburgh, stressed that targeted outreach must involve multiple institutions in a community.
“It’s not just the Black doctor, it’s not just the barber, it’s not just the pastor, kind of these traditional folks who have been the big messengers. We have to be broad,” he said. “It’s investing in folks who know the neighborhood, the small-store owner who gets to see all the 12- to 15-year-old kids come through the store getting snacks before they head off to school.”
Why Native Americans Lead in Vaccinations
Nationally, Native Americans and Alaska Natives have been vaccinated at significantly higher rates than other groups. Tribes administered doses quickly, prioritizing elders with culturally important knowledge, saidMeredith Raimondi, director of congressional relations and public policy for the National Council of Urban Indian Health. The rollout was imbued with urgency: Native Americans have died of covid at more than double the rate of white Americans, according to thelatest CDC data.
Native vaccination rates are higher than white rates in 28 states, including New Mexico, Arizona and Alaska, where many receive care from tribal health centers and the Indian Health Service. In states such as South Carolina and Tennessee, where IHS access ismore limitedand Native residents are more likely to live in urban areas, vaccination rates are far lower than for white residents.
Groups in those areas reported problems finding health care providers to administer shots. Tribal organizations compiled lists of retired nurses to tap for clinics. At one point, staffers from an Oklahoma City clinic for Native Americans offered to fly to Washington, D.C., to help vaccinate Indigenous people living around the nation’s capital, Raimondi said.
“It became an issue of, ‘Well, we could get you the vaccine, but we don’t know who is going to administer them,’” Raimondi said.
The council and Native American Lifelines, a nonprofit providing health services, partnered with the University of Maryland-Baltimore for a vaccination site exclusively for Native Americans living in Maryland, Virginia and Washington, D.C. It launched in April.
While the vaccination rates for Native Americans surpass those of whites in some states due in part to IHS, that infrastructure does not exist for Black Americans, saidRhonda BeLue, the department chair of health management policy at Saint Louis University.
At the beginning of the pandemic, people were shocked by how much more likely Black Americans were to die from covid, she said.
“However, the same structural inequities that caused that disproportionate mortality in covid are the same structural inequities that predated covid and caused disproportionate burdens of morbidity and mortality,” she said. “This isn’t new.”
Easing Fears in Hispanic Communities
Some states are reporting higher vaccination rates among Hispanics than white and Black residents, which Bibbins-Domingo said fits with surveys showinghigh enthusiasmfor vaccination among Hispanics. It also indicates that some of the reported barriers may have been addressed more effectively in those states, she said.
Paul Berry, chair of the Virginia Latino Advisory Board, partly attributes Virginia’s success to targeted outreach efforts. The state and certain counties also increased Spanish-language resources to boost sign-ups.
Connecting with every community cannot be an afterthought, saidDiego Abente, president and CEO of St. Louis’ Casa de Salud, a health care provider focused on immigrant communities. Community buy-in, effective social media use and language programming from the start have been essential, he said. Hispanics have a higher vaccination rate than whites in Missouri.
But nationally, a dearth of transportation options, an inability to take off from work to get a vaccine, and concerns about documentation and privacy have dampened uptake among Hispanics, according to experts.
“To me it’s more about access to health care,” Berry said. “If you don’t live close to health care, you’re just going to shrug it off immediately. ‘I can’t get that vaccination. I’m going to miss work.’”
To reduce fear among Idaho agricultural workers that may be part of mixed-immigration status families, public health workers emphasized messaging that documentation wouldn’t be required, saidMonica Schoch-Spana, a senior scholar at Johns Hopkins Center for Health Security. She has helped lead its CommuniVax project seeking to boost uptake among Black, Hispanic and Indigenous communities.
It’s also important to engage trusted institutions to administer vaccines, Schoch-Spana said: “Is it a familiar place, does it feel safe, and is it easy to get to?”
Federal efforts have placed sites in underserved neighborhoods. About 60% of shots at the Federal Emergency Management Agency’s vaccination sites and at community health centers were given to people of color, federal health officials said this week.
Incomplete Data Collection
Race or ethnicity information is still missing for nearly 69 million vaccinated people — or 44% — in the CDC data, despitevowsby federal officials to improve outdated systems to better inform their response.
CDC spokesperson Kate Fowlie said their efforts, including sharing strategies for capturing demographic data and reducing data gaps with state and local governments, have resulted in improvements in data collection. Officials are also planning to allow agencies to update previously submitted vaccine records. The true national rates by race or ethnicity group would each be higher with complete data.
Unlike the federal government, North Carolina made it nearly impossible for providers to submit vaccine data without recording race and ethnicity. As a result, it has the most complete demographic data of any state.
Adding that step was not an easy sell — providers and other vaccinators were initially resistant, saidKody Kinsley, the chief deputy secretary for health at the North Carolina health department. But it has paid off in the state’s ability to target its response to populations getting left behind, he said.
Bibbins-Domingo said the federal government and states need to make collecting this vaccination data by race mandatory, because data drives the response to the pandemic.
“The feds know how to do this. They do it every 10 years for the census,” she said. “That we somehow cannot figure it out in public health data is quite simply unacceptable.”
KHN reporter Victoria Knight contributed to this report.Targeted efforts have raised vaccination rates among other minority groups.
Ten percent of Papua New Guineans confirmed to have been infected with covid-19 are health workers, while the death toll from the pandemic has jumped sharply to 154.
The number of confirmed cases of the virus in PNG continues to climb at a worrying rate, with the Pandemic Response Controller reporting 569 new cases in a 48-hour period ending midday on Wednesday.
This increases the total number of cases to 14,910, of whom the Controller, David Manning, said 1499 were health workers.
“This is a serious cause for concern. Health workers are in the front line of this fight against covid-19 and they must be protected at all cost,” he said.
“However, statistics again show that health workers again make up for about ten per cent of those vaccinated thus far.”
According to Manning’s office, as of Tuesday a total of 16,459 people had received their first dose of the AstraZeneca covid-19 vaccine. The majority are essential workers, including 3618 health workers.
By province, the National Capital District still has the highest number of people vaccinated with 8199, followed by Morobe with 1874.
Vaccine hesitancy significant
Seventeen provinces have rolled out their vaccination programmes with the remaining five set to begin theirs as well.
Vaccine hesitancy is significant among PNG’s public, including health workers, especially nurses, increasing pressure on a health system under massive strain due to covid.
“It is optional but I am appealing to the health workers around the country to take the shot immediately. Protect yourself first so that you can then effectively defend your country from this unseen enemy,” Manning said.
As well as hundreds of new confirmed cases, the Controller reported 15 new deaths over the last two daily updates.
The total number of deaths is now at 154.
This article is republished under a community partnership agreement with RNZ.
Seventeen PNG provinces have rolled out their vaccination programmes with the remaining five set to begin theirs as well. Image: AFP/RNZ
Timor-Leste today registered 172 more cases of covid-19 infection with the majority in Dili – passing the barrier of 5000 cases since the beginning of the pandemic.
On the day that the country celebrated 19 years of the restoration of independence, the Integrated Crisis Management Center (CIGC) announced 126 more cases in Dili, 11 in Manatuto, 10 in Bobonaro, eight in Baucau, five in Viqueque, three in Ermera and one in Ainaro.
With the recovery of 76, the country now has 2398 active cases and 5121 cases accumulated since the beginning of the pandemic.
About 10 percent of the cases recorded in the last 24 hours had symptoms of covid-19, with positive cases in Dili representing 13.1 percent of the 964 tests performed in the capital and almost 7 percent of the 662 tests recorded outside the capital.
The infection incidence rate is set at 13.4/100,000 inhabitants outside Dili and at 40.6/100,000 inhabitants in Dili.
The number of cases in the Vera Cruz isolation center has increased to 37, of which four are in serious condition.
Antonio Sampaio is the Lusa News Agency correspondent in Dili and this article is republished in community partnership.
The chair of the board of French Polynesia’s social security agency CPS has called on the French state to pay for the medical costs caused by its nuclear weapons tests.
Patrick Galenon, who is also a leading trade unionist, has written to the French Overseas Minister Sebastien Lecornu as France plans a high-level roundtable in Paris next month on the legacy of the nuclear weapons tests in the South Pacific.
Galenon said that since 1995 the CPS had paid out US$800 million to treat a total of 10,000 people suffering from any of the 23 cancers recognised by law as being the result of radiation.
Patrick Galenon, chair of the board of French Polynesia’s social security agency CPS … France’s liability needs to be anchored in law. Image: Tahiti Infos
A 2010 French law recognised for the first time that the nuclear tests were not clean but compensation to successful claimants was only made on the basis of national solidarity, not because the French state recognised any liability.
Galenon said France’s liability had to be anchored in law as the rest was just sentimentality and politics.
He said France should also assume paying for ongoing oncology services, which cost the CPS more than US$50 million a year.
Between 1966 and 1996, France carried out 193 nuclear weapons tests in French Polynesia.
The test sites of Moruroa and Fangataufa remain excised from French Polynesia and are French no-go zones.
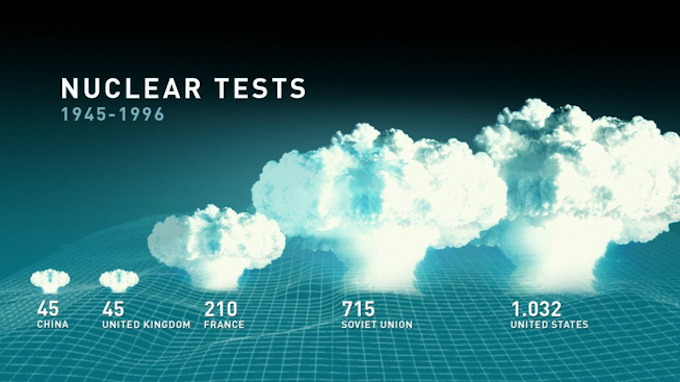
More than 2000 nuclear tests have been conducted since the first American test, Trinity, in 1945, according to the Swedish Physicians against Nuclear Weapons. More than 500 tests have been done in the atmosphere, under water or in space. The rest have been tested underground.The US is responsible for around 1000 of these tests, the Soviet Union conducted about 700, France 210 (including 17 in Algeria), China 35 and the UK about 30 tests. India has conducted six tests, Pakistan five and North Korea one nuclear test.
Major global nuclear testing nations. Graphic: Laromkarnvapen
Fiji has recorded its second death from the current outbreak of covid-19 while reporting four more new positive cases – three of them administration staff of the Fiji Centre for Disease Control (CDC).
The death is of a woman from the recent Makoi cluster who was entered into intensive care last night after her condition rapidly deteriorated.
Health Secretary Dr James Fong said the woman’s family had been informed of her death before the national announcement tonight.
The first of the four new cases is from Makoi and presented to Oceania Hospital with symptoms.
“At this early stage of the investigation, this case has no known links to other cases,” Dr Fong said.
“The Oceania Hospital outpatients department was temporarily closed yesterday for contact tracing and decontamination. Anyone who potentially had contact with this case at the hospital has been quarantined.”
The second case is also from Makoi and he is an administration staff member of the Fiji CDC.
Tested after annual leave
Dr Fong said that according to Fiji CDC protocol the man was tested after returning this week from annual leave.
He said the next two cases were also administrative staff at the Fiji CDC who had tested negative during routine testing earlier this week but tested positive as part of contact tracing for this new case.
He added that the three staff members who had tested positive for the virus had been transferred to isolation facilities.
“Our investigations so far indicate that this cluster originated outside of the Fiji CDC and the virus was then brought in – as would be an expected consequence of community transmission,” Dr Fong said.
“Apart from these three cases, all other Fiji CDC staff have tested negative so far, including all of the laboratory and medical staff in the centre.”
Given the rapidly rising number of contacts stemming from new Fiji cases of covid-19 in the Suva-Nausori area, a full lockdown that was announced yesterday by Health Secretary Dr James Fong has been extended to 4am next Wednesday, May 19.
This has been confirmed in a statement by the Ministry of Health and Medical Services.
Dr Fong had announced last night that a full lockdown of Suva and Nausori would commence from Friday night at 11pm until Tuesday morning at 4am to enable widespread contact tracing.
The ministry has advised Fijians living in the Suva and Nausori containment areas to prepare for an all-day stay-at-home order that will remain in force from tomorrow evening at 11pm until Wednesday morning at 4am.
“As stated yesterday, food rations will be available during the later stages of the lockdown period for Fijians living within the Suva-Nausori lockdown zone who have a genuine need for an emergency food supply.”
The total number of community cases now stands at 44, as an outbreak of the B1617 (Indian) variant of the virus prompted the government to announce the lockdown.
It is in this area that the government said it expected to have “many” more cases recorded in the coming days.
As the government works to trace infections from an outbreak at a large supermarket in Flagstaff, near the capital Suva, health authorities have admitted they may not have employed the best communications strategies in this second wave of the virus.
The government has in recent weeks conducted once daily updates, sometimes starting close to 10pm.
“We do need to improve our communication strategy. That is something that I for one will be working on, that I’ve been working on with a few others,” Dr Fong said.
“We have put a plan together and we have thought about it. It’s just that when we can implement it, is the issue that we will have to work with
There was a delicate balance between ensuring that he had all the information that he needed to share, and that what he shared was accurate and at the right time, Dr Fong said.
Admitting the public information campaign part of the government’s response had not been easy to implement, Dr Fong said the team he headed would need to segregate “between the team that’s driving the response and the overseeing of the response, and the team that’s driving the narrative”.
Fijians have been advised to remain calm as “ample notice” will be given should a situation in Fiji warrant a total lockdown of Viti Levu, reports The Fiji Times.
Health Secretary Dr James Fong issued this assurance last night as he announced 12 new covid-19 cases.
RNZ’s correspondent in Suva, Lice Movono, said: “That tells us that people are still moving in and out of each other’s homes, people are not maintaining any sort of bubble.”
Movements of the 12 cases in the past few days included trips to supermarkets in Suva’s central city more than 30 minutes drive away from their suburb.
Fiji now has 48 active cases, 35 of them locally transmitted, and seven in border quarantine, while the source of six cases is under investigation.
Struggling families In an editorial titled “Reflections”, the newspaper said:
Let’s reflect on some things we probably take for granted.
Not too many people realise the impact of the covid-19 pandemic on Fijians until they see things for themselves.
It’s difficult to appreciate this when you are far removed from the hardship thousands of Fijians are forced to live with.
Now take for instance the fact that there are no jobs for carrier drivers in Nadi Town. It’s probably not going to ruffle feathers so to speak, unless you are one of those directly or indirectly impacted.
Today’s Fiji Times “Remain calm” front page. Image: Fiji Times screenshot
The assistant secretary of the carrier stand in Nadi, Mohammed Naseeb said the situation “is really bad”.
To drive his point through, he points out there are 167 carrier drivers who operate out of the base.
There are now only 20 to 30 drivers turning up every day, scratching around for jobs. It’s a nightmare!
Mr Naseeb returned to the base after three weeks.
Now consider the fact a lot of these drivers took out loans to buy their vehicles.
Now slap in the fact there is no business, and they are left with a massive burden on their shoulders.
Now throw in the need for them to put food on their table, mouths to feed, rent or mortgage to pay, and medical expenses to meet, and you are left with an unpleasant scenario.
The Mulomulo, Nadi man said most of their customers were farmers coming from the interiors such as Nanoko, Natawa, Nagado, however, those farmers were no longer selling their produce at the market. Now consider that segment of impacted people!
A little over 21km away, in Lautoka, a non-governmental organisation (NGO) Grog Masters distributed grocery packs to at least 200 families in Lautoka during the lockdown phase.
Its president, Amol Kumar said it was important to fight this battle together and struggling families should not be abandoned at this time.
Now, by this morning, [the Fiji] government had paid out $4.3 million through the $90 assistance programme to more than 48,000 households.
The Timor-Leste health authorities have registered a total of 126 new infections with SARS-CoV-2 in the last 24 hours, almost all in the Timorese capital, according to official data.
The data was released in a statement from the Integrated Crisis Management Center (CIGC), which states that in addition to 120 cases in Dili, three more cases were registered in Baucau and another in Covalima.
This consolidates the three regions with the highest prevalence of the virus.
With the new cases, and the record of 82 recovered cases, the number of active infections is currently 1584. The total accumulated since March 2020 has risen to 3353.
The positive cases detected in Dili represent 16.7 percent of the 719 tests carried out – one of the highest percentages ever.
The incidence rate is now 8.5/100,000 inhabitants in Dili and 27.8/100,000 inhabitants, the highest ever. The country’s population is 1.3 million.
In the Vera Cruz isolation center there are now 37 people, of which one is in a serious condition and 36 are moderate.
However, sources from the Ministry of Health confirmed to Lusa News Agency that dozens of cases of infection with SARS-CoV-2 have been detected in recent weeks in various institutions of the Timorese state, including the Presidency of the Republic, Parliament and the government.
The sources explained to Lusa that at least 40 positive results were detected in screenings carried out last week in the Presidency of the Republic.
There are also about two dozen cases detected in the National Parliament and several other cases in ministries and public institutions, the same sources confirmed.
Antonio Sampaiois the bureau chief of Lusa News Agency in Dili. This article is republished with permission.
The Timor-Leste health authorities have registered a total of 126 new infections with SARS-CoV-2 in the last 24 hours, almost all in the Timorese capital, according to official data.
The data was released in a statement from the Integrated Crisis Management Center (CIGC), which states that in addition to 120 cases in Dili, three more cases were registered in Baucau and another in Covalima.
This consolidates the three regions with the highest prevalence of the virus.
With the new cases, and the record of 82 recovered cases, the number of active infections is currently 1584. The total accumulated since March 2020 has risen to 3353.
The positive cases detected in Dili represent 16.7 percent of the 719 tests carried out – one of the highest percentages ever.
The incidence rate is now 8.5/100,000 inhabitants in Dili and 27.8/100,000 inhabitants, the highest ever. The country’s population is 1.3 million.
In the Vera Cruz isolation center there are now 37 people, of which one is in a serious condition and 36 are moderate.
However, sources from the Ministry of Health confirmed to Lusa News Agency that dozens of cases of infection with SARS-CoV-2 have been detected in recent weeks in various institutions of the Timorese state, including the Presidency of the Republic, Parliament and the government.
The sources explained to Lusa that at least 40 positive results were detected in screenings carried out last week in the Presidency of the Republic.
There are also about two dozen cases detected in the National Parliament and several other cases in ministries and public institutions, the same sources confirmed.
Antonio Sampaiois the bureau chief of Lusa News Agency in Dili. This article is republished with permission.
A covid-19 vaccine from French company Valneva has yet to complete clinical trials. But it has caught the eye of governments in the UK, Europe and Australia.
One of the vaccine’s main selling points is its apparent ability to mount a more general immune response against SARS-CoV-2, the virus that causes covid-19, rather than rely on the spike protein to do this.
This means the vaccine is more likely to be effective against the type of virus variants that have already been emerging, and may emerge in the future. Some reports describe it as “variant proof”.
The hope is vaccines using this technology would be able to provide protection for longer, rather than keep being reformulated to get ahead of these new variants.
How does Valneva work? Valneva’s vaccine, called VLA2001, is based on tried and tested vaccine technology. It is the technology used in the vaccine against poliovirus and in some types of flu vaccines. And the company already has a commercially available Japanese encephalitis vaccine based on the same technology.
This type of inactivation is expected to preserve the structure of the viral proteins, as they would occur in nature. This means the immune system will be presented with something similar to what occurs naturally, and mount a strong immune response.
After being inactivated, the vaccine would be highly purified. Then, an adjuvant (an immune stimulant) is added to induce a strong immune response.
VLA2001 isn’t the first inactivated vaccine against covid-19. Leading covid-19 inactivated vaccines, such as those developed by Sinopharm and Bharat Biotech, have been approved for use in China and received emergency approval in other countries, including India.
However, VLA2001 is the only covid-19 vaccine candidate using whole inactivated virus in clinical trials in the UK and in mainland Europe.
What are the benefits known so far? This approach to vaccine development presents the immune system with all of the structural components of the SARS-CoV-2 virus, not just the spike protein, as many other covid-19 vaccines do.
So Valneva’s vaccine is thought to produce a more broadly protective immune response. That is, antibodies and cells of the immune system are able to recognise and neutralise more pieces of the virus than just the spike protein.
The federal government is speaking with a French company about potentially importing its vaccine to use in the Australian rollout.https://t.co/8OXapOauE4
As a result, Valneva’s vaccine could be more effective at tackling emerging covid-19 virus variants and, if approved, play a useful role as a booster vaccine.
How about results from clinical trials? According tothe company, no safety concerns or serious adverse events were associated with VLA2001 in early-stage clinical trials.
VLA2001 was given as a low, medium or high dose in these trials with all participants in the high-dose group generating antibodies to the virus spike protein.
One measure of immune response in the high-dose group after completing the two doses indicated antibody levels were, after two weeks, at least as high as those seen in patients naturally infected with SARS-CoV-2.
Interestingly, VLA2001 induced immune responses against a number of virus proteins (including the spike protein) across all participants, an encouraging sign the vaccine can provide broad protection against covid-19.
We’re looking for volunteers for the latest UK COVID-19 vaccine study.
The Valneva phase 2/3 study is open to healthy adults who have not had a previous COVID-19 vaccine.
The phase 3 trial is expected to be completed by the northern hemisphere’s autumn this year. And if successful, would be submitted for regulatory approval after that.
Who is interested?
Despite phase 3 clinical trials only just starting, the UK government has pre-ordered more than 100 million doses of the vaccine from Valneva, with the option of buying more down the track. If trials prove successful and pass regulatory approval, this means the vaccine could be used as a booster in time for this year’s northern hemisphere’s winter.
Australia has confirmed it’s also in talks with Valeneva about importing the vaccine. Some countries in Europe are also reportedly keen to strike a deal.
As new cases of covid-19 increase globally, we’ll continue to see new viral variants emerge that threaten to escape the protection existing vaccines offer.
Already, we are seeing vaccines from companies such asModerna and Novavax begin to reformulate their spike protein-based vaccines to get ahead of emerging variants.
So Valneva’s vaccine, with the potential to elicit a more broadly protective immune response, may prove to be a useful tool to combat the rise of the virus and its mutations. However, whether the vaccine is really “variant proof” or merely less affected by emerging variants remains to be seen.
Dr Adam Taylor, is early career research leader, Emerging Viruses, Inflammation and Therapeutics Group, Menzies Health Institute Queensland, Griffith University. This article is republished from The Conversation under a Creative Commons licence. Read the original article.
Fiji has today reported seven new cases of covid-19 and all are locally transmitted cases. These were confirmed after 1349 tests.
They are in Lautoka and Nadi in the west of the main island, Viti Levu, and the settlement of Makoi, near the capital Suva.
The first is a 30-year-old woman from Field 4 in Lautoka who presented to the Kamikamica Health Centre with severe covid-19 symptoms. She had been sick for three weeks.
Health Secretary Dr James Fong said the woman had been admitted to Lautoka Hospital isolation unit and the members of her household had been quarantined.
He said this patient had some contact with medical officers and nurses within the health centre. This forced the temporary closure of the centre to members of the public earlier today.
“However, the level of exposure among our clinical staff is not as extensive as was the case for Lautoka Hospital. We expect the centre to re-open to the public following a thorough decontamination exercise,” Dr Fong said.
The second case is a 20-year-old woman who presented to the Makoi Screening clinic with covid symptoms.
Makoi family cluster
Dr Fong said investigations revealed that she had had contact with the household of the Makoi family cluster but was not identified as a contact at the time.
He said she had been entered into isolation along with her household members.
Dr Fong also confirmed that three of her household members had since tested positive for the virus.
“This case again highlights how important it is for everyone to download the careFiji app,” he said.
“Some of our recent cases have shown us just how unreliable a person’s memory can be during a contact tracing investigation – and those gaps have cost us dearly.”
The sixth case is a 26-year-old and is the husband of a previously announced local case (case 75) from Kerebula in Nadi.
Dr Fong said the man had been in quarantine facility in Nadi since April 18 and did not pose any transmission risk to the public.
The seventh case is a 35-year-old male from Saru, Lautoka, who presented with symptoms at Natabua health centre. He and his household contacts are being taken into isolation.
Fiji has today reported seven new cases of covid-19 and all are locally transmitted cases. These were confirmed after 1349 tests.
They are in Lautoka and Nadi in the west of the main island, Viti Levu, and the settlement of Makoi, near the capital Suva.
The first is a 30-year-old woman from Field 4 in Lautoka who presented to the Kamikamica Health Centre with severe covid-19 symptoms. She had been sick for three weeks.
Health Secretary Dr James Fong said the woman had been admitted to Lautoka Hospital isolation unit and the members of her household had been quarantined.
He said this patient had some contact with medical officers and nurses within the health centre. This forced the temporary closure of the centre to members of the public earlier today.
“However, the level of exposure among our clinical staff is not as extensive as was the case for Lautoka Hospital. We expect the centre to re-open to the public following a thorough decontamination exercise,” Dr Fong said.
The second case is a 20-year-old woman who presented to the Makoi Screening clinic with covid symptoms.
Makoi family cluster Dr Fong said investigations revealed that she had had contact with the household of the Makoi family cluster but was not identified as a contact at the time.
He said she had been entered into isolation along with her household members.
Dr Fong also confirmed that three of her household members had since tested positive for the virus.
“This case again highlights how important it is for everyone to download the careFiji app,” he said.
“Some of our recent cases have shown us just how unreliable a person’s memory can be during a contact tracing investigation – and those gaps have cost us dearly.”
The sixth case is a 26-year-old and is the husband of a previously announced local case (case 75) from Kerebula in Nadi.
Dr Fong said the man had been in quarantine facility in Nadi since April 18 and did not pose any transmission risk to the public.
The seventh case is a 35-year-old male from Saru, Lautoka, who presented with symptoms at Natabua health centre. He and his household contacts are being taken into isolation.
When COVID-19 was recognised as a global pandemic in 2020, we heard from many civil society actors in Cambodia who held strong fears about its potentially critical impact. They anticipated that the spread of the pandemic, in combination with people’s fear and the government’s tightened regulation, would significantly restrict the space for their campaigns and reduce their autonomy. Approximately a year since then, fear has turned into reality. If there has been any difference from what was anticipated, it is that the impact is worse than predicted.
A minimum space for activities
An immediate impact of COVID-19 has been the restriction on human mobility. Since March 2020, the government has adopted various regulations in order to control the social transmission of the virus by minimising human interaction, including the complete lockdown of Phnom Penh imposed between April and May 2021. While the impact of such restricted mobility and gathering has a negative influence on all aspects of social activities, it has had a particularly critical impact on the civil society sector whose activities were not considered essential for managing people’s livelihoods. According to a human rights organisation in Phnom Penh, almost all existing projects for human rights advocacy have stopped operating. As all inter-provincial travel requires the approval of local authorities, practitioners are no longer able to conduct meetings with local staff members; capacity building programmes, outreach programmes, and legal consultation processes in the communities have had stop. Some legal aid procedures at the court have also become stuck.
Moreover, most new proposals submitted to donor agencies are “on hold” for approval due to the uncertainty of prospects for implementation. This implies that the chance of new project initiatives in the forthcoming years is extremely narrow. For instance, ActionAid Cambodia, an international human rights advocacy NGO, has had to stop almost 70% of its projects since the outbreak of the pandemic. Cooperation Committee for Cambodia (CCC), an organisation that acts as the hub of the NGO network in the country, has struggled to maintain programmes with local NGO network members.
NGOs have sought alternative ways to carry on their activities by using online communication methods such as Zoom, Microsoft Teams, Facebook messenger, and Telegram, in order to maintain communication amongst their staff and with other stakeholders. While such new technology certainly helps, it benefits only the practitioners who can access high-quality internet and are able to use online platforms. More importantly, in the sector of human rights protection, many types of activities do require physical visits and face-to-face communication due to confidentiality issues and the need for physical paperwork. Therefore, the voices of and inputs from communities and civil society in national strategic development planning have not been heard.
Plunge in funding
The global pandemic has had a critically negative impact on the financial conditions of many NGOs. Finding no alternative way to maintain the income generating programme, a large number of small-sized local NGOs have ceased operations. This challenge is two-fold.
Firstly, the amount of funding from foreign donors is being radically reduced. For instance, one local NGO that supports the Cambodian diaspora in Vietnam confirmed that it just failed to secure funding from a donor which was previously pledged. In many cases, the communication of such decisions comes out of blue, due to challenges that donors themselves hadn’t predicted. Moreover, many local human rights advocates had to stop their overseas travel, which has previously been conducted on a regular basis in order to build and maintain working relationships with foreign donors and partners.
Secondly, many income-generation programmes operated by these NGOs, based on local community activities for mobilising operational funding, have now stopped. Programmes that relied on international tourists who visit Angkor Wat have had almost no customers for a year since May 2020 due to the international travel restriction. Moreover, programmes that targeted foreign customers have also stopped; these include Cambodian Living Arts, Phare Ponleu Selpak and Chab Dai Coalition, which had gained extra income through presentation of art performances and selling souvenirs. Other types of activities that targeted Cambodian community members were also seriously affected. For instance, an NGO that has earned on average approximately 20,000 USD per year from house rentals faces many tenants who have not been able to afford rent throughout the previous year.
It is notable that, from a short-term perspective, the impact of COVID-19 is less significant for international NGOs that maintain more stable working channels with foreign donors. Our communications with some international NGOs confirmed that their funding sources remain healthy. The EU has even increased its funding, especially for COVID-19 response and recovery. However, as most of their Cambodian partner organisations struggle with the funding crisis, these international organisations cannot operate programmes which rely on their partners’ collaboration. Moreover, from a longer-term perspective, these organisations feel unsure about the situation they will face once the pre-confirmed funding flow comes to an end.
State regulation over the civil society
There have been warnings and concerns about the risk that the governments in some countries may utilise COVID-19 as an opportunity to further suppress the civil society movements which are anti-authority by nature. There were reports from countries like Myanmar and Indonesia that their governments, purportedly in the interest of public health, have adopted new laws, surveillance and other restrictive measures that have serious implications for civil society activities.
Cambodia is no exception, and the government’s attempt to control the activities is applied in two main ways. First, there are tight regulations on every aspect of NGOs operations. A range of activities that are not directly relevant to COVID-19 transmissions are being prohibited under vague but comprehensive regulation packages. An international NGO manager mentioned that freedom of expression at the individual, institutional and community levels became impossible while illegal logging, illegal fishing and filling-in of the sea for development projects continues. There were reports that some NGOs had even struggled to get permission from local authorities for a programme to distribute personal COVID-related protective materials like masks, alcohol and hand sanitiser to the poor villagers, and they had been under constant surveillance by the local authorities during the distribution process. Things became significantly more challenging as the Law on Governing the Country in a State of Emergency was enacted on 9 April 2021.
Second, a lack of transparency enables the government to apply any regulations without providing any substantial and scientific grounds. As for the system to collect, analyse and disseminate data on the internal transmission of COVID-19, there has been a public suspicion that the government’s updates are being manipulated according to the political needs. Civil society actors were not given any reliable source of information to verify the validity of the government’s statements, and were not included in any consultation about the social regulations/arrangements applied as part of the state responses to COVID-19.
Related to the above point, people are also concerned that the Sino-Cambodia connection seems to be getting stronger in the midst of COVID-19. It’s been a while since China emerged as the most important partner of these countries for economic, humanitarian, and development collaboration; this international tie offers the Cambodian government important grounds to compromise or ignore many Western donors’ demands for improving human rights and transparent governance. Over the past few years, Cambodia’s challenges to such demands from European and American partners have become significantly more direct and outspoken.
During the pandemic, this unbalanced influence from foreign actors is intensifying. Having had a critical impact in their own territories, many Western countries are in competition to secure more vaccines and to tighten the regulations for international travel. These conditions put many developing countries like Cambodia in a challenging situation for international cooperation. In contrast, China is increasing its material and diplomatic support to Cambodia. Thus far, China has provided three shipments, totalling over 1,700,000 doses, of Sinopharm, the vaccine that it developed. This far outnumbers the 324,000 doses of the AstraZeneca vaccine that were received from COVAX Facility of the World Health Organisation.
This not only strengthens the government-to-government friendship; it draws the attention of the Cambodian population despite suspicions about the quality of the vaccines. To many human rights advocates, China’s increased influence means that the political authority will care less about international pressure to enhance human rights in the country. Such fears held by the Cambodian civil society are being intensified by China’s role in disputing Western powers’ criticisms of the military coup in Myanmar.
In short, the combined impact of the restricted physical mobility, a plunge in funding, and stronger government control means that human rights organisations in Cambodia are facing one of their most challenging situations in recent times. The people with whom we communicated also expressed their concerns that they need to manage these challenges while also dealing with the formidable (and real) threat of COVID-19. Most of these issues are likely to continue, if not become exacerbated, even after the ongoing pandemic itself is brought under control, unless some immediate actions to alleviate this risk are undertaken. As their traditional partners are unable to maintain the same support, these human rights activists question if civil society actors in countries which have been less significantly impacted by COVID-19. like Australia and New Zealand, can turn their attention to them.
Fiji’s Lautoka Hospital is now closed to members of the public after a new positive case announced last night was that of a patient who was admitted for a surgical procedure at the hospital.
Health Secretary Dr James Fong said all medical services would now be re-routed to a network of back-up hospitals in Nadi, Ba, Sigatoka, as well as the Punja and Kamikamica health centres in Lautoka.
“We’ve activated the entire government machinery to ensure these critical services remain accessible to our people,” Dr Fong said.
The Fiji Times reports that a 53-year-old patient at Lautoka Hospital had died – the third death from covid-19 in Fiji.
As announced before, he said the borders of the containment areas were open to those travelling for medical emergencies.
“Given we expect more cases, and more severe cases, sections within the Lautoka Hospital are being converted into intensive care units which will house additional beds and ventilators,” he added.
Staff accommodated in hospital Dr Fong said the staff of Lautoka Hospital would be accommodated and work within the hospital while contact tracing continued.
“Remember, our staffing capacity was already stretched due to quarantine of the close contacts of our two doctors,” he said.
“Those who are working will operate on high-alert, fully-equipped in the proper personal protective equipment.
“They will be screened regularly and tested often.
“We are going to provide them with any and all support that they need. Food, supplies, bedding, whatever they require, we will provide.”
Earlier last night, Dr Fong said some staff who had left the hospital had been called back in, and Republic of Fiji Military Forces (RFMF) personnel and police officers had ring-fenced the entire hospital. They would strictly manage who was allowed onto the premises.
“More than 400 patients, doctors, nurses, and other staff have been sequestered and will be effectively quarantined within the hospital until we can determine who else may or may not have had contact with this patient,” Dr Fong said.
Fiji’s Lautoka Hospital is now closed to members of the public after a new positive case announced last night was that of a patient who was admitted for a surgical procedure at the hospital.
Health Secretary Dr James Fong said all medical services would now be re-routed to a network of back-up hospitals in Nadi, Ba, Sigatoka, as well as the Punja and Kamikamica health centres in Lautoka.
“We’ve activated the entire government machinery to ensure these critical services remain accessible to our people,” Dr Fong said.
As announced before, he said the borders of the containment areas were open to those travelling for medical emergencies.
“Given we expect more cases, and more severe cases, sections within the Lautoka Hospital are being converted into intensive care units which will house additional beds and ventilators,” he added.
Staff accommodated in hospital
Dr Fong said the staff of Lautoka Hospital would be accommodated and work within the hospital while contact tracing continued.
“Remember, our staffing capacity was already stretched due to quarantine of the close contacts of our two doctors,” he said.
“Those who are working will operate on high-alert, fully-equipped in the proper personal protective equipment.
“They will be screened regularly and tested often.
Patient 125 dead: #COVID19Fiji
A 53yo man has succumbed to #COVID19 in Lautoka. Originally admitted for surgery, the patient is also the suspected origin of 2 infections at Lautoka Hosp.
The hospital w over 400 staff & patients has been closed in by military&police. #FijiNews
“We are going to provide them with any and all support that they need. Food, supplies, bedding, whatever they require, we will provide.”
Earlier last night, Dr Fong said some staff who had left the hospital had been called back in, and Republic of Fiji Military Forces (RFMF) personnel and police officers had ring-fenced the entire hospital. They would strictly manage who was allowed onto the premises.
“More than 400 patients, doctors, nurses, and other staff have been sequestered and will be effectively quarantined within the hospital until we can determine who else may or may not have had contact with this patient,” Dr Fong said.
As the U.S. rushes to vaccinate its population against the coronavirus, most counties with the sickest residents are lagging behind and making only incremental progress reaching their most vulnerable populations.
A ProPublica analysis of county data maintained by the U.S. Centers for Disease Control and Prevention shows that early attempts to prioritize people with chronic illnesses like heart disease, diabetes and obesity have faltered. At the same time, healthier — and often wealthier — counties moved faster in vaccinating residents, especially those 65 and older. (Seniors are a more reliable measure of vaccination progress than younger adults, who are less likely to have been eligible long enough to receive their second shots.) Counties with high levels of chronic illnesses or “comorbidities” had, on average, immunized 57% of their seniors by April 25, compared to 65% of seniors in counties with the lowest comorbidity risk.
A similar gap has also opened for all other adults. The one-third of counties with the highest chronic illness risk have on average finished shots for 15% of their 64-and-under residents, four percentage points below the average for the healthiest one-third of counties.
In counties with high rates of chronic disease, residents are more likely to die prematurely from heart or pulmonary diseases, diabetes or illnesses related to smoking or obesity. Those conditions also increase a person’s risk of developing severe COVID-19.
People with chronic illnesses are especially important to vaccinate because their coronavirus infections are more likely to end in hospitalization and death, said Janet Baseman, an epidemiology professor at the University of Washington. If counties with high comorbidities remain behind, she said, “then we are not accomplishing our objective, as communities or as a nation, of saving lives.”
Counties With the Highest Health Risks Have the Lowest Vaccination Rates Among Seniors
In the four months since public vaccinations began, clear disparities have emerged in how quickly the richest and poorest counties have delivered shots to their residents. Multiple health experts and officials say the numbers underscore a key strategic misstep under the Trump administration, which asked state and local governments to prioritize people with illnesses that would increase their chances of hospitalization or death, but provided no additional funding to support the efforts.
Many states chose a simpler approach, opening vaccine appointments to everyone 65 and older with minimal on-the-ground outreach to people with chronic illnesses. “It made some states go a little bit faster,” said Dr. Grace Lee, a member of the CDC’s Advisory Committee on Immunization Practices and an infectious diseases physician at Stanford Children’s Health. “But I think it really increased the inequities early on.”
When vaccinations started in December and January for the general population, the federal Department of Health and Human Services distributed free doses and supplies, but almost no money or staffing to administer the shots. State and local health officials had to decide who would first be eligible for the small amounts of vaccine then available and how to get doses into arms. They also had to watch for interlopers — many of them young, white and from other locations — who booked appointments they didn’t qualify for.
In counties with more chronic illness, identifying the neighborhoods and housing complexes where residents or critical workers most need the shots — and then actually getting them to accept vaccinations — can be complicated, time-consuming work. Health officials in several counties with high rates of chronic illness said they are making slow progress by focusing resources on small events and mobile teams instead of on sprawling mass vaccination sites.
ProPublica focused on comorbidities because they are directly related to increased risk of developing severe COVID-19. People with lower incomes are more likely to have comorbidities; urban counties with high average incomes tend to have fully immunized a larger share of their older residents than other counties. In addition to income, the analysis looked at the urban and rural divide, age demographics and differences between states’ overall vaccination rates.
While communities of color have disproportionately high rates of chronic illness nationally, the analysis found no relationship between counties’ racial demographics and coronavirus vaccination rates.
The rollout has largely relied less on government outreach than on individual initiative. People with flexible schedules, transportation and regular access to the health care system have been better able to get appointments on their own or with help from family and friends. Those with less support have fallen behind.
Separately,surveys by the CDClast year indicated that adults with underlying medical conditions were less interested in getting the vaccine than healthier adults. People surveyed who said they were unlikely to get vaccinated most often cited concerns about side effects and safety.
To date, more than 98 million people in the U.S. — including 37 million seniors — are fully vaccinated against the coronavirus, while another 150 million adults have yet to receive a shot. During an address to a joint session of Congress on Wednesday, President Joe Biden heralded the vaccination effort as “one of the greatest logistical achievements” in the country’s history.
The push continues even as demand for shots appears to be declining, said Michael Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota.
Providers injected more than 21.7 million doses during the second week of April, according to CDC data, as the supply of vaccines from Pfizer, Moderna and Johnson & Johnson increased significantly. That number declined to 19.2 million shots the next week, and preliminary figures indicate immunizations dropped even more sharply last week. (Federal authorities temporarily paused use of the Johnson & Johnson vaccine for 10 days to study a small number of blood clot cases potentially related to the shot. It has since been cleared for use.)
There probably aren’t yet enough fully vaccinated people in the U.S. to protect against another surge, Osterholm said, especially with the more transmissible coronavirus variants now prevalent. In Michigan, new cases again soared in April, setting records for daily COVID-19 hospitalizations.
“We’re not out of the woods yet in this country,” Osterholm said. “What happened in Michigan could still happen in a number of other states out there. Even with the level of vaccination they’ve had and the previous infections, look what still happened.”
Reaching the most vulnerable has been a top concern for many of the poorest cities and counties since vaccinations began.
In Baltimore, COVID-19 caused far more severe illness and death in the majority-Black city’s communities of color, where people with chronic illnesses are more common, according to Dr. Letitia Dzirasa, the city health commissioner. During the first month of the vaccine rollout, the Baltimore health department realized it needed different tactics for immunizing its seniors.
The city of Baltimore has the highest rates of diabetes, smoking and obesity of the seven counties in its metro area, and its premature death rate is nearly double that of its neighboring counties, data from the National Institute of Environmental Health Sciences shows. It ranks among the nation’s most at-risk jurisdictions from chronic illness. Other parts of the region, like the more affluent nearby Howard County, are among the healthiest.
CDC data shows just 55% of Baltimore City’s seniors were fully vaccinated as of April 25, 15 percentage points lower than the rate for residents 65 and older in larger Baltimore County, which surrounds the city.
Counties in the Baltimore Metro Area With the Lowest Vaccination Rates Among Seniors Have Some of the Highest Health Risks
Within Baltimore, Dzirasa said, the pandemic hit hardest in Black neighborhoods on the city’s east and west sides, where residents have long struggled against discrimination, poverty and chronic illnesses. “Unfortunately, we’ve seen the same thing again with vaccination rates,” she said.
The city health department knew that many of its most vulnerable seniors would have no transportation to vaccination sites, and that their senior living centers were less likely than facilities in wealthier communities to have relationships with pharmacies to secure doses.
In January, Dzirasa said, her staff partnered with hospitals and pharmacies to create mobile vaccine teams that could deliver shots directly to those most at risk of severe COVID-19.
The first step was to win residents’ trust with visits to centers from community health workers, who explained the vaccines, provided reassurance and scheduled appointments. The teams identified 117 senior living centers and have immunized residents one by one at almost every facility over the past three months.
“It’s definitely a slower approach,” Dzirasa said. “At these events, we’re doing anywhere from 75 to 150 people, tops.”
Baltimore has multiple mass vaccination sites that can each provide from hundreds to thousands of shots a day. A couple of months ago, all site appointments were booked, and ineligible people had to be weeded out, Dzirasa said. Now, those spots are increasingly unfilled, and Dzirasa expects gradual progress going forward.
The disparity in vaccination rates between counties with high rates of chronic illness and the rest of the country is partly the result of the Trump administration’s decision not to invest federal dollars in vaccine sites at the beginning, argues Lee.
“They launched this massive campaign and were like, ‘Good luck, you’re on your own,’” Lee said. “And not only do you have to deliver a very complicated series of vaccines, but on top of that we expect you to address inequities, all without any additional support.”
The Biden administration set up several mass vaccination sites in high-risk communities in February and has now sent federal workers, equipment or funds to operate more than 400 vaccination sites nationwide. But many counties with high rates of comorbidity are still working to make up for a slow start.
The winter COVID-19 surge was peaking when vaccine doses started to arrive in Wyandotte County, part of Kansas City’s urban core. Small deliveries containing about 2,000 doses arrived each week from the federal government, said Dr. Erin Corriveau, the county’s deputy medical officer.
At first, only health care workers and nursing home residents qualified to be vaccinated. Then, on Jan. 21, Kansas Gov. Laura Kelly opened eligibility to everyone 65 and older, including more than 20,000 seniors in Wyandotte County.
“We’re going, ‘Oh my God, that’s a huge number of people,’” Corriveau recalled. The county decided to set its own eligibility rules, since it was still receiving just 2,000 doses a week.
Most new COVID-19 cases at the time were young adults. To help drive down case numbers, Corriveau said, the county temporarily narrowed eligibility to just residents 85 and older while adding critical workers whose jobs exposed them to greater infection risk.
Wyandotte County opened the shots to all seniors a few weeks later as case numbers dropped. But the demand for shots was modest, Corriveau said, especially compared to the clamor in other parts of the country, where older Americans struggled to find providers with available doses.
The county now runs three mass vaccination sites located on bus routes, with assistance from the Federal Emergency Management Agency. It keeps pharmacies stocked with vaccines, and dispatches “drop teams” to administer shots at small neighborhood operations. Doses are plentiful, but willing recipients are scarce. Corriveau said many of the county’s seniors are wary about the vaccines’ safety and have been unwilling to get the shots at large, impersonal sites.
“We’ve tried to make this vaccine as available as humanly possible,” she said. “We’re incentivizing vaccines with giveaways and food boxes and we’re doing Saturday hours and expanding our evening hours.”
Despite those efforts, only 56% of seniors in Wyandotte County were fully vaccinated as of April 25. A few miles south, in Johnson County, more than 83% were immunized.
The neighboring jurisdictions have little in common with each other. Wyandotte, meanwhile, stands out as being more diverse, with residents who suffer from far more chronic illness. Wyandotte’s rate of premature death is double Johnson’s rate, according to NIH data.
Tami Gurley, associate professor of population health at the University of Kansas Medical Center, said Johnson County has longstanding advantages that likely helped its residents get vaccinated so quickly.
“You have people with time, who can get on computers and sign up for multiple lists,” Gurley said. “They all have their own transportation, nobody’s relying on public transportation, it’s all private cars out here.”
The university medical center where Gurley works is located in Wyandotte and cares for its residents, she said. But many of its health workers live in other parts of Kansas City, including Johnson County. “That is where the doctors live, and the professors, and the people who tend to be more pro-vaccine to start with,” she said.
Wyandotte’s health officials are trying to reassure residents that the shots are safe and that communities of color can trust the county health department. “Frankly, there have been major, major issues of trust,” Corriveau said of residents’ view of local agencies, “which are warranted.”
She and her colleagues are increasingly asking trusted community leaders to stand in for epidemiologists. Throughout the pandemic, Rev. Tony Carter, Jr., senior pastor of Salem Missionary Baptist Church, has encouraged his congregation to test for the virus, follow health protocols and, in recent months, get vaccinated.
Carter’s church volunteered to host a Saturday neighborhood vaccine event on April 17, and nearly 50 people signed up for appointments to get the Johnson & Johnson shot. But several days before the event, federal authorities paused use of that vaccine as they investigated six cases of serious blood clots among the 6.8 million people who had received it. (The U.S. resumed use of the Johnson & Johnson vaccine without limitations on April 23.)
The county switched to another vaccine, but half of the recipients canceled their appointments. Carter reassured his congregants that the vaccine would offer a way of eventually reuniting with family. About two dozen people kept their appointments and received their first vaccine dose. “Most of those people stayed because of their connection to the church,” he said.
Big Pharma has hired an army of lobbyists to pressure U.S. lawmakers to block an effort at the World Trade Organization to loosen intellectual property rules onCOVID-19 vaccines, which would allow countries around the world to ramp up production, vaccinate more people and bring the pandemic to an end sooner. Dozens of countries from the Global South, led by India and South Africa, are demanding a temporary waiver on vaccine patents, but rich countries, including the U.S. under both the Trump and Biden administrations, have opposed the move. Lee Fang, investigative journalist at The Intercept, says there is a “glut” of vaccines going to wealthy countries while much of the rest of the world is left waiting. “These initiatives that are based on voluntary agreements with the pharmaceutical companies have not worked,” he says. Fang also discusses his reporting on the Biden’s administration’s ties to the vaccine makers: White House adviser Anita Dunn is co-founder of the consulting firmSKDK, which works closely with Pfizer; Biden’s domestic policy adviser, Susan Rice, holds up to $5 million in Johnson & Johnson shares; and White House science adviser Eric Lander holds up to $1 million in shares of BioNTech, which co-developed Pfizer’s coronavirus vaccine.
Fiji has reported no new case of coronavirus infection after the screening of 7560 Fijians and 1212 tests conducted by the Ministry of Health and Medical Services.
However, at this evening’s covid-19 daily press briefing, Health Secretary Dr James Fong stressed that there was no need to celebrate.
Dr Fong said it did not mean there were no further cases in Fiji – it meant that none have been detected over the past 24 hours.
“We are certain there are more cases that will develop or – worryingly – that an unconfirmed case of the virus has already developed into a highly-contagious disease,” he said.
“Our biggest fear right now is that someone, with symptoms, has not reported to a screening clinic or called 158.”
As of today, Sunday, May 2, 2021, there are still 49 active confirmed covid-19 cases in isolation, 16 of which are border quarantine cases, with 31 locally transmitted cases and two currently still under being investigated to determine the source of transmission.
Fiji has reported no new case of coronavirus infection after the screening of 7560 Fijians and 1212 tests conducted by the Ministry of Health and Medical Services.
However, at this evening’s covid-19 daily press briefing, Health Secretary Dr James Fong stressed that there was no need to celebrate.
Dr Fong said it did not mean there were no further cases in Fiji – it meant that none have been detected over the past 24 hours.
“We are certain there are more cases that will develop or – worryingly – that an unconfirmed case of the virus has already developed into a highly-contagious disease,” he said.
“Our biggest fear right now is that someone, with symptoms, has not reported to a screening clinic or called 158.”
As of today, Sunday, May 2, 2021, there are still 49 active confirmed covid-19 cases in isolation, 16 of which are border quarantine cases, with 31 locally transmitted cases and two currently still under being investigated to determine the source of transmission.
The authorities have escalated the measures with no businesses allowed to operate for a 56-hour period.
Containment measures have also been stepped around the capital Suva in a rush to trace the Indian variant of covid-19.
The Health Ministry tonight ordered everyone indoors from 8pm amid concerns the B16-17 variant has spread through the community.
Fiji now has had 117 covid-19 cases, 65 recovered and two deaths reported.
Garment factory employees
The ministry has warned that a 52-year-old woman from Nausori Town who tested positive over the past 48 hours may have exposed 887 garment factory employees to the virus.
Parallel to that, Health Secretary Dr James Fong told a media conference there were concerns of a further spread of covid-19 from a returning Fiji citizen who had tested negative before interacting with quarantine personnel before travelling extensively through Suva.
Dr Fong said the man had been cleared of the virus but was recalled to quarantine following fears he may have contracted the virus from soldiers at the facility who had fraternised with others while in isolation.
Meanwhile, Dr Fong confirmed a new case – she is the wife of a man from the province of Ra which is now also on lockdown.
The source of this couple’s infection is not yet linked to current cases which began when a soldier at a quarantine facility contracted the virus between April 10-12 from two Fijians who returned from India.
While announcing the lockdown, Dr Fong said the measures were escalated after they tested more than 1000 Fijians overnight and found another positive person.
“We have some urgent developments to cover that require immediate changes to our containment strategy,” Dr Fong said.
Contact tracing full-swing
“Our contact tracing stemming from case number 113 — the garment factory worker – is in full-swing. There are two factories we are focused on.”
Health checks are ongoing in Fiji in an effort to combat covid-19. Image: RNZ/Fiji government
Dr Fong said one of the factories is Lyndhurst, the factory in which the woman worked. The other is the Mark One Apparel factory.
“Employees at these factories travel to and from work on the same company-provided transportation, so we are treating both of these factories as potential source points of further transmission.”
Following an overnight screening effort, the government still needed to test hundreds of factory employees.
Dr Fong said there was no more time to waste in locating the rest of those exposed in the factories and so asides from emergency medical trips, no movement was allowed.
“To allow my teams to find these Fijians quickly, we will be locking down the Suva and Nausori Containment zones from 2000 hours tonight until 0400 hours Monday morning.
No one should leave home
“No one should leave their homes. I’ll say that again, within the lockdown zone, no one, not parents, not breadwinners, not children, no one should leave their homes.
“The police will be enforcing that movement restriction.”
Given it’s short notice of the lockdown, announced with only 30 minutes before it was enforced, the government organised food packs to be delivered to those who needed it.
“If you live in the lockdown area and need to access this emergency food supply, you can call toll-free number 161 from 9am tomorrow morning. Please be patient, your calls will be answered.”
Meanwhile, the Ministry of Health has since sent specimens to Melbourne to determine the origin of the cluster in the Ra province it has not been able to link to the B16-17 cluster.
The ministry said it would review the lockdown on Sunday.
This article is republished under a community partnership agreement with RNZ.
Fiji’s government has taken the most drastic measures since covid-19 hit the country in March last year.
Most of the country is on lockdown from 8pm tonight to 4am on Monday local time.
This comes amid a new covid-19 case confirmed by the Health Ministry, taking the total number of active cases to 50, with 29 transmitted locally.
The authorities have escalated the measures with no businesses allowed to operate for a 56-hour period.
Containment measures have also been stepped around the capital Suva in a rush to trace the Indian variant of covid-19.
The Health Ministry tonight ordered everyone indoors from 8pm amid concerns the B16-17 variant has spread through the community.
Fiji now has had 117 covid-19 cases, 65 recovered and two deaths reported.
Garment factory employees The ministry has warned that a 52-year-old woman from Nausori Town who tested positive over the past 48 hours may have exposed 887 garment factory employees to the virus.
Parallel to that, Health Secretary Dr James Fong told a media conference there were concerns of a further spread of covid-19 from a returning Fiji citizen who had tested negative before interacting with quarantine personnel before travelling extensively through Suva.
Dr Fong said the man had been cleared of the virus but was recalled to quarantine following fears he may have contracted the virus from soldiers at the facility who had fraternised with others while in isolation.
Meanwhile, Dr Fong confirmed a new case – she is the wife of a man from the province of Ra which is now also on lockdown.
The source of this couple’s infection is not yet linked to current cases which began when a soldier at a quarantine facility contracted the virus between April 10-12 from two Fijians who returned from India.
While announcing the lockdown, Dr Fong said the measures were escalated after they tested more than 1000 Fijians overnight and found another positive person.
“We have some urgent developments to cover that require immediate changes to our containment strategy,” Dr Fong said.
Contact tracing full-swing “Our contact tracing stemming from case number 113 — the garment factory worker – is in full-swing. There are two factories we are focused on.”
Health checks are ongoing in Fiji in an effort to combat covid-19. Image: RNZ/Fiji government
Dr Fong said one of the factories is Lyndhurst, the factory in which the woman worked. The other is the Mark One Apparel factory.
“Employees at these factories travel to and from work on the same company-provided transportation, so we are treating both of these factories as potential source points of further transmission.”
Following an overnight screening effort, the government still needed to test hundreds of factory employees.
Dr Fong said there was no more time to waste in locating the rest of those exposed in the factories and so asides from emergency medical trips, no movement was allowed.
“To allow my teams to find these Fijians quickly, we will be locking down the Suva and Nausori Containment zones from 2000 hours tonight until 0400 hours Monday morning.
No one should leave home “No one should leave their homes. I’ll say that again, within the lockdown zone, no one, not parents, not breadwinners, not children, no one should leave their homes.
“The police will be enforcing that movement restriction.”
Given it’s short notice of the lockdown, announced with only 30 minutes before it was enforced, the government organised food packs to be delivered to those who needed it.
“If you live in the lockdown area and need to access this emergency food supply, you can call toll-free number 161 from 9am tomorrow morning. Please be patient, your calls will be answered.”
Meanwhile, the Ministry of Health has since sent specimens to Melbourne to determine the origin of the cluster in the Ra province it has not been able to link to the B16-17 cluster.
The ministry said it would review the lockdown on Sunday.
This article is republished under a community partnership agreement with RNZ.
One of Fiji’s latest two cases of covid-19 remains a concern for health authorities.
The Health Ministry said a 53-year-old caretaker from the town of Rakiraki would require further investigation into his contacts to determine whether he is linked to other covid-19 patients.
Health Secretary Dr James Fong, who was reported by The Fiji Times today as issuing a warning to the public, said the man showed symptoms of the virus when he visited the health centre on Saturday.
Dr Fong said the man was being isolated at Lautoka Hospital.
He said the other latest case was linked to a woman who contracted the virus from her husband, a worker at the MIQ facility in Nadi.
“There are others out there who may have been in contact with this individual. We need all Fijians living in the Rakiraki area to be alert of any potential covid-19 symptoms and if they are feeling unwell, follow this man’s example.”
Either visit your nearest screening clinic or dial 158 for the Ministry of Health officials to come and check on you,” he said.
Three people charged
Three people have appeared in court over charges relating to a breach of the Public Health Act.
The trio’s arrest on Tuesday came as the authorities warned that a surge in covid-19 cases on the main island of Viti Levu threatens 60 percent of the country’s population.
Fiji health officials Dr Aalisha SahuKhan (left) and Health Secretary Dr James Fong. Image: RNZ/Facebook/Fiji govt
Police say the three men were found intoxicated in Suva during the lockdown restrictions imposed since Monday.
Dr Fong said following basic safety measures could save lives.
“Even if we are not showing any symptom of the virus we need to behave as if we have got covid-19. By doing so and thereby wearing masks, staying at home and turning on your careFiji App you will be saving lives.
“With every new case, this crisis brings new and more personal meaning for more Fijians. Not only for Fijian members but for neighbors and the entire community,” said Dr Fong.
Fiji has 111 covid-19 cases, 44 active with 26 of them locally-transmitted cases.
There have been 65 recoveries and two deaths reported since the country’s first case was detected on March 19 last year.
‘Start listening’ appeal The Wold Health Organisation (WHO) said Fijians needed to start listening to all advisories and take immediate action to safeguard themselves from the B1617 variant of covid-19.
The WHO acting head of the Pacific, Dr Akeem Ali, said Fijians needed to take heed and work to protect themselves.
He told FBC News that the impact of the variant on India showed that Fijians needed to be prepared.
Dr Ali said people must be attentive to directions and the advice given by the government.
He said when authorities say stay at home, it means stay at home, when they say wear masks, it means wear masks.
Dr Ali said the need for beds, ventilators and other equipment to fight the virus had become paramount, and the WHO stood ready to assist.
This article is republished under a community partnership agreement with RNZ.
One of Fiji’s latest two cases of covid-19 remains a concern for health authorities.
The Health Ministry said a 53-year-old caretaker from the town of Rakiraki would require further investigation into his contacts to determine whether he is linked to other covid-19 patients.
Health Secretary Dr James Fong, who was reported by The Fiji Times today as issuing a warning to the public, said the man showed symptoms of the virus when he visited the health centre on Saturday.
Dr Fong said the man was being isolated at Lautoka Hospital.
He said the other latest case was linked to a woman who contracted the virus from her husband, a worker at the MIQ facility in Nadi.
“There are others out there who may have been in contact with this individual. We need all Fijians living in the Rakiraki area to be alert of any potential covid-19 symptoms and if they are feeling unwell, follow this man’s example.”
Either visit your nearest screening clinic or dial 158 for the Ministry of Health officials to come and check on you,” he said.
Three people charged Three people have appeared in court over charges relating to a breach of the Public Health Act.
The trio’s arrest on Tuesday came as the authorities warned that a surge in covid-19 cases on the main island of Viti Levu threatens 60 percent of the country’s population.
Fiji health officials Dr Aalisha SahuKhan (left) and Health Secretary Dr James Fong. Image: RNZ/Facebook/Fiji govt
Police say the three men were found intoxicated in Suva during the lockdown restrictions imposed since Monday.
Dr Fong said following basic safety measures could save lives.
“Even if we are not showing any symptom of the virus we need to behave as if we have got covid-19. By doing so and thereby wearing masks, staying at home and turning on your careFiji App you will be saving lives.
“With every new case, this crisis brings new and more personal meaning for more Fijians. Not only for Fijian members but for neighbors and the entire community,” said Dr Fong.
Fiji has 111 covid-19 cases, 44 active with 26 of them locally-transmitted cases.
There have been 65 recoveries and two deaths reported since the country’s first case was detected on March 19 last year.
‘Start listening’ appeal The Wold Health Organisation (WHO) said Fijians needed to start listening to all advisories and take immediate action to safeguard themselves from the B1617 variant of covid-19.
The WHO acting head of the Pacific, Dr Akeem Ali, said Fijians needed to take heed and work to protect themselves.
He told FBC News that the impact of the variant on India showed that Fijians needed to be prepared.
Dr Ali said people must be attentive to directions and the advice given by the government.
He said when authorities say stay at home, it means stay at home, when they say wear masks, it means wear masks.
Dr Ali said the need for beds, ventilators and other equipment to fight the virus had become paramount, and the WHO stood ready to assist.
This article is republished under a community partnership agreement with RNZ.