All mask wearing requirements in Aotearoa New Zealand — except in healthcare and aged care — will be scrapped, and household contacts will no longer need to isolate, the government confirmed today.
Prime Minister Jacinda Ardern and Minister for Covid-19 Response Dr Ayesha Verrall confirmed cabinet’s decision to scrap the Covid-19 Protection Framework — known as the “traffic light” system — and the majority of related public health restrictions.
The traffic light system will end tonight at 11.59pm.
Mask-wearing only required in healthcare and aged care: including hospitals, pharmacies, primary care, aged residential and disability-related residential care
People who test positive for covid-19 must still isolate for seven days, but household contacts no longer required to provided they take a RAT test every day
All government vaccine mandates to end on 26 September 26
Removal of all vaccine requirements for incoming travellers and air crew
Leave support payments to continue
All New Zealanders over age 65, and Māori over age 50, to get automatic access to covid-19 antiviral drugs if they test positive for Covid-19
Ardern said it marked a milestone in New Zealand’s response to the virus.
She said people may still be asked to wear a mask in some places but it would be at the discretion of those managing the location, not a government requirement. Vaccination requirements would also be at the discretion of employers.
‘Claim back certainty’
“Cabinet has determined that based on public health advice we are able to remove the traffic light system and with that decision claim back the certainty we have all lost over the last three years,” she said.
“For the first time in two years we can approach summer with the much needed certainty New Zealanders and business need, helping to drive greater economic activity critical to our economic recovery.
She said there was no question the actions of New Zealanders had saved thousands of lives, but the risks were changing.
“When we moved into our first lockdown the objective was simple: To save lives and livelihoods,” Ardern said.
“I’m sure there will be many who over the years will pore over the details of every nation’s response including ours. They’ll certainly measure the outcomes in different ways but when you look at countries of our size and compare them, they’ll find the tragic loss for instance of 15,500 people in Scotland and less than 2000 in New Zealand.
“The most recent health advice now tells us that with the lowest cases and hospitalisations since February, our population well vaccinated, and expanded access to anti-viral medicines, New Zealand is in a position to move forward.”
New Zealand could move on with confidence that its actions had successfully managed cases down, she said.
‘Never to be taken alone’
“This pandemic was never one to be taken on alone, and it never was. And so today I say again to everyone from the bottom of my heart, thank you.
“I know there will be those concerned by the changes made today. I can assure you that we would not make them if we did not believe we were ready but we also need to remember that not everybody experiences covid or its risk — including to our disability community — in the same way.
“That’s why isolating covid cases to protect our most vulnerable is important, and why treatment is too.”
She said she hoped it would be the first summer where the “covid-19 anxiety can start to heal”.
“As a nation, covid has hurt us in many ways but perhaps the one we talk about less than others is the toll it’s taken on everyone’s mental health. I see that toll — I see it in my colleagues, in my community in Tāmaki Makaurau, and especially I see it in our kids.
“I don’t want people’s wellbeing to be the price of covid, but it is going to take a concerted effort from us as government and others for that not to be the case.”
Ardern said one of the byproducts of the pandemic had been that New Zealand now have some of the most advanced mental health tools in the world, and the government had taken a number of steps to improve mental wellbeing support.
Two apps a highlight
This included two apps she highlighted for anyone who may need them: Groove and Habits.
Ardern finished her statement with a line from when New Zealand first went into lockdown: “‘For the next wee while, things will look worse before they look better’. It turned out to be true, things did get worse, things did get hard, but it’s also true that finally they will and can be better”.
Ardern said looking back, decisions were often being made with imperfect information but the decisions were made with the best intentions and she stood by it.
She said the government had been open to the idea of an independent inquiry into the response but was still getting advice about what that would look like.
“We do want to learn from this period and I think you’ll see that we’ve been taking that approach all the way through.”
Asked if it was the end of the covid response, Ardern said she hoped the change would give people huge confidence and optimism.
“We are moving on because this pandemic has moved on.”
The traffic light system used things like gathering limits but that was no longer fit for purpose, she said.
“We don’t need those extraordinary measures, so we won’t use them.”
Right time to remove ‘traffic lights’
Dr Verrall said New Zealand had succeeded in avoiding the devastation caused by the pandemic overseas, and now was the right time to remove the traffic light framework and begin a new approach to managing the virus.
“Together we have got through this with one of the lowest cumulative mortality rates in the world.”
She announced another 40,000 courses of antiviral medication had also been purchased and would be freely available to older New Zealanders.
“Anyone over the age of 65, and Māori and Pacific people over the age of 50, or anyone who meets Pharmac requirements, can access the treatment in the early stages of contracting the virus,” she said.
“This means more than double the number of New Zealanders will be able to access these medicines if they need them than previously.
She acknowledged that lessening the restrictions caused concern to disabled and immune-compromised people.
“I want to reassure those Kiwis that we are making these changes because risks are lower, in fact cases are more than 10 times lower than what they were earlier in the year and we now have layers of protections in place.”
She said the support was not ending and hoped that removing the remaining vaccine mandates would ease the staffing pressures disability services have been under.
This article is republished under a community partnership agreement with RNZ.
United States-based medical doctors have praised the Marshall Islands for an “unprecedented” response to its first covid outbreak, as the positive case numbers declined dramatically this week after a record-setting first two weeks.
“The Marshall Islands has exceeded most expectations to deliver testing and treatment for large numbers of people, and to provide care for those with covid,” said Dr Richard Brostrom, the US Centers for Disease Control Field Medical Officer who arrived in Marshall Islands last week to assist the Ministry of Health and Human Services.
Brostrom has been engaged in the US response in all US-affiliated islands, including most recently in the Micronesian states of Pohnpei and Kosrae.
The Marshall Islands was seeing above 1000 positive cases daily last week, but those numbers dropped to the low hundreds by Monday this week as the omicron BA.5 variant appeared to peak and drop off quickly.
Last week, Johns Hopkins University, which tracks covid cases globally, reported that the Marshall Islands set a seven-day all-time record for the rate of positive cases of covid.
“But what the data also shows is a jurisdiction that is able to test, treat and provide access to healthcare,” said Dr Brostrom.
“BA.5 will behave the same everywhere,” he said. “The Marshall Islands had access points for people to get tested and treated, it was prepared and it handled thousands of people in a short period of time.”
14 died in two weeks
No deaths have been reported since last Friday. During the first two weeks, 14 people died of covid. The majority of the deaths were among people who were not vaccinated or partially vaccinated, the ministry reported.
Health authorities put the low number of deaths down to widespread use of PaxLovid, a five-day treatment that Dr Brostrom said was 90 percent effective in reducing symptoms of covid.
“The use of PaxLovid in Marshall Islands is appropriate, by the book, and unprecedented,” Brostrom said.
He said PaxLovid had been well used in all US-affiliated islands with covid. But uniquely in the Marshall Islands, more people sought healthcare and didn’t stay home when they got covid, he said.
“It was an opportunity for the Ministry of Health to deliver PaxLovid,” he said.
‘One of the best responses to this pandemic the world has seen’ Health Secretary Jack Niedenthal praised health workers and community volunteers for their response under pressure when more than 200 were initially sidelined by covid in the early days of the outbreak.
“As this current outbreak of covid-19 begins to lessen, the facts say, even with the complicated logistical issues and limited resources that we have in the Marshall Islands, and even though we have a very immuno-compromised population, we have had one of the best responses to this pandemic the world has seen,” said Niedenthal.
“Our goal from the beginning has been resolute: Let the science catch up to the virus, and now we are seeing the result of over two years of diligent prevention and preparation.”
Among unprecedented events in the Marshall Islands, Niedenthal said the nation was the “only country in the world to have been able to offer people of all ages vaccines before we had community spread of the virus”.
He added: “Our current fatality rate of 0.1 percent of covid-19 cases ranks as among the best in the world with only Palau having a similar fatality rate for this virus.”
Dr Brostrom was part of a “surge support medical team” involving CDC, WHO, Taiwan and other medical officials that arrived during the second week of the outbreak.
What the visiting doctors have seen in the first two weeks of the outbreak was “an amazing delivery (of services) that we haven’t seen elsewhere,” Dr Brostrom said.
Speed in setting up care sites
Dr Brostrom said the Ministry of Health’s speed in setting up the alternative care sites in the community was key to dealing with the BA.5 variant that is in Marshall Islands. BA.5 is milder in its effect than earlier variants but much more contagious.
“It is so fast that if you spend a week to get sites set up, you missed the boat.”
He said the country had seen a five-day surge in cases, a further five days at the peak number, and now five days of numbers dropping down.
“It is most certainly going down,” he said.
“It’s amazing to see how the Ministry of Health has responded — not just now, but for two and a half years,” said Dr Sheldon Riklon, one of two Marshallese US-trained medical doctors working at rural clinic in Majuro.
“The Marshall Islands has done well. The Ministry of Health leadership prepared the Marshall Islands for this.”
This article is republished under a community partnership agreement with RNZ.
One year on from Aotearoa New Zealand’s longest covid-19 lockdown, an epidemiologist says further lockdowns cannot be ruled out, instead preparing to do them better.
On 17 August 2021, New Zealand went to alert level 4 because the deadly delta variant had arrived.
Aucklanders had no idea that day that they would still be in lockdown until December, and that after 18 months of trying to keep covid-19 out, it would be here to stay.
The city was asked to hold the line so the country could get vaccinated, something critics said should have happened much earlier.
Auckland University epidemiologist Professor Rod Jackson was vocal in urging the country to aim high and vaccinate more than 95 percent of eligible people.
Reflecting back, he said New Zealanders responded well, with most areas hitting that mark or higher by the measurements at the time.
Much had been learnt about the virus — and how to respond to it — since then, with the highly contagious but less harmful omicron variant changing everything at the start of this year, he said.
But the danger was not over.
Random severity of variants
“I think there are a lot of people who think, ‘oh look, it’s getting less severe over time so we’re fine,’ but it’s pretty random whether the next variant is going to be less severe or not,” he said.
Either way, it would need to be at least as spreadable as omicron to take over, he said.
Empty … an Auckland motorway near the city centre, mid-morning on 19 August 2021. By 7 September 2021 the rest of New Zealand had moved to level 2, but Auckland stayed in alert level 3 restrictions until December 2. Image: Robert Smith/RNZ
The government has said lockdowns are not part of any future covid-19 plans, with the traffic light system taking its place.
But Professor Jackson said that may not “cut the mustard” if the worst happened.
“If we get a new mutation that is more severe, that kills more people, then we’ve got something huge to worry about,” he said.
“If that happens, if people start dropping dead in the street like the original version of covid, we will have little choice but to lock down.”
That was why the country still needed to be prepared for the worst, he said.
Frontline of delta outbreak
As an Auckland GP and co-leader of Te Rōpū Whakakaupapa Urutā, Dr Rawiri McKree-Jansen was at the frontline of the delta outbreak and lockdown and the vaccine rollout.
Some Māori and Pacific health teams had initially struggled to be given the resources they needed, or to be listened to.
The work they were able to do for their communities and the country showed what they were capable of and should be a lasting legacy, Dr McKree-Jansen said.
They were crucial to the vaccine roll out and helped the most vulnerable, especially those isolating.
“The mobilisation was impressive, relentless and co-ordinated,” he said.
“Those features are remarkable and give us a great sense of optimism about the contribution that Māori communities and Māori health professionals can make and I hope that is enduring.”
When it came to new variants, he said while it was important to be vigilant about what may come next, it was also important to focus on what was happening now.
“Omicron’s not done with us yet … I’m keen that we don’t forget the lessons we’ve learnt from the Delta and Omicron outbreaks – and supporting communities is fundamental to that.”
Both Professor Jackson and Dr McKree-Jansen acknowledged the people who had died since pandemic began, many more since the omicron outbreak that reached so many people.
But they said they were also grateful that many were protected by the lockdown and the vaccine rollout.
16 more people die RNZ News reports that another 16 people with covid-19 have died and there are 4489 new community cases today, according to the Ministry of Health.
There are 496 people in hospital, 13 of them are in a high dependency unit
Yesterday the ministry reported another 21 people with covid-19 had died and there were 533 people in hospital, including 12 in intensive care or a high dependency unit.
Deputy Director-General and Public Health Agency head Dr Andrew Old told media this afternoon that modelling from Covid Modelling Aotearoa showed New Zealand was continuing to track at the lower end of what was expected in terms of a second wave this winter.
“We passed a peak in cases earlier that the modelling suggested and now hospitalisations are also declining suggesting these too have peaked. It’s sitting somewhere between 800 and 850 occupied beds across the country in late July,” he said.
Te Whatu Ora-Health New Zealand interim national medical director Dr Pete Watson said the recent drop in covid-19 cases was an encouraging trend.
“By each one of us sticking to public health measures we are making a difference,” he said.
This article is republished under a community partnership agreement with RNZ.
The Marshall Islands is a live demonstration that the omicron BA.5 variant is the most contagious covid variant yet to appear.
In the first five days of the outbreak in the Marshall Islands, more than 10 percent of the population in Majuro, the capital, has tested positive, reports the Ministry of Health and Human Services.
From initial confirmation of a handful of positive cases in the community on August 8, the number of positive cases skyrocketed to the one-day total of 1064 testing positive on Saturday, August 13, at the three community-based “alternative care sites” established to test and treat local residents.
This brings Majuro’s total in the wake of the outbreak to more than 2000 cases in a population estimated at 20,000. There were nine early hospitalisations, with most reported to be recovered by Sunday.
President David Kabua on Friday signed a proclamation of a “State of Health Disaster,” which outlines duties of all ministries and government agencies to respond.
It also gives the government the power to access emergency funding for the response to the initial outbreak.
Health authorities reported two deaths in the first week — both men. The first was a 23-year-old man, the second a 69-year-old.
Both pronounced dead
They were both pronounced dead on arrival at Majuro Hospital’s emergency room, Health officials said. Their vaccine status was not announced.
Majuro experienced a chaotic first couple of days as alternative care sites (ACS) were rolled out at two local schools and at an outdoor sports court, with thousands of islanders crowding in to get tested.
By Friday the influx of hundreds of volunteers to support the Ministry of Health and Human Service in managing the flow of people led to improvements in the service.
“What we are seeing at these sites is what we expected, the ACS sites are getting better and more organised as we go along,” said Health Secretary Jack Niedenthal Sunday.
“Much of the chaos is beginning to die down, though it is still there for sure, but this will continue to get better.”
Spread was not contained to Majuro Atoll, the capital. Within a day of the initial confirmation of positive cases in the Majuro community last Monday, the first case was identified on Ebeye, the densely populated community next door to the US Army’s Reagan Test Site at Kwajalein Atoll.
In addition, several isolated outer atolls at week’s end were reporting multiple residents with covid-like symptoms.
All remote island flights suspended
All flights on Air Marshall Islands and all government ships to remote islands were suspended August 9 in an effort to contain the spread. But travellers from the previous week to remote islands unwittingly caused the spread.
August 12, a special Air Marshall Islands flight took a health team to Wotje Atoll, confirming multiple positive cases, training the local health aide to conduct further testing, and leaving a supply of PaxLovid and other therapeutic medicines for islanders, according to health officials.
Health teams were attempting to visit other remote islands for similar follow up Sunday, but all AMI pilots reportedly tested positive, putting flights in limbo.
Although the government did not require a lockdown, most churches cancelled in-person services Sunday and the one main road in the capital atoll was unusually quiet as people appeared to be staying home.
Restaurants also saw the number of customers decline dramatically, although most continued to see ongoing demand for takeout meals.
“We at the Ministry of Health and Human Services are very proud of the response that has come in from all corners of our country to help us deal with the health crisis,” said Niedenthal.
The ministry struggled in the initial phase of the outbreak with more than 200 of its staff, including many doctors and nurses, testing positive for covid — many exposed before they knew it was circulating in the community.
Covid-free success
Until last week the Marshall Islands had successfully employed some of the world’s strictest quarantine rules for people entering the North Pacific nation. This had kept it covid-free for the first two-and-a-half-years of the covid pandemic.
A reduction of quarantine time in recent weeks, coupled with unprecedented numbers of people coming in through the managed quarantine process is suspected to be the cause of the outbreak.
The government had earlier announced it was going to eliminate the managed quarantine requirement and open the borders on the October 1.
“As expected, the outbreak continues to gain strength,” Niedenthal said on Sunday.
“We had over 1000 cases in Majuro yesterday, almost double from the previous day. About 75 percent of the people we test are positive, which is an incredibly high positivity rate.”
A security officer controls the flow of islanders into one of several community-based alternative care sites established by the Ministry of Health and Human Services. Image: Wilmer Joel/RNZ Pacific
Outbreak escalating
Last week, as the outbreak was escalating, Majuro traditional leaders sent a letter to President Kabua calling for the borders to be closed and opposing the announcement that medical teams arriving this week would not be required to quarantine.
The medical surge support teams are from the US Centers for Disease Control and other agencies. Niedenthal emphasised the importance for delivering services to the public by these medical professionals.
He described these as “boots on the ground medical support professionals” and said they would be tested on arrival and then sent right into the field to support ongoing services by local Health authorities.
“As a country we have moved from prevention to mitigation because we are now fighting this disease,” he said.
“The days of quarantine upon arrival are now over. I know some people are nervous about this, but we at the Ministry of Health are not and we are the ones on the frontline,” Niedenthal said.
“Please respect these public health decisions. We knew this would have to be a fast shift in strategy that would trouble some people because we had been working so hard (and) successfully to prevent the disease from coming into the Marshall Islands.”
This article is republished under a community partnership agreement with RNZ.
The Marshall Islands lost its covid-free status yesterday when tests confirmed six positive cases in the capital, the first known community transmission since the pandemic started in early 2020.
It was not immediately clear the source of the covid-19 spread as Marshall Islands borders have been closed since March 2020 and rules currently require 10 days of government-managed quarantine prior to release.
The six people who tested positive Monday had “no travel history, no contact with anyone who was in quarantine,” said Health Secretary Jack Niedenthal.
The government moved quickly last night to announce a halt to the start of the new school year with all island schools scheduled to open this week.
President David Kabua delivered a brief 90-second statement to the nation via an online live stream in which he announced that the Ministry of Health and Human Services had confirmed six people positive in the capital of Majuro.
The President’s short speech was the first official notice of news that in the fashion of a small island had spread several hours prior to his speech.
“I advise people to remain calm and follow the protocols to prevent covid,” Kabua said.
President Kabua advised the country to follow established protocols of wearing facemasks when in public. Kabua wore a facemask while delivering his speech.
Notices on social media went viral in the minutes and hours after people learned of the first-ever covid community spread in this isolated north Pacific nation.
Although there were no rules except for school closure announced by government, within minutes of the official confirmation of the cases, a national basketball tournament game was halted mid-way through the contest Monday night, and some restaurants began shutting their doors.
The Office of the Chief Secretary said that the start of the new school year, which opened yesterday at some public schools and was scheduled to open later this week in private schools, would now be postponed for two months.
While businesses and government offices can continue as usual, hospital services will be modified and masks will be required in public for the next two months, said a statement issued by the government.
Marshall Islands President David Kabua … he wore a facemask in his live stream broadcast. Image: Wilmer Joel/File/RNZ
The government also announced a halt to travel by plane or ship to remote outer islands in hopes of restricting spread of covid to islands that have only rudimentary medical care services available.
“The most important lesson learned from Palau’s experience with a wave of covid starting in January is to protect the hospital during the initial stages of a covid outbreak,” said Niedenthal.
“This is to protect both the patients already in hospital from being infected by incoming covid patients and, of equal importance, minimising the exposure of hospital staff so they can remain functional and on the job.”
The Ministry of Health and Human Services moved quickly last night to set up previously planned “test and treat” facilities in designated locations in the community.
Niedenthal said the number one lesson learned from watching other nations respond to their covid waves was the priority of “protecting the hospital”.
The goal, he said, is to have people use community test and treat facilities where health officials will perform tests and determine treatment needed.
The entire Marshall Islands has a population estimated at only 42,000 scattered on dozens of atolls and single islands. The two urban centers of Majuro and Ebeye, however, contain three-quarters of the population and many people live in overcrowded conditions ripe for the spread of covid.
Laboratory tests of people who were positive for covid while in managed quarantine last month showed they were all BA.5 variant. And ministry officials said they were proceeding on the basis that BA.5 is what they are seeing.
One local resident said that he was aware of a church member who was confirmed with covid yesterday.
“That means spreading already since yesterday was a busy day at church,” said the person.
Giff Johnson is editor of the Marshall islands Journal and the RNZ Pacific correspondent in Majuro. This article is republished under a community partnership agreement with RNZ.
Early carnivals offered political power a safety value. For a few days a year, rich and poor switched positions. The poor ran society (if in ritual only), except, when things were going badly in the everyday, the reversal suddenly turned into open rebellion from below.
In the present pandemic, it’s the powerful who are running a months-long masquerade, taking off masks ironically enough, in the face of all the evidence that the pandemic is marching on and mask mandates in combination with vaccines and other interventions can protect populations from infection.
The ruling class’s public health putsch aims to free a precarious just-in-time capitalism from supply chain gluts and social welfare obligations that a serious pandemic imposes. Better let people get sick or die than violate such a society’s prime directive placing profits first, the political class plots.
SARS-CoV-2, the COVID-19 virus, is cycling through new variants every two months, tinkering with both the human immune system and our already precarious vaccine coverage. The reduced deadliness the virus seems to represent at the moment, as some experts pronounce, isn’t a set outcome. It’s only one of multiple possibilities. As the hospitalizations, which doubled under the BA.5 variant underscore, sudden surges in virulence are also possible, perhaps even likely as the virus is being left to explore its evolutionary possibilities.
The virus, meanwhile, keeps knocking thousands into the Long COVID side pocket, where patients are lost to complex combinations of chronic conditions that medicine is finding difficult to treat.
The State of the Pandemic
Where are we in the global pandemic? The Johns Hopkins Coronavirus Resource Center reported another 7.16 million new COVID cases worldwide for the week ending July 31 (see the red time series on the right of the John Hopkins dashboard). That’s more new weekly cases than for any other COVID wave except Omicron this past winter.
The number of global weekly deaths underwent another increase to 16,400 deaths the week ending July 31, although representing fewer cases than in previous waves (the white time series on the right of the Johns Hopkins dashboard). Forty-two million new vaccinations were administered that week worldwide (the green time series).
The New York Times is mapping COVID hotspots in the Americas, Europe, Asia and Australasia. There in purple, France, Germany, Austria, Italy, Greece, Taiwan, Australia and New Zealand continue to be epicenters in average daily new cases per 100,000 population. In recent weeks, Costa Rica, Finland, Japan, South Korea, and Thailand all returned to hotspot status. Canada, Mexico, Brazil, Peru, Bolivia, Argentina, Tunisia, Armenia, Kazakhstan, Iran, Iraq and Mongolia hosted recent increases in caseloads. Panama, Botswana, Portugal, Spain and Norway saw declines from late June.
The seven-day average of daily confirmed COVID cases per million people from the beginning of the outbreak shows the present hotspots are trending in different directions. Taiwan and Italy’s outbreaks appear in decline. Greece and Finland are hosting large new spikes. Japan, South Korea, and Mongolia are hosting new surges. Australia, New Zealand, France, Italy and Germany continue to cycle through their months-long epidemics. The U.S., the U.K. and Brazil are reporting slow but steady increases. We see that none of the countries highlighted are reporting national testing data as of July 3 (click on “color by test positivity”).
For the COVID deaths per million people for these same countries, we see that the U.S., Brazil and Germany are showing slight increases. Italy, the U.K. and Australia are showing more robust increases, and Costa Rica, Finland and Greece are displaying sharp spikes.
The virus also continues to evolve. This is a family tree for COVID samples over the past six months, although, for the radial version of the tree, rooted from the beginning of the pandemic at the center of the diagram and branching outward as SARS-2 evolves. We see in dark blues and purples the early variants like Alpha and Beta. In the light blue are samples of the Delta variant. We see over the past six months that multiple Omicron subvariants — there in yellow BA.1 and 2, in the light and medium oranges BA.4 and 5, and the darker orange BA.2.12 — are continuing to explore SARS-2’s evolutionary space. Indeed, we see in the few red samples the arrival of subvariant BA.2.75 or the Centaurus variant found first in India in June.
Across the Omicron group, we find molecular changes from the root of the SARS-2 tree here numbering as high as 64 amino acid changes and 16 deletions. What that means is that the virus continues to evolve, along the way experimenting with the human immune system to the tune of over 7 million new infections a week during what governments worldwide are treating as the end of the pandemic.
Hospitalizations are all up in the countries in our highlighted set. These appear as a function of the surge in caseloads, the reemergence of deadlier subvariants such as BA.5, and a developing mismatch between Omicron and COVID vaccines. We also see across countries in our set a near-global retraction in nonpharmaceutical interventions since Omicron. These indices of the stringency of public health measures show that some countries at first attempted to differentiate masking mandates and the like for the vaccinated (in green) and for the unvaccinated (in brown) before largely abandoning that distinction.
That combo — evolving subvariants probing our defenses and a willful public health surrender — bodes ill for this winter’s likely surge.
The U.S. Outbreak
As of August 7, the U.S. continues to host a raised floor in COVID-19 caseloads post-winter Omicron. This summer marks the worst in U.S. COVID-19 incidence of the three summers so far in this pandemic.
The New York Times map shows Northeast and upper Midwest are presently characterized by a relative decline in COVID. But we also see the start of a possible new surge in New Jersey, New York City and now, Pennsylvania. We see sharp spikes in Appalachia, particularly in Kentucky and West Virginia. The South is hosting lifted floors, especially in North Carolina, northern Louisiana, the Florida panhandle, Miami, parts of Alabama and Georgia, Oklahoma overall, and select counties in west and south Texas. We see a slight decline along the West Coast, a steady surge in parts of the Southwest, and sharp spikes county-by-county across the Plains states. Alaska and Puerto Rico continue to be hit badly.
There are other ways of tracking COVID. The levels of SARS-2 virus detected in the wastewater that comes through our sewage plants as reported here (July 19-August 2) shows little change from earlier in July. Sewage plants in red represent loads at 80 to 100 percent their previously recorded levels. We see these scattered across the U.S., but especially in Nebraska, Illinois, Ohio, Kentucky, South Carolina and downstate New York. The cool blues of recorded lows in the Northeast are starting to be infiltrated by increased SARS-2 concentrations in orange from New Jersey up north. We do see cooling off in coastal Washington State, Oregon and northern California.
The map of percent change in the last 15 days underscores the West Coast’s cooling off. We see such declines in light blue of 10 to 90 percent across Utah, Colorado, Nebraska, and what we were worried about in the first wastewater map in downstate New York. These might represent only mean declines off very large peaks that still host widespread COVID. At the same time, we see new 15-day surges in Illinois, Ohio, upstate New York, Kentucky and North Carolina.
A standing problem in tracking COVID-19 stateside is that the U.S. appears to be willfully ignoring previous surveillance measures. In April, ABC News and other outlets reported that the Department of Health and Human Services ended the requirement that hospitals report daily COVID deaths, overflow and ventilated COVID patients, and critical staffing shortages. Some U.S. states outright ended reporting COVID metrics, hospital bed usage and availability, and ventilator use. Some states turned to delaying COVID-19 numbers to reports on a weekly basis.
The ABC News report continued that some hospitals are following the National Institute of Health’s lead in changing definitions of COVID cases, including to only those patients that receive antivirals remdesivir or dexamethasone. So COVID cases wouldn’t be counted unless the patient needed those drugs.
It appears the willful decline in monitoring is beginning to extract its public health costs. For instance, we see here in San Francisco that previously SARS-2 loads in sewage (in blue) tracked COVID caseloads (in red). That appears no longer to be the case, with COVID caseloads during BA.4 and 5 likely to be underreported.
To sum up U.S. COVID, we see almost the entire country — 94 percent of U.S. counties — under “Data Type: Community Transmission” in the CDC maps is filled in at the highest level of community transmission, including what were a month ago sites of COVID decline in Iowa, Pennsylvania and New York State. The summer surge is accumulating with much of the country still reporting in COVID-19 tests at 20 percent or more positive (click on “Nucleic Acid Amplification Tests (NAATs)”). And much of the country — especially through the South, Appalachia and the Plains states — with less than 30 percent of the population with two COVID vaccine shots, even before including subsequent boosters (click on “Vaccinations” on the left and “% of total population fully vaccinated” on the right).
Monkeypox Marks Another Roll of the Epidemiological Dice
As on the global stage, SARS-2 continues to evolve here in the U.S. We see here new variants first emerging and then dominating in cycles of every two months. The BA.2 Omicron subvariant in pink was replaced by the BA2.12 subvariant in orange, which is now being replaced by subvariants BA.4 and 5 in green, with BA.5 surging ahead to account for over 85 percent of new cases as of July 30.
Each new COVID variant marks the U.S.’s — and the world’s — concerted failure to control infectious disease. Entirely new pathogens underscore the point. Monkeypox — a previously marginal Orthopoxvirus that can induce at times very painful lesions in the anus, genitals and mouth — has spread to all but two U.S. states, with patients getting little access to follow-up care or the vaccines that at best offer disease mitigation.
Epidemiologist Kathryn Jacobsen reports that the federal government’s recent declaration that monkeypox represented a U.S. public health emergency opens up more of such resources. The declaration, while welcome, is a month too late from helping quash an outbreak once limited to a few urban epicenters. The declaration also serves more as a guideline for local public health departments as to reporting and treatment, but not how to intervene or to help the greater community respond, with schools about to reopen at the end of August.
That is, the failures of the COVID response stateside have been set on repeat. The damage isn’t merely a matter of the surprise of a new outbreak or which political party is in power. The fiasco is systemic and extends back into the disease cascade.
Each new emergent pathogen represents a roll of the socioecological dice. Deforestation and development in the far reaches of capitalist production are springing even the most marginal pathogens out onto global trade and travel networks to reach countries that have taken great pride in destroying their own public health systems in the name of open economies.
Here, Rebecca Levine’s team maps its ecological niche model of monkeypox distribution across Sub-Saharan Africa, including in a Congo Basin that since has suffered considerable deforestation, especially there in the purple.
While most land deals underlying extraction in the Congo Basin are European and Asian in origin, the Land Matrix Observatory identified seven deals with direct American investment, including a 348,000-hectare deal with U.S.-registered Congo Emissions Management and Groupe Blattner Elwyn. Although this latter deal appears to be pursued under the rubric of carbon offsets, such agreements in green capitalism score their damage in helping rationalize offshore capital’s right to the Global South.
Many of the European and Asian efforts in the Congo and across West Africa meanwhile end up supplying U.S. customers, including wood siding to retailers Home Depot and Menards.
The defacement only compounds in its effects. When the Global North refused to follow through with a promised $500 million to the Democratic Republic of the Congo (DRC) to preserve its rainforest, the DRC, looking to Angola and Nigeria’s path of development, turned to auctioning off its forest to oil companies, including Virunga National Park, the critical gorilla sanctuary.
Monkeypox in the U.S. may be a matter of blowback. It’s not that any one of these land deals let loose this strain of the virus, but that pathogens are in part sprung when this model of development turns food forests into cleared land and expropriated resources marked by a loss in the environmental complexity that once bottled in those pathogens.
Two Additional Dangers
The capital-led destruction is also found on this side of disease spillover. Two additional dangers other than acute infections and deaths — the latter now projected at 17.5 million or more — arise from letting SARS-2 run free.
The first is that the virus may experiment enough to figure out how to emerge from our vaccines’ disease immunity — the protection the vaccines offer us from getting too sick when we’re infected.
One Dutch team of microbiologists produced what’s called an antigenic map to track vaccine coverage. The map on the left shows that the Omicron subvariant BA.1 evolved out from underneath the protection provided by being infected with earlier variants like Alpha, Beta and Delta. The map on the right tracks the antibody neutralization the vaccines provide in comparison to the circulating COVID variants. That map shows Omicron (in pink) has escaped the antibodies produced by the vaccines we’ve used to this point.
That doesn’t mean the vaccines are useless, just that they don’t necessarily produce all the Omicron-specific antibodies.
Moderna is reporting its Omicron-specific vaccine in development to be successful. But we are likely in for boosters for years, with no guarantee a SARS-2 on a two-month schedule won’t continue to evolve out from underneath that protection.
The second danger is the Long COVID any one infection may induce or, perhaps, the cumulative impact of multiple COVID infections. A Weill Cornell Medicine team recently summarized the damage: On the left, the little graphs in red show the hazard ratios of all the body systems that have been documented to be impacted.
The “Long” in Long COVID isn’t just the length of time of such an infection, but also represents a foundational transition from an acute respiratory infection to a chronic condition of often devastating impact. We’re talking about various combinations of cognitive impairments, ulcers, pulmonary fibrosis, embolisms, diabetes, fatigue, and many more illnesses in the list to the left of the human figure shown.
To the right of the figure, we see all the different drugs Long COVID patients are found to be at a higher risk of having to take.
That’s why the People’s CDC — the coalition of public health practitioners and everyday people I’ve joined — is adamant that all efforts must be made to implement a full array of public health interventions that keep all people, whatever their starting health, from entering the horror of Long COVID.
Biden’s Mask Off Shows Us Another Trump
In contrast, a Biden administration elected to volte-face Trump on COVID turned its position 360 degrees back to Trump positions. In the face of an adaptive and ongoing pandemic that is producing nearly 7 million new infections a week worldwide and Omicron subvariants evolving out from under vaccine coverage, the Biden administration decided to declare victory on COVID-19.
NBC Newsreported that in February, Impact Research, the administration’s polling firm, recommended moving beyond merely dropping mask mandates and by default toward discouraging mask use.
Molly Murphy and Brian Stryker of Impact suggested that the administration make a play for November’s midterm elections and “declare the crisis phase of COVID over and push for feeling and acting more normal.” In what seem to be talking points from the problematic “Urgency of Normal” campaign that encouraged moving students back into schools without adjunct interventions, Murphy and Stryker cited learning loss at school and COVID’s effect on the economy as reasons to exit COVID as a reality.
Both problems arose out of decisions the Trump and Biden administrations made in refusing to provide adequate support for communities and households alike during a national crisis. At the same time, the Impact memo continued, aiming to eliminate COVID isn’t the answer. In effect, with language reminiscent of Trump’s Chief of Staff Mark Meadows, the memo admits that COVID will remain the reality, which Murphy and Stryker also suggest the Biden administration ignore.
The CDC, other administration officials, and outside epidemiologists would follow up the memo by warning the American people of upcoming COVID spikes, including this fall and winter when Americans go to the polls.
Such realities are socially structured. In early July, Anna Peele interviewed the soon-to-retire Anthony Fauci for the Washington Post magazine, under the headline, “The Pandemic Is Waning”:
I am also aware that it would be a moral crime to transmit the coronavirus to Fauci. So when I got COVID two weeks before our interview, I obsessively parsed the guidelines from the Centers for Disease Control and Prevention: As long as I waited 10 days after my first positive test, I could still meet Fauci in person, right? No, I was informed by Fauci, via a member of his communications team. I would need to test negative three days in a row and wear a mask, even outdoors.
So, no five-day quarantine for Fauci’s circle along the lines a CDC under employer pressure recommended for Americans. And Fauci treats the possibility of infection after 10 days as real. These are exactly the kinds of precautions the People’s CDC recommended for the rest of the country.
When Biden finally contracted COVID, showing up to work maskless while infected, CDC Director Rochelle Walensky took to the airwaves saying that, yes, the president would be treated with precautions above and beyond what the CDC recommended for the American people. After all, the Americans whom the administration abandoned make up the labor force that chooses to go to work sick or alongside sick coworkers. The CDC is only accommodating them:
Yeah, I think we can all agree that the president’s protocols likely go above and beyond and have the resources to go above and beyond what every American is able and has the capacity to do.
As we put forward our CDC guidance, we have to do so so that they are relevant, feasible, followable by Americans, and that is Americans that live in urban jurisdictions and rural jurisdictions, that have resources and less resources, that have, you know, work constraints and many other things. So, when we put forward our guidance, we do so so that they reflect such that every American is able to follow them.
A growing class divide, which mainstream public health must accommodate first and foremost in the folksiest of fatalism, is treated as more sacrosanct than the obligations to control and prevent an infectious pandemic.
The resulting damage is unlikely of any American’s choosing. “For the period from June 29 to July 11 [2022],” the Wall Street Journal reported, “3.9 million Americans said they didn’t work because they were sick with Covid-19 or were caring for someone with it, according to Census Bureau data. In the comparable period last year, 1.8 million people missed work for those reasons.”
Even steps forward act to fill in such continuing damage. The administration recently announced it would be establishing a new Department of Health and Human Services office dedicated to addressing the debilitating Long COVID that an estimated 23 million Americans are suffering beyond their initial acute infections. An associated National Research Action Plan on Long COVID is to be pursued alongside the administration’s efforts to “return to normal” and strip out programs in COVID prevention.
In other words, the supply of extremely difficult-to-treat Long COVID cases the administration now says it seeks to mitigate will continue apace to accommodate employers.
When Pandemic Play Turns Serious
Given the bipartisan push to end COVID as an idea (if not as an empirical fact), science writer Ed Yong’s sense of defeat may be more an acknowledgement that a different public health is possible. And that it’s already underway, with a passing reference to the People’s CDC:
In 2018, while reporting on pandemic preparedness in the Democratic Republic of Congo, I heard many people joking about the fictional 15th article of the country’s constitution: Débrouillez-vous, or ‘Figure it out yourself.’ It was a droll and weary acknowledgment that the government won’t save you, and you must make do with the resources you’ve got. The United States is now firmly in the débrouillez-vous era of the COVID-19 pandemic…
I have interviewed dozens of other local officials, community organizers, and grassroots groups who are also swimming furiously against the tide of governmental apathy to push some pandemic response forward, even if incrementally. This is an endeavor that all of American society would benefit from; it is currently concentrated among a network of exhausted individuals who are trying to figure out this pandemic, while living up to public health’s central tenet: Protect the health of all people, and the most vulnerable especially. The late Paul Farmer, who devoted his life to providing health care to the world’s poorest people, understood that when doing such work, victories would be hard-won, if ever won at all. Referencing a line from The Lord of the Rings, he once said, ‘I have fought the long defeat.’ In the third year of the COVID pandemic, that fight will determine how America fares against the variants and viruses still to come.
What Yong misses in his respectable summary is that the resulting patchwork isn’t just a reminder of what we have lost or what we might gain upon a reformation of a pivot, but perhaps a new world born out of the husk of the old.
With death and illness accumulating from one COVID variant to the next, and now with novel pathogen species like monkeypox joining the party, the ritualized protest that the capitalist carnival allows may suddenly lurch into open rebellion. Millions may organize to burn down that Venn diagram of going to work in an apocalypse. There is another option: they can refuse to get sick and die for profit’s sake.
22 May 2018 Dr Ashley Bloomfield was named as the new Director-General of Health while he was serving as the acting chief executive of Capital and Coast District Health Board.
2019 The health system faced some big challenges in 2019. Dr Bloomfield fronted health responses to both a measles outbreak and the Whakaari/White Island disaster.
27 January 2020 “Kia ora koutou katoa, welcome to the Ministry of Health, thank you very much attending this briefing this afternoon. My name is Dr Ashley Bloomfield, I’m the Director-General of Health.”
After two and a half years of a pandemic, it is probably hard to remember a time when Dr Ashley Bloomfield needed to introduce himself.
Before New Zealand had its first case of covid-19, back when it was referred to simply as a coronavirus (WHO would name it covid-19 on 12 February 2020), Dr Ashley Bloomfield and Director of Public Health Dr Caroline McElnay held a media stand-up.
Like most of the early briefings, it was held at the Ministry of Health.
It was two weeks after the first confirmed case outside of China had been identified and across the ditch, Australia had four cases. There had been 56 deaths worldwide.
28 February 2020 Almost exactly one month later, New Zealand’s first covid-19 case was confirmed in someone that had returned from overseas.
Reminiscent of a format we would come to know more intimately as time went on, the evening news would cut to a live press conference where Dr Bloomfield and then-Health Minister David Clark would provide more details of New Zealand’s first case. (Prime Minister Jacinda Ardern was in Australia at the time.)
The following day, supermarkets would see a rush of customers buying up toilet paper, hand sanitiser and tinned food.
March 2020 We would start to hear a lot more from Dr Bloomfield as the second, third and fourth (who had been at a Tool concert) cases of covid-19 were confirmed in early March.
By the end of the month New Zealand would be in lockdown and Dr Bloomfield had become a daily part of our lives.
“It did feel a little bit like I was having a performance review at one o’clock every day, broadcast live on television. But that’s as it should be — your job is to ensure that we’re being held accountable for our response,” he said.
PM Jacinda Ardern and Dr Ashley Bloomfield … creatively captured from a daily 1pm update fan. Image: RNZ
Daily cases had jumped to numbers in the eighties and the briefings had shifted to the Beehive, against a backdrop of yellow and white striped Unite Against Covid-19 branding.
On 29 March, during the 1pm briefing, Bloomfield would announce New Zealand’s first covid-19 death.
4 May 2020 “No new cases”. For the first time since New Zealand went into level 4 lockdown on 25 March, Dr Bloomfield announced there were no new cases of covid-19. It would be a phrase we would hear more of as the first community outbreak would start to slow.
And it evoked such emotion that “There are no new cases of covid-19 to report in New Zealand today” came second place in Massey University’s Quote of the Year.
August 2020 In an effort to encourage people to test for covid-19, Dr Bloomfield had his first covid-19 PCR test while filmed at a community testing site.
“It was much less painful than tackling Billy Weepu on the rugby field a couple of weeks ago.”
*Raises eyebrows With millions of people stuck at home in isolation watching daily media briefings, it was no surprise that Dr Bloomfield would find himself in meme-territory.
This was Dr Bloomfield’s response when he was asked about 5G in 2020:
Dr Ashley Bloomfield being asked about 5G conspiracy theories on April 8 vs Ashley Bloomfield being asked about bleach injections on April 26. Image: RNZ
And a year later when Covid-19 Response Minister Chris Hipkins said people should go outside and “spread your legs”.
The Guardian on the Hipkins quote.
Festival debut Who would have thought Dr Bloomfield would grace the main stage at Rhythm and Vines festival?
Unstoppable summer video.
December 2020 Dr Bloomfield was awarded the New Zealand Medical Association’s highest accolade — The Chair’s Award
Fan art for Dr Ashley Bloomfield. Image: Sam Rillstone/RNZ
17 August 2021 The prime minister announced another nationwide lockdown after a case, assumed to be the delta variant, was detected. That meant the 1pm briefings, and daily doses of Dr Bloomfield, were back too.
22 September 2021 As New Zealand tackled the delta outbreak, Dr Bloomfield broke the news that we may never get to zero cases of covid-19.
A portrait pie of Dr Ashley Bloomfield. Image: Devoney Scarfe/RNZ
A portrait pie of Dr. Ashley Bloomfield. Photo: Supplied / Devoney Scarfe
October 2021 During Super Saturday, Dr Bloomfield was caught on camera busting a move at one of the community events.
“It seems we’re at a good point in terms of the pandemic, the response is shifting, I’m also confident that the system is in good hands with the changes that are afoot, and most certainly my family will be very pleased to have a little more of my time,” he said.
May 2022 Dr Bloomfield tested positive for covid-19 while he was at the World Health Assembly in Geneva, Switzerland.
Professional history
In May 2018, Dr Bloomfield was appointed the new Director-General of Health.
Dr Bloomfield was the acting Chief Executive for Capital & Coast District Health Board from 1 January 2018.
From 2015-2017, he was chief executive of the Hutt Valley District Health Board – the first clinician to lead the Hutt Valley District Health Board.
In 2017 Dr Bloomfield attended the Oxford Strategic Leadership Programme.
Prior to becoming chief executive at the Hutt Valley DHB, Dr Bloomfield held a number of senior leadership roles within the Ministry of Health, including, in 2012, acting Deputy Director-General, sector capability and implementation.
From 2012-15 he was Director of Service, Integration and Development and General Manager Population Health at Capital & Coast, Hutt and Wairarapa District Health Boards.
From 1999-2008 he was a Fellow of the Australasian Faculty of Public Health Medicine. Since 2008 he has been a Fellow of the NZ College of Public Health Medicine.
In 2010-2011 he was Partnerships Adviser, Non-Communicable Diseases and Mental Health at the World Health Organisation, Geneva.
Dr Bloomfield obtained a Bachelor of Medicine and Bachelor of Surgery at the University of Auckland in 1990.
This article is republished under a community partnership agreement with RNZ.
Good news, everyone! The COVID-19/Omicron/BA.5 pandemic is apparently all over! Done! Gone! How do I know this? Because the editorial board of the Murdoch-owned fa-chrissakes New York Post says so. Why? Because President Biden is still alive. “Biden’s mild COVID case is proof the pandemic is over, and everyone should stop pretending otherwise,” reads the headline. All that’s missing is a “So there!” at the end.
I’m just going to splash this on the stoop and see if the cat licks it up… but isn’t it at least possible the president of the United States is recovering so well in part because he’s, well, the president of the United States? With immediate access to the best health care and COVID treatments on the planet? That certainly sounds reasonable, even as an unreasonable number of people do not have such health care opportunities. And the New York Post doesn’t even begin to consider the fact that scores of people exist who have health conditions that render them severely immunocompromised and much more vulnerable to severe COVID than Biden.
“We wish the president a rapid recovery,” announces the opening of the editorial. “So far, it looks like his case is high-profile evidence that the pandemic is completely over — that Americans’ anti-coronavirus efforts should focus exclusively on getting jabs to those who need them and treating cases as they pop up. That means absolutely no mandates — not for mass masking and so on, and not even for vaccination (except perhaps for special cases such as those who care for the elderly).”
Ah, the masks, ye gods and little fishes, the bedeviled masks. Never in human history has such an amalgam of wanna-be tough guys been so thoroughly undone by Band-Aid-level technology. Do the folks on the Post ed. board understand that one of the reasons this nightmare has dragged on for so long is because Donald Trump – aided and abetted by conservative news outlets owned by Mr. Murdoch – went out of their way to shit-talk the use of masks because Trump thought they made him look weak?
Increased infection rates caused by this unconscionable behavior ran headlong into the rise of international variants that dominate the pandemic today, variants now virulent enough to get around the masks. The daily infection rates still tally in the thousands. That’s not “over” by even the most wildly irresponsible metric. It’s a perfect circle.
Trump has been yelling about Jesus a lot lately, and the Fox News empire has long fashioned itself a Christian-friendly organization… but their line on masking is yet another example of their hypocrisy. A major reason to mask was to protect others from you in case you have COVID and don’t know it. Put another way, wearing a mask was a small sacrifice you made to help your neighbor. Unless I read the book wrong, that is pretty much the bone-marrow definition of what Christianity is supposed to be about. The hypocrisy is boggling.
“Even as many of our policymakers have focused on deaths,” writes Kevin Kavanagh, MD for Infection Control Today, “long COVID-19 is continuing to take a toll on society by impacting multiple organ systems. Long COVID-19 has been found to occur in 30% of patients treated for COVID-19, and up to 70% have symptoms of brain fog, memory, or other cognitive problems. It also can have a profound impact on the heart and other organs. Also, long COVID-19 is responsible for approximately doubling COVID-19 deaths with 8.39 per 1000 additional deaths occurring after the acute infection.”
And after hearing this, we are supposed to accept that COVID is “over”?
“Hospitals across the country are grappling with widespread staffing shortages, complicating preparations for a potential Covid-19 surge as the BA.5 subvariant drives up cases, hospital admissions and deaths,” reports Krista Mahr for Politico. “The current wave, in which the new number of patients hospitalized with Covid-19 has risen more than 40 percent in the last month, is also putting fresh stress on facilities as federal funding for the pandemic response is running out, leaving some with less flexibility to hire more staff if they need to…. ‘There is growing concern that this money has run out,’ said Nancy Foster, vice president for quality and patient safety policy at the American Hospital Association. ‘It’s not really getting sufficient attention.’”
Over?
“All over, you say?” I wrote back in June. “Someone forgot to tell that to the preschool-aged son of my dear friend and colleague, a 4-year-old who presented with a viciously spiked fever over the weekend. As with nearly 4 million children in the U.S., my colleague’s child is susceptible to seizures if his temperature rises too high. When the seizure set in this time, he became unresponsive and had to be rushed to the emergency room, which fortunately had room for him. As the medical staff worked to reduce his fever, the diagnosis arrived: COVID-19…. You really can’t peddle the ‘all this is behind us’ bullshit to my colleague with her son in the emergency room this weekend, or to my other coworker whose toddler contracted the virus in February and who had to sit up all night listening as their child labored to breathe.”
And then there’s this, the inconvenient weevil in the porridge: Me, and the millions like me who deal with medical issues that leave us permanently open to being flayed by the virus. For me, it’s bad lungs, a gift from a prior bout of pneumonia. Many others are immunocompromised for a variety of reasons – cancer, heart disease, various disorders – and our lives get a little bit worse, a little bit smaller, a little bit more terrifying, every time a large media microphone coughs out another “reason” for people to let down their guard and act like this is over for everyone.
“This pandemic is done,” proclaims the conclusion of the Post editorial, “and it’s not coming back. We have nothing to fear but fear itself. And anyone still pushing fear (status-seeking ‘experts,’ power-seeking pols, etc.) is almost certainly working an agenda that has nothing to do with your best interests.”
Nice of them to end this with such a rich vein of bullshit. “Working an agenda that has nothing to do with your best interests,” you say? I think I know what that’s like. That’s like working an anti-mask agenda to try and get a terrible Republican president re-elected. That’s like working a viciously capitalist agenda to hurl unprotected workers into harm’s way so the owners and bosses can start making money again.
That’s the same crap we’ve been hearing from the same self-serving nonsense vectors almost since this whole thing began. It is wrong and dangerous all day long.
The covid-19 pandemic has already generated its own mythology. In Britain, they talk of the “myth of the blitz” – the idea of a society that pulled together in the Second World War to withstand the bombs dropped by the Luftwaffe with pluck, bravery and humour.
In Australia, our covid-19 myth is about a cohesive and caring society that patiently endured lockdowns, border closures and other ordeals. Like many myths, ours has some foundation in reality.
It might be a poor thing when considered alongside wartime Britain’s wartime sacrifices, and you have to ignore the empty toilet paper shelves in the local supermarket, but it still has its own force. It might be especially potent in Melbourne, where the restrictions were most severe and prolonged.
The covid-19 myth is now presenting its puzzles to true believers. If you imagined we all pulled together for the common good, and because we have the good sense to look after our own health, you are likely to find it strange that we are now apparently prepared to tolerate dozens of deaths in a day.
More than tolerate: there has been a preparedness to pretend nothing out of the ordinary is happening.
All of this seems a far cry from those days when we hung on the daily premiers’ media conferences and experienced horror as the number of new infections rose above a few dozen a day, a few hundred, and then a thousand or so. Have our senses been blunted, our consciences tamed?
A product of power
Public discourse is never neutral. It is always a product of power. Some people are good at making their voices heard and ensuring their interests are looked after.
Others are in a weak position to frame the terms of debate or to have media or government take their concerns seriously.
The elderly — especially the elderly in aged-care facilities — have carried a much larger burden of sacrifice than most of us during 2020 and 2021. They often endured isolation, loneliness and anxiety.
They were the most vulnerable to losing their lives — because of the nature of the virus itself, but also due to regulatory failure and, in a few places, gross mismanagement.
Aged Care Minister Anika Wells has provided @abcnews with new details on COVID cases in residential aged care homes:
983 current outbreaks
6000+ residents infected
3250 staff are positive
ADF support for aged care homes will be continued until the end of September.
Casual and gig economy workers, too, struggle to have their voices heard. On his short journey to an about-face over the question of paid pandemic leave, Prime Minister Anthony Albanese at first said the payment was unnecessary because employers were allowing their staff to work from home.
Yet the conditions of those in poorly paid and insecure work have been repeatedly identified as a problem for them as well as for the wider community, because they are unable easily to isolate.
Up to his point, however, our democracy has spoken: we want our pizzas delivered and we want to be able to head for the pub and the restaurant. And we are prepared to accept a number of casualties along the way to have lives that bear some resemblance to those of the pre-covid era.
The “we” in this statement is doing a lot of heavy lifting. There is a fierce debate going on about whether governments — and by extension, the rest of us — are doing enough to counter the spread of the virus.
Political leadership matters
Political leadership matters enormously in these things.
In the years following the Second World War, Australia’s roads became places of carnage, as car ownership increased and provision for road safety was exposed as inadequate. It peaked around 1970, with almost 3800 deaths — more than 30 for every 100,000 people.
Road fatalities touched the lives of many Australians. If not for the death of my father’s first wife in a vehicle accident on New Year’s Day in 1954, I would not be around to write this article today.
In the 1960s and 1970s, the coming of mandatory seatbelt wearing and random breath-testing helped bring the numbers down. Manufacturers made their cars safer.
Public campaigns urged drivers to slow down and stay sober. These were decisions aimed at avoiding avoidable deaths, despite the curtailment of freedom involved.
A British seat belt advertisement from the 1970s.
These decisions were also in the Australian utilitarian tradition of government, “whose duty it is to provide the greatest happiness for the greatest number” – as the historian W.K. Hancock famously explained in 1930.
The citizen claimed not “natural rights”, but rights received “from the State and through the State”. Governments made decisions about how their authority could be deployed to preserve the common good and protect individuals — from themselves as well as from others.
Pragmatic position
Governments have during the present surge so far been willing to take what they regard as a pragmatic position that the number of infections and fatalities is acceptable to “the greatest number”, so long as “the greatest number” can continue to go about something like their normal lives.
But this utilitarian political culture also has its dark side. It has been revealed persistently throughout the history of this country — and long before anyone had heard of covid-19 — as poorly equipped to look after the most vulnerable.
The casualties of the current policy are those who have consistently had their voices muted and their interests set aside during this pandemic — and often before it, as well.
These are difficult matters for governments that would much prefer to get on with something other than boring old pandemic management. The issue is entangled in electoral politics — we have just had a federal contest in which major party leaders studiously ignored the issue, and the nation’s two most populous states are to hold elections in the next few months.
Governments also realise that restrictions and mandates will meet civil disobedience.
But covid cannot be wished away. At a minimum, governments need to show they are serious about it to the extent of spending serious money on a campaign of public information and advice on issues like mask-wearing and staying home when ill.
They usually manage to find a sufficient stash of public money ahead of each election when they want to tell us what a beaut job they’ve been doing. They might now consider whether something similar might help to save lives.
Nearly 17,000 monkeypox infections have now been reported across 75 countries, and the World Health Organization declared the spread of monkeypox a global emergency. Meanwhile, the U.S. has stopped short of declaring a public health emergency even with nearly 3,000 cases reported in 44 states. New York alone has reported 900 cases of monkeypox, with rollout of the vaccine inhibited by short supply. We speak to Joe Osmundson, professor of microbiology at New York University, about the queerphobic myths about the viral spread, the global inequity of vaccine distribution and more. “This should have been an easy virus to contain,” says Osmundson. “The immense frustration in our community has been watching hundreds of people get sick, not because they’re having sex, not because of their queer identity, but because they’ve wanted to get vaccinated and those vaccines have not been available.” Osmundson also describes how he helped a friend get treatment for monkeypox. His new book is Virology: Essays for the Living, the Dead, and the Small Things in Between.
TRANSCRIPT
This is a rush transcript. Copy may not be in its final form.
AMYGOODMAN:There have now been more than 17,000 cases of monkeypox infections in at least 75 countries, including the United States. Monkeypox isn’t fatal, but it can cause fever, rashes and extremely painful lesions. It’s most often spread through close, intimate physical contact. On Saturday, for the second time in two years, the World Health Organization declared a global emergency to address the spread. The last time, it was forCOVID-19; this time, for monkeypox. This isWHODirector-General Dr. Tedros Adhanom Ghebreyesus.
TEDROSADHANOMGHEBREYESUS:WHO’s assessment is that the risk of monkeypox is moderate globally and in all regions, except in the European region, where we assess the risk is high. There is also a clear risk of further international spread, although the risk of interference with international traffic remains low for the moment. So, in short, we have an outbreak that has spread around the world rapidly, through new modes of transmission, about which we understand too little, and which meets the criteria in the International Health Regulations. For all of these reasons, I have decided that the global monkeypox outbreak represents a public health emergency of international concern. …
Stigma and discrimination can be as dangerous as any virus. In addition to our recommendations to countries, I’m also calling on civil society organizations, including those with experience in working with people living withHIV, to work with us on fighting stigma and discrimination. But with the tools we have right now, we can stop transmission and bring this outbreak under control.
AMYGOODMAN:Here in the United States, the Centers for Disease Control and Prevention has reported more than 2,800 cases of monkeypox so far across 44 states, with the largest outbreaks in New York, California, Illinois, Florida, D.C. and Georgia. The White House has not declared a public health emergency, that could bolster the U.S. response to the monkeypox outbreak. White HouseCOVIDresponse coordinator Dr. Ashish Jha said, quote, “It’s an ongoing, but a very active conversation atHHS.” That’s the Department of Health and Human Services.
For more, we’re joined by Joe Osmundson, professor of microbiology at New York University, scientist, activist, author of the new bookVirology: Essays for the Living, the Dead, and the Small Things in Between. He’s featured in a newpieceinThe New Yorkerheadlined “The Agony of an Early Case of Monkeypox.”
The piece begins, quote, “On the evening before Juneteenth, Joseph Osmundson, one of my best friends and a microbiologist at N.Y.U., texted me: ‘We think Andy has monkeypox.’ Two nights earlier, our friend Andy, as I’ll call him, had spent hours hunched over in an emergency room with excruciating rectal pain, only to be refused testing. It was his third try in five days. Andy’s anal sores were internal; for patients to qualify for testing, C.D.C. guidelines required the appearance of lesions on the skin. Osmundson needed help.”
Well, Professor Joe Osmundson, that’s the opening paragraph of the piece inThe New Yorker. Tell us where you went from there. And in the process, explain what monkeypox is.
JOEOSMUNDSON:Yeah. I’ll actually start with the second part. Monkeypox is not a new virus. And this is sort of why our community has been so frustrated by the lack of urgency to get us the tools we need to care for ourselves and each other and to prevent this virus. It was discovered in 1958 in animals and was shown in 1970 to exist in humans. It’s a virus that’s related to smallpox. You mentioned earlier that it’s not deadly. It’s not very often deadly, but in this outbreak so far this year, there have been five deaths, all of them in the endemic region between Congo and Nigeria. It’s a virus that is similar to smallpox but less dangerous. But it causes pockmarks all over the body, high fever. The lesions can be in the throat or on the mouth, inside the anus and rectum. They are excruciatingly painful. And the course of infection typically lasts two to four weeks. And during this time, patients are asked to fully isolate.
So, again, it’s a pretty miserable virus, although it’s not very often deadly. The frustration has been that because it’s so closely related to smallpox, we actually, prior to this sort of explosion of monkeypox outside of the endemic region — we haveFDA-approved tests, we haveFDA-approved medications that are likely to help ease suffering, and, most importantly, we have vaccinations that can prevent infection. So we have all of the tools, and yet all of these tools have been exceedingly difficult to access, even for someone like Andy, who has a Ph.D., has friends who are working on the response. I mean, it took direct phone calls to contacts in the New York City Department of Health and in the federal government to get him tested. And then, once he was tested and presumed positive, it took another few days to get him access toTPOXX, which is, again, anFDA-approved medication that we thought would help. Once he did getTPOXX, he went, in 24 hours, from being in the most pain of his life to the pain easing. And within five or six days, all of his lesions had healed, and he was cleared to leave isolation.
So, the good news is we have the tools both to prevent infections and to ease suffering. The immense frustration in our community has been watching hundreds of people get sick, not because they’re having sex, not because of their queer identity, but because they’ve wanted to get vaccinated and those vaccines have not been available.
AMYGOODMAN:I mean, we’re here in Chelsea, New York, and this is where people lined up around the block to get vaccines, but there simply weren’t enough.
JOEOSMUNDSON:That’s right. And that, you know, the rollout in New York, has gotten a lot of criticism. And, you know, the New York City Department of Health didn’t reach out to community partners prior to that. They just wanted to get shots into arms prior to Pride weekend. They’ve been listening to us about how that didn’t go well, and they are trying to do better. They are reaching out to more community-based organizations. They’re trying to have more vaccine equity in nonwhite, less affluent communities than the Chelsea community. But, you know, they are incredibly limited. You cannot have equity when vaccine is so scarce. It’s just not possible.
AMYGOODMAN:I wanted to turn to the protest that occurred last Thursday here in New York.ACTUP New York organized an emergency march against monkeypox and government failure in New York City. This is Cecilia Gentili, founder of Transgender Equity Consulting, speaking at the rally.
CECILIAGENTILI:Sex workers are again being forced to the impossible situation of choosing between prioritizing their health or having enough money to survive. Sounds familiar. Yes. The same [beep] happened a couple of months ago withCOVID. What did the government do? Almost nothing. What is the government doing now? Almost nothing. I am so tired of getting almost nothing from the federal government.
AMYGOODMAN:Professor Joe Osmundson, if you can say what needs to happen? I mean, this weekend, you have Congressman Adam Schiff demanding that more be done. You have Ashish Jha on the weekend news shows saying they haven’t decided whether to make the — call this a national emergency in the U.S. And if it were called an emergency, what would that unleash?
JOEOSMUNDSON:Yeah, it would just increase the amount of funding and tools available. There’s a couple of things going on here. One is the scientific response, the biomedical response, that is absolutely lacking. There is no urgency. This should have been an easy virus to contain. UnlikeCOVID, unlike many other emerging threats, we have all of the tools. They are in a stockpile. The point of that stockpile is that it’s meant to be there to respond to an emergency. Here we have an emergency, and the stockpile has not been activated. We found out that vaccine sits in the stockpile in such a way that it can’t actually get into people’s bodies. And vaccine in a freezer is useless. So, we need resources to mobilize the national stockpile that we have to help us, to keep us safe, to treat us when we’re ill.
But we also know — look,COVIDis — you know, a lot of us, by now, have doneCOVIDisolation, 10 days, even five days. It is incredibly difficult. It is costly. Sometimes you miss out on work. Sometimes you have to get a hotel to isolate in. It is really difficult to do. Here we have an isolation with monkeypox that is two to six weeks. That is incredibly disruptive for people’s lives. We’ve been having to crowdfund to get people the money that they need to take time off work. We need emergency funds and hotel rooms so people can properly isolate to prevent the spread. And none of that, none of those funds and resources have been coming from any level of government.
In addition, there are essential scientific questions: Is the virus present in semen? Can we develop new tests that don’t require a skin lesion? Can we test saliva during the early-on flu-like illness? These are obvious questions. And without the proper funding, it will take too long to answer them. The ideal is we get these scientific questions answered as rapidly as possible; instead of skin lesion tests, we have really good saliva tests; if you think you have monkeypox, you can go in, get a saliva test in your flu-like illness, getTPOXXimmediately, and maybe you don’t even get an outbreak of skin lesions, or if you do, you suffer much less, and you’re much less likely to spread the virus. And just, I mean, the vaccine is the most ridiculous thing. There are people who wanted to get vaccine, and now instead of getting vaccine, they have monkeypox.
AMYGOODMAN:Professor Osmundson, this whole controversy over whether to call this a sexually transmitted disease — you can also get it just in close breathing contact, isn’t that right?
JOEOSMUNDSON:That’s right. It’s a very tricky, you know, question. And there are obviously STIs that don’t require sex to transmit them, like herpes. But I’m really worried. We’re already seeing this pushback of, “Oh, if monkeypox is anSTI, why are we seeing it in children?” — sort of, again, doing the groomer thing, implying that queer people are having sex with children. This is incredibly, incredibly dangerous.
This is a virus that commonly spreads throughout households when it’s in households. It is on sheets. It’s on towels. It’s on clothes. And we need to be aware of those nonsexual modes of transmission, so that if it pops up in a wrestling team or a massage parlor or a Broadway show where someone is handling costumes all the time, we actually — that’s on our radar, and we can diagnose it in those places and prevent spread there. I think it’s a little bit myopic to be so focused on sex and the queer community. WeAs Monkeypox Spreads, US Vaccine Access Is Pitifully Inadequate need to be curious and open to the many places this virus may spread.
AMYGOODMAN:Finally, Professor Osmundson, let’s talk about the issue of global equity. There is a severe lack of vaccine here in the United States, but multiply that many times over. Talk about the rest of the world.
JOEOSMUNDSON:This was a choice. This international outbreak was a choice. The United States government let 28 million doses of the modern smallpox vaccine,JYNNEOS, expire and get binned from the national stockpile, as opposed to being used in the endemic regions, from Congo to Nigeria, where people commonly are getting monkeypox. I was on a webinar with the head of the NigerianCDC, who laughed when I asked, “What countermeasures do you have? Do you have vaccine? Do you have treatment?” They have nothing. If in Nigeria, where there’s been an ongoing outbreak of human-to-human spread of monkeypox since 2017, if they had countermeasures there to care for this painful infection there, it’s likely that we may have prevented the international spread of this virus.
Infectious diseases show us that borders are meaningless. Viruses will spread because people interact around the world. It is our obligation to care for human suffering everywhere, not just because it will prevent us from potentially getting sick, but because human suffering is human suffering. So there is absolutely an issue with countermeasures, including vaccine and treatment globally. And capitalism does not set us up well to care for everybody. It is not a way to make a profit. But in our increasingly warming and increasingly interconnected world, we are going to see more of these crises. This is not a viral crisis; this is a crisis of late capitalism. a AMYGOODMAN:Joe Osmundson, I want to thank you for being with us, professor of microbiology at New York University, scientist, activist, author of the new book Virology: Essays for the Living, the Dead, and the Small Things in Between. We’ll also link to thatpieceinThe New Yorkerthat features Professor Osmundson.
When we come back, we speak with California Congressmember Ro Khanna about his efforts to address the ongoing infant formula crisis impacting working-class families and parents of color, to stop the price gouging. Stay with us.
After leading the Aotearoa New Zealand’s covid-19 response for the last two years, Dr Ashley Bloomfield is stepping down from the role of director-general of health at the end of this month.
The softly spoken public servant became a household name early in the pandemic, his image gracing T-shirts, tote bags, mugs and even tattoos.
Having been appointed to the director-general role in mid-2018, Dr Bloomfield was officially set to finish his five-year tenure in June 2023 — but decided to resign from the “complex and challenging” role early.
His last day on the job will be on Friday, July 29, at which time Dr Diana Sarfati will be acting Director-General of Health until a permanent appointee takes up the position.
“We’ve seen over the last week it’s levelled off which is great,” he told RNZ Saturday Morning’s Kim Hill.
His plans for an epic “karaoke party” farewell were already derailed by the recent rise in Omicron cases, but he said caution is the way to go until things settle down.
Pandemic legacy
“I didn’t want my legacy in the pandemic to be taking out some of our tip-top politicians and the leadership of the health sector at a super-spreader event.”
But while Dr Bloomfield is leaving, the crisis he presided over is very much ongoing.
It was announced Friday that primary schools are expected to move from encouraging mask wearing to enforcing it again when Term 3 starts Monday.
While the change may be frustrating for some, covid-19 requires flexible responses, he said.
“I think there will be a high level of general acceptance of the role [masks] will play, especially through winter in the future.”
Dr Bloomfield himself caught covid-19 in May at a World Health Organisation conference in Switzerland, where he said he was surprised at the low level of mask wearing.
“There’s this talk about the rest of the world has moved on. Well, they might have moved on in terms of what they’re doing, but the virus hasn’t moved on. It’s creating just as much havoc as it has in the past.
Higher infection rates
“To think in the UK, they’ve got higher rates of infection and hospitalisation than we do even in the middle of summer, that’s something to worry about.
“There is a general commentary — not just in New Zealand but elsewhere — that we’re moving on, we’re living with covid.”
That’s premature, he said.
“The virus isn’t done with us yet. We’re still in a pandemic. The WHO [World Health Organisation] hasn’t withdrawn that categorisation and the virus continues to evolve,” he said.
“We’ve just got to keep our wits about us.”
Dr Bloomfield … the vaccine rollout ultimately succeeded in its goals. Image: RNZ/Ross Giblin/Stuff/Pool
Pressures ‘always there’ There have been many stories about the strain on emergency rooms and doctors and nurses the past few weeks, but Dr Bloomfield defended the response.
“The pressures that are on the health system now are always there and they’re not unique to New Zealand,” he said.
“I would say we were better prepared this winter than we’ve ever been any winter.
“We also knew that after two years of no flu, we would have a heavy flu season.”
Dr Bloomfield rejected claims that the health system was caught by surprise by the omicron surge.
“We certainly had time to prepare and did. But you can’t suddenly magic up a new workforce from somewhere, certainly not in a situation where a lot of that time the borders were closed, although we were getting new workers in from overseas.”
“Some of the commentary has suggested there are less staff now than there were,” but Dr Bloomfield said there had been a big increase between 2021 and 2022, including nursing and medical staff.
Shortages very localised
Dr Bloomfield said he did not dismiss the views of people on the ground, but said shortages were sometimes very localised.
“I might have a different view from the clinicians on the ground … What one particular clinician or service or institution or organisation might be experiencing might not be reflecting the experience across the system, which is the view I have.”
Dr Bloomfield said for example in the case of PPE, the problem was not supply but in getting the equipment to where it was needed.
“We also responded where we heard, ‘look, we can’t get this PPE here or there,’ then we made sure we would follow those particular problems up.”
There have also been concerns that Māori and Pasifika were not prioritised properly in the vaccine rollout.
Dr Bloomfield said border and health care staff and those over 65 were the first priority for the vaccine drive, but many Māori and Pasifika were also included in that uptake.
“For our first two months of the rollout of the over-65, our highest rates of vaccinations in that group was among Māori and Pasifika. It was ahead of non-Māori, non Pacific.
Younger Māori rates
“We knew that the group that would take the longest, probably because it required repeated effort to build trust, the longest to get higher rates among was our younger Māori. … And that’s the group where we had to put in a lot of extra effort and it took longer to get the rates up, but we did get there.”
That outreach had hopefully led more young Māori to take part in the health system, Dr Bloomfield said.
“There’s now over 100,000 people who previously were not in contact with the health care system who are now on the books because of the efforts that went in through that vaccination programme, so that’s a great legacy.”
Dr Bloomfield has stood at the podium dozens of times in the past couple of years, facing the country’s press as he updated the state of the pandemic for the nation. While at times it hasn’t been easy, he said he respects the media’s role.
“I have to say I’m a big fan of the media being able to do its job properly. It’s a fundamental pillar of strong democracy and it didn’t always feel that way when you were up there facing the music and something had gone wrong, which I had to a few times.
“But they’re doing their job and a big part of their job is making sure the government, including the public services, is accountable to the population.”
Dr Bloomfield and Prime Minister Jacinda Ardern … continuing to work to improve deficiencies in the health system. Image: RNZ/Pool /NZME
‘I was asking, why me?’
As his term as director-general ends, Dr Bloomfield said he’s not interested in becoming a thorn in the government’s side. He’d like to continue to work to improve deficiencies in the system, however: “In my mind the currency I’m interested in is influence.”
If he had known what the last few years held, would Dr Bloomfield have taken the job back in 2018?
“I have to say there were a few moments early on in the pandemic, I really questioned myself on that. I was asking, why me?
“This is a one-in-100 year pandemic and I’ve only got a five-year contract … bad timing,” he joked.
“You quickly forget the parts that were really tough and really challenging,” he noted.
“My abiding memory will be of what a privilege it was to be in this role at this time in this country. I have great hope for the future of this country based on my experience the last four years.”
But he’s still leaving the job a year early, although few would say he hasn’t put in the hard yards.
‘Given my all’
His last child recently left home, and he said: “I feel like I’ve given my all the last four years.”
With big changes happening in the structure of New Zealand’s health system, it seemed a good time to leave.
Dr Bloomfield … hopeful over the changes Health NZ Te Whatu Ora may bring in one of the biggest overhauls of New Zealand’s health system. Image: RNZ/Getty Images
‘Very exciting’ time for health changes Health NZ Te Whatu Ora replaced the country’s 20 district health boards at the start of July.
It’s one of the biggest overhauls in Aotearoa New Zealand history. Dr Bloomfield said he was hopeful for what it might bring.
“There are features of the change that I think are very exciting,” such as the establishment of the Māori Health Authority.
That said, he believes the DHBs served an important role in healthcare.
“The big challenge in any health system is getting this right balance between what’s done at a national or regional level and the responsiveness to local communities, and the DHB model allowed that in some part, that responsiveness to local communities.
“But it was very hard at times to get unity around things that were good for the system. I guess ultimately you’re looking for a system that’s unified but not uniform.
“Certainly Health New Zealand, in the way it’s been set up, is designed to try to get a better balance between that national and local delivery — and that’s a good thing.”
Optimistic about reforms
Dr Bloomfield said he was ultimately optimistic about the reform.
“There’s a risk that you can move the deck chairs around but nothing really changes. The reform has been carefully thought through.
“The proof’s always in the eating of the pudding, so it will be interesting to see how it plays out over the next few years.”
So if Ashley Bloomfield had not been a doctor, what might he have become?
“I always joke with my kids I would have been a police detective. Maybe that would’ve been another career direction.
“I really enjoy observing little bits of information and putting them together to create a picture.
“It served me well in my current career,” he said.
This article is republished under a community partnership agreement with RNZ.
Gwyneth Paige didn’t want to get vaccinated against covid-19 at first. With her health issues — hypertension, fibromyalgia, asthma — she wanted to see how other people fared after the shots. Then her mother got colon cancer.
“At that point, I didn’t care if the vaccine killed me,” she said. “To be with my mother throughout her journey, I had to have the vaccination.”
Paige, who is 56 and lives in Detroit, has received three doses. That leaves her one booster short of federal health recommendations.
Like Paige, who said she doesn’t currently plan to get another booster, some Americans seem comfortable with the protection of three shots. But others may wonder what to do: Boost again now with one of the original vaccines, or wait months for promised new formulations tailored to the latest, highly contagious omicron subvariants, BA.4 and BA.5?
The rapidly mutating virus has created a conundrum for the public and a communications challenge for health officials.
“What we’re seeing now is a little bit of an information void that is not helping people make the right decision,” said Dr. Carlos del Rio, a professor of infectious diseases at the Emory University School of Medicine.
Del Rio said the public isn’t hearing enough about the vaccines’ value in preventing severe disease, even if they don’t stop all infections. Each new covid variant also forces health officials to tweak their messaging, del Rio said, which can add to public mistrust.
About 70% of Americans age 50 and older who got a first booster shot — and nearly as many of those 65 and older — haven’t received their second covid booster dose, according to data from the Centers for Disease Control and Prevention. The agency currently recommends two booster shots after a primary vaccine series for adults 50 and older and for younger people with compromised immune systems. Last week, multiplenews outlets reported that the Biden administration was working on a plan to allow all adults to get second covid boosters.
Officials are worried about the surge of BA.4 and BA.5, which spread easily and can escape immune protection from vaccination or prior infection. A recent study published in Nature found BA.5 was four times as resistant to the currently available mRNA vaccines as earlier omicron subvariants.
Consistent messaging has been complicated by the different views of leading vaccine scientists. Although physicians like del Rio and Dr. Peter Hotez of Baylor College of Medicine see the value in getting a second booster, Dr. Paul Offit, a member of the FDA’s vaccine advisory committee, is skeptical it’s needed by anyone but seniors and people who are immunocompromised.
“When experts have different views based on the same science, why are we surprised that getting the message right is confusing?” said Dr. Bruce Gellin, chief of global public health strategy at the Rockefeller Foundation and Offit’s colleague on the FDA panel.
Janet Perrin, 70, of Houston hasn’t gotten her second booster for scheduling and convenience reasons and said she’ll look for information about a variant-targeted dose from sources she trusts on social media. “I haven’t found a consistent guiding voice from the CDC,” she said, and the agency’s statements sound like “a political word salad.”
On July 12, the Biden administration released its plan to manage the BA.5 subvariant, which it warned would have the greatest impact in the parts of the country with lower vaccine coverage. The strategy includes making it easier for people to access testing, vaccines and boosters, and covid antiviral treatments.
During the first White House covid briefing in nearly three weeks, the message from top federal health officials was clear: Don’t wait for an omicron-tailored shot. “There are many people who are at high risk right now, and waiting until October, November for their boost — when in fact their risk is in the moment — is not a good plan,” said Dr. Rochelle Walensky, head of the CDC.
With worries about the BA.5 subvariant growing, the FDA on June 30 recommended that drugmakers Pfizer-BioNTech and Moderna get to work producing a new, bivalent vaccine that combines the current version with a formulation that targets the new strains.
The companies both say they can make available for the U.S. millions of doses of the reformulated shots in October. Experts think that deadline could slip by a few months given the unexpected hitches that plague vaccine manufacturing.
“I think that we have all been asking that same question,” said Dr. Kathryn Edwards, scientific director of the Vanderbilt Vaccine Research Program. “What’s the benefit of getting another booster now when what will be coming out in the fall is a bivalent vaccine and you will be getting BA.4/5, which is currently circulating? Although whether it will be circulating in the fall is another question.”
The FDA on July 13 authorized a fourth covid vaccine, made by Novavax, but only for people who haven’t been vaccinated yet. Many scientists thought the Novavax shot could be an effective booster for people previously vaccinated with mRNA shots from Pfizer-BioNTech and Moderna because its unique design could broaden the immune response to coronaviruses. Unfortunately, few studies have assessed mix-and-match vaccination approaches, said Gellin, of the Rockefeller Foundation.
Edwards and her husband got covid in January. She received a second booster last month, but only because she thought it might be required for a Canadian business trip. Otherwise, she said, she felt a fourth shot was kind of a waste, though not particularly risky. She told her husband — a healthy septuagenarian — to wait for the BA.4/5 version.
People at very high risk for covid complications might want to go ahead and get a fourth dose, Edwards said, with the hope that it will temporarily prevent severe disease “while you wait for BA.4/5.”
The omicron vaccines will contain components that target the original strain of the virus because the first vaccine formulations are known to prevent serious illness and death even in people infected with omicron.
Those components will also help keep the earlier strains of the virus in check, said Dr. David Brett-Major, an infectious disease specialist at the University of Nebraska Medical Center. That’s important, he said, because too much tailoring of vaccines to fight emerging variants could allow older strains of the coronavirus to resurface.
Brett-Major said messages about the value of the tailored shots will need to come from trusted, local sources — not just top federal health officials.
“Access happens locally,” he said. “If your local systems are not messaging and promoting and enabling access, it’s really problematic.”
Although some Americans are pondering when, or whether, to get their second boosters, many people tuned out the pandemic long ago, putting them at risk during the current wave, experts said.
Dr. Georges Benjamin, executive director of the American Public Health Association, said he doesn’t expect to see the public’s level of interest in the vaccine change much even as new boosters are released and eligibility expands. Parts of the country with high vaccine coverage will remain relatively insulated from new variants that emerge, he said, while regions with low vaccine acceptance could be set for a “rude awakening.”
Even scientists are at a bit of a loss for how to effectively adapt to an ever-changing virus.
“Nothing is simple with covid, is it? It’s just whack-a-mole,” said Edwards. “This morning I read about a new variant in India. Maybe it’ll be a nothingburger, but — who knows? — maybe something big, and then we’ll wonder, ‘Why did we change the vaccine strain to BA.4/5?’”
KHN(Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
When it comes to the world’s two biggest emitters, we are caught between a secretive autocracy and an oversharing corrupted democracy.
Most media attention is focused on the latter. The United States this week raised hopes of a compromise climate spending bill and quashed it again before you could say “Joe Manchin is a bad-faith actor”.
Having somebody to blame does not make it any easier to address a system rigged in favour of fossil fuel interests.
At Climate Home, we bypassed that news cycle (come back to us when you’ve achieved something, America!) and took a longer look at the former.
Because the fact that so little climate journalism comes out of China at a certain point becomes newsworthy in itself. And once Chloé Farand started asking around, we knew this story’s time had come.
It has never been easy for journalists and civil society to operate in Xi Jinping’s China. As he looks to secure a third term as president over the coming months, it is harder than ever.
Beijing’s zero-covid policy is, most sources said, no longer just about public health, but a tool of control at a politically sensitive time. Conferences are cancelled indefinitely and travel restricted. Officials up and down the hierarchy are afraid to speak to the media.
Out of six China-based climate reporters who spoke to Climate Home for the article, four had left or were preparing to leave the country.
This is a problem. Not just for the international community, which has an interest in holding China to account for its emissions performance, but for China. In the vacuum, misinformation and Sinophobia flourish.
From the slivers of news that do emerge, we can see that Chinese experts have much to teach the rest of the world. Ok, so they might want to keep their advantage in mass producing solar panels, but when it comes to smart deployment policy, they have every incentive to share tips.
Perhaps they could give US climate campaigners, who are in despair right now, some fresh ideas.
A prominent New Zealand epidemiologist is calling for much wider mask mandates, saying the roll-out of free masks, while positive, will make a “fairly small” difference to the covid-19 outbreak.
The government yesterday announced masks and rapid antigen tests would be made freely available while the country battled a resurgence of covid-19 and other winter illnesses.
University of Otago’s Professor Michael Baker told RNZ News much more was required to prevent the worst outcomes of a “really grim winter”.
In a statement, the ministry said a child less than 10 years old had died, while five other people who died were in their 70s, nine were in their 80s and eight were aged over 90. Of these people, 11 were women and 12 were men.
All the deaths being reported occurred in the past seven days, the ministry said.
That takes the total number of publicly reported deaths with covid-19 to 1760 and the seven-day rolling average of reported deaths is 20.
Dr Baker said New Zealand needed to shift to becoming a “mask-using society”, which he believed could be achieved only through mandating their use in most indoor environments.
“The very ad hoc approach to requiring mask use is eroding the social licence for them,” Dr Baker said.
“You go to one social event, and everyone’s wearing a mask, and so you feel comfortable. Next day, you go to a different one, and no one’s wearing a mask, except you, and that feels a bit odd. We need to get rid of those inconsistencies.”
Fear of political backlash
Dr Baker said he believed the government had opted for a greater focus on personal responsibility for fear of a potential political backlash.
“Unfortunately, we’ve politicised this issue too much and politics is starting to take over from the science.”
But, speaking to RNZ Checkpoint, Covid-19 Response Minister Ayesha Verrall said it was “not simple” to implement mask mandates.
“It impacts the running of many businesses and we need people to take a pragmatic approach to this.”
Dr Verrall said, however, she would encourage everyone to wear a mask while indoors as much as possible.
She rejected the suggestion the government’s approach to tackling rising covid-19 cases was based on politics over health.
Dr Verrall would not say if the predicted peak of 1200 hospitalisations a day would be a crisis, but said the government was doing everything it could to avoid the scenario playing out.
‘Real health pressures’
“I think it’s really important we respond to the very real pressures in our health system, and I’ve been in close contact with healthcare workers, as well as following the statistics we get to make sure we know what the facts are, and that we respond to them and fix the problems that exist,” she said.
“A lot of what we set out today is designed to do that.”
Green Party MP Teanau Tuiono said the development was “about time”, but he would have liked to see masks made mandatory in schools.
“We’re all over it, we’re all tired… but it’s just no excuse to drop the ball because here’s the thing: there are people still in hospital, people dying from covid,” he said.
“The numbers are going up and we are in the middle of winter, so what we need here is that leadership.”
This article is republished under a community partnership agreement with RNZ.
In response to President Joe Biden’s claim that his administration is “look[ing] at” whether or not to declare a public health emergency over abortion rights, progressive lawmakers are urging him to follow through on the declaration that could free up resources to fight abortion bans.
Biden told reporters in Delaware on Sunday that the declaration is “something I’m asking the medical people in the administration to look at whether I have the authority to do that and what impact that would have.” He said that the strongest action that Democrats could take is to pass a bill that recently failed in the Senate that would codify Roe v. Wade.
The president offered words of encouragement for pro-abortion protesters who have risen up in droves — including outside of the White House over the weekend — in response to the far right Supreme Court’s decision to overturn Roe. “Keep protesting. Keep making your point. It’s critically important,” he said.
Responding to news that Biden is considering the declaration, Rep. Ayanna Pressley (D-Massachusetts) wrote, “Good. Now declare it,” on Twitter.
“Every minute we wait, we risk losing someone we love,” said Rep. Cori Bush (D-Missouri). SCOTUS’ decision to overturn Roe could be a death sentence for our most marginalized communities who already face racism and barriers to health care. [The president] must declare a public health emergency to save lives.”
Pressley and Bush have previously advocated for Biden to declare an emergency to protect abortion access. In a letter sent last month, Pressley led 19 other Black women in Congress in urging Biden to “use every tool at your disposal to protect fundamental reproductive rights and abortion access across this country.” The lawmakers said that conservatives’ abortion bans would especially harm Black people, who already face higher pregnancy death rates than their white counterparts.
Senators Elizabeth Warren (D-Massachusetts) and Tina Smith (D-Minnesota) have also asked for an emergency declaration in order to protect reproductive rights.
A public health emergency declaration would free up funds and government agency resources in order to respond to the crisis. Advocates say that the declaration is crucial so that the government has the authority and the resources to respond to an uptick in demand for reproductive health services.
It seems unlikely that the Biden administration will actually take this step, however. Reporters found last week that top Biden administration officials had already considered declaring a public health emergency after the Supreme Court decision last month and decided against it.
The director of the White House Gender Policy Council, Jennifer Klein, told reporters on Friday that it’s still a possibility, but that the declaration wouldn’t be that effective in responding to the problem.
Meanwhile, Biden has been facing criticism from Democrats and the left for his administration’s inaction on abortion rights so far.
Last week, the president signed an executive order that directs the Department of Health and Human Services (HHS) to research ways to expand abortion rights, like widening access to abortion medication and contraceptives and expanding its family planning services. While it includes some critical provisions like addressing data privacy concerns, abortion advocates said, it’s nowhere near enough to protect the people who will suffer due to the far right’s abortion bans.
Meanwhile, pro-abortion advocates lambasted the White House last week when White House communications director Kate Bedingfield criticized left-wing protesters who have been demonstrating against bans. “Joe Biden’s goal in responding to Dobbs is not to satisfy some activists who have been consistently out of step with the mainstream of the Democratic Party,” she said.
But progressives argue that it is Biden and mainstream Democrats who have been blocking action on abortion rights. After all, just two months ago, Biden had refused to endorse filibuster abolition or reform in order to codify Roe, and only changed his mind after the Supreme Court decision came down — after people had already been affected by state trigger laws that immediately implemented bans.
Quickly delivering donated organs to patients waiting for a transplant is a matter of life and death. Yet transportation errors are leading to delays in surgeries, putting patients in danger and making some organs unusable. This week, we look at weaknesses in the nation’s system for transporting organs and solutions for making it work better.
More than any other organ, donated kidneys are put on commercial flights so they can get to waiting patients. In collaboration with Kaiser Health News, we look at the system for transporting kidneys and how a lack of tracking and accountability can result in waylaid or misplaced kidneys.
We then look at the broader issues affecting organ procurement in the U.S. with Jennifer Erickson, who worked at the White House Office of Science and Technology Policy under the Obama administration. She says one of the system’s weaknesses is that not enough organs are recovered from deceased people – not nearly as many as there could be.
We end with an audio postcard about honor walks, a new ritual that hospitals are adopting to honor the gift of life that dying people are giving to patients who will receive their organs. We follow the story of one young man who was killed in a car accident.
This episode originally was broadcast Feb. 8, 2020.
In May and June of 2022 two milestones were passed in the world’s battle with Covid and were widely noted in the press, one in the US and one in China. They invite a comparison between the two countries and their approach to combatting Covid-19.
The first milestone was passed on May 12 when the United States registered over 1 million total deaths (1,008,377 as of June 19, 2022, when this is written) due to Covid, the highest of any country in the world. Web MD expressed its sentiment in a piece headlined: “US Covid Deaths Hit 1 Million: ‘History Should Judge Us.’”
Second, on June 1, China emerged from its 60-day lockdown in Shanghai in response to an outbreak there, the most serious since the Wuhan outbreak at the onset of the pandemic.
In the shadow of the Davos summit of global elites taking place this week, a new report from Oxfam International details how skyrocketing inequality during two years of the global Covid-19 pandemic surged to a point where a new billionaire was created in the world nearly every day while over one million people are now being pushed into poverty at almost the same daily rate.
The new report — titled “Profiting From Pain” — is the latest accounting of how the pandemic has only deepened grotesque discrepancies between the haves and have-nots of the world, showing that while 573 new billionaires were created since the pandemic began, approximately one billionaire every 30 hours, an estimated 263 million are expected to “crash into extreme poverty” this year — a rate of one million people every 33 hours.
Such stark realities and gross injustice, the anti-poverty group concludes, is clear evidence that a tax on billionaire wealth and windfall pandemic profits is urgently needed to address crucial needs.
For every one billionaire minted since the pandemic began, 1M more people could be pushed into extreme poverty in 2022. While the world is reeling from multiple crises, the world’s wealthiest are unashamedly #ProfitingFromPain of ordinary peopleMorehttps://t.co/47FyVW5b0Upic.twitter.com/rRlKAFv1Nj
“Billionaires are arriving in Davos to celebrate an incredible surge in their fortunes. The pandemic and now the steep increases in food and energy prices have, simply put, been a bonanza for them. Meanwhile, decades of progress on extreme poverty are now in reverse and millions of people are facing impossible rises in the cost of simply staying alive,” said Gabriela Bucher, executive director of Oxfam International.
Among the key findings of the report:
Today, 2,668 billionaires — 573 more than in 2020 — own $12.7 trillion, an increase of $3.78 trillion.
The world’s ten richest men own more wealth than the bottom 40 percent of humanity, 3.1 billion people.
The richest 20 billionaires are worth more than the entire GDP of Sub-Saharan Africa.
A worker in the bottom 50 percent would have to work for 112 years to earn what a person in the top 1 percent gets in a single year.
High informality and overload due to care tasks have kept 4 million women in Latin America and the Caribbean out of the workforce. Half of working women of color in the US earn less than $15 an hour.
While a tall stack of reports has documented such trends since the pandemic took hold in early 2020, Oxfam’s latest study shines a bright light on the massive profits in the key sectors of energy, food, and pharmaceutical companies — all of which are able to consolidate financial gains due to their monopoly control over commodities essential to society.
According to Bucher, the fortunes of the world’s billionaires have “not increased because they are now smarter or working harder” than the average worker, many who faced layoffs, lack of hours, fractured families, childcare crises, and dangerous work conditions throughout the pandemic.
“The super-rich have rigged the system with impunity for decades and they are now reaping the benefits,” she said. “They have seized a shocking amount of the world’s wealth as a result of privatization and monopolies, gutting regulation and workers’ rights while stashing their cash in tax havens — all with the complicity of governments.”
At the same time, she added, hundreds of millions of regular workers and their families “are skipping meals, turning off the heating, falling behind on bills and wondering what they can possibly do next to survive. Across East Africa, one person is likely dying every minute from hunger. This grotesque inequality is breaking the bonds that hold us together as humanity. It is divisive, corrosive and dangerous. This is inequality that literally kills.”
The report notes that the profit margins of the world’s big oil companies doubled during the pandemic, while the cost of energy worldwide is projected to soar by 50% this year — the largest increase in energy prices, the group noted, since 1973. Giant food companies that control a bulk of the world’s food supply and the large pharmaceutical companies, some like Pfizer and Johnson & Johnson which control large portions of the Covid-19 vaccine supply, have been swimming in profits since the virus struck.
Billionaires in the food & energy sectors have seen their fortunes increase by $1B every 2 days while 263M people could be pushed into extreme poverty in 2022 due to the pandemic, inequality & rising food prices. #ProfitingFromPain
With the world’s billionaire class and national leaders meeting in Davos this week as they pretend to meet as stewards of international leadership, Oxfam said there is one clear thing they should do if they want to be taken seriously: support a tax on billionaire wealth.
Among other things, Oxfam calls for a “one-off solidarity taxes on billionaires’ pandemic windfalls to fund support for people facing rising food and energy costs and a fair and sustainable recovery from Covid-19.”
Citing the nearly $8 trillion in tax havens that the global elite is believed to have stashed around the world, the group indicated the global tax system — which has never been defensible — is no longer sustainable in the face of such enormous challenges.
The group is also calling for an end to “crisis profiteering” by introducing a “temporary excess profit tax of 90 percent to capture the windfall profits of big corporations across all industries.” Oxfam estimates that such a tax on less than three dozen “super-profitable multinational companies” could have generated $104 billion in revenue in 2020 alone.
Lastly, Oxfam says a permanent tax on extreme wealth and the disruption of monopoly power by huge multinationals is essential to equalize the world’s economy, lift billions of people out of poverty, and to fund the kind of investments on healthcare, climate action, and social protection for all the low- and middle-income people of the world.
“The extremely rich and powerful are profiting from pain and suffering. This is unconscionable,” said Bucha.
“Over two years since the pandemic began, after more than 20 million estimated deaths from Covid-19 and widespread economic destruction,” she said, “government leaders in Davos face a choice: act as proxies for the billionaire class who plunder their economies, or take bold steps to act in the interests of their great majorities.”
Labor’s win in Saturday’s election heralds real change in health policy. Although Labor had a small-target strategy, with limited big spending commitments, its victory represents a value shift to a party committed to equity and Medicare, and, potentially, a style shift to a hands-on, equity-oriented health minister.
Labor’s health spokesperson, Mark Butler, is expected to be the new health minister, subject to a reshuffle caused by two Labor shadow ministers losing their seats.
Butler is very different from his predecessor. He was Australia’s first minister for mental health and ageing in the Gillard government.
He also held the equity-focused ministries of housing, homelessness, and social inclusion. He has written a book about ageing in Australia, published by Melbourne University Press.
The new minister faces two urgent policy priorities: primary care and covid.
Fixing primary care Outgoing health minister Greg Hunt released an unfunded strategy paper on budget night. It aimed to improve primary care — a person’s first point of contact with the health system, usually their GP or practice nurses. The paper had languished on his desk for months and was the result of years of consultation and consensus-building.
One of the largest and most important Labor commitments during the campaign was almost A$1 billion over four years for primary care reform, about A$250 million in a full year.
The funding commitment is cast broadly, promising to improve patient access to GP-led multidisciplinary team care, including nursing and allied health and after-hours care; greater patient affordability; and better management of complex and chronic conditions.
Presumably, a key way this will be effected will be through voluntary patient enrolment. A patient would enrol with a practice, and the practice would get an annual payment for that enrolment. This was promised for people over 70 in the 2019–20 budget but not delivered.
This new policy is a welcome start for reform in primary care and signals the importance that a Labor government attaches to the sector.
Mark Butler was minister for mental health and ageing in the Gillard government. Image: Lukas Coch/AAP
The Strengthening Medicare Fund was only sketched out in broad terms before the election, and provides insight into the new ministerial style. The details of the policy will be thrashed out in a taskforce which will include key stakeholders.
Most importantly, the taskforce will be chaired by the minister — no hiding behind consultants; he or she will hold the hose.
Reducing covid deaths Another crucial early challenge for the minister will be addressing the continuing covid pandemic.
Covid deaths continue: three times as many people have died this year than in the previous two. The Coalition delegitimised any form of action, including mask wearing and vaccine mandates, as part of its undermining of state public health measures, especially action by Labor states.
The prevalence of third dose vaccinations, necessary for adequate protection from omicron, sits at about two-thirds of the over-16 population, much lower in the under-16s, meaning that many in the population are not protected.
Public hospitals are bursting at the seams, with staff overwhelmed. This needs urgent attention, and the Coalition strategy of ignoring it and saying it was someone else’s problem, must be dumped.
Labor vowed to “step up the national strategy” late in the election campaign.
“The Australian people have voted for change.”
Labor leader Anthony Albanese told his supporters in Sydney on Saturday after leading his party to victory ending nearly a decade of conservative gov’t https://t.co/ufTwpZ1FXApic.twitter.com/YdEqshEWRC
Aged care support Hopefully Labor’s shadow aged care minister, Clare O’Neil, will continue in this role post-election. She proved more than a match for her hapless opponent, Richard Colbeck.
Labor made big commitments in aged care, creating a significant point of difference with the Coalition, despite the Coalition’s investments in the 2021–22 budget.
In addition to the Coalition commitments, Labor promised 24/7 registered nurse coverage in residential aged care facilities, and to support a wage rise for aged care workers. The latter is particularly important because without a wages uplift, the staff shortages in the sector will continue.
A new approach Labor won’t engage in climate denialism or use climate policy as a political wedge.
Recognising and addressing climate change is an important issue for the health sector and, of course, the community more broadly as the teal surge and the Greens’ wins demonstrated.
Labor has committed to establishing a centre for prevention and disease control, which should provide a framework for addressing social and economic determinants of health.
Potentially as important in terms of policy style are Labor’s public service policies. The “consultocracy” which thrived under the Liberals will be shown the door, replaced by public servants doing the job the public service has always been available to do.
Obviously, a new Labor government will not be able to be meet all the community’s pent-up aspirations in a single term.
Nevertheless, it is disappointing Labor did not commit to phasing in universal dental care – the crucial missing piece of Australia’s universal health coverage.
Butler and his colleagues have a huge agenda on their plates. Starting with primary care is a good first focus, as without those foundations in place, the whole system cannot work well.
Aotearoa New Zealand has reported 9570 new community cases of covid-19 and a further 32 deaths today, bringing total publicly recorded deaths with the coronavirus 1017.
In a statement, the Ministry of Health said the total number of deaths was up by 31 from yesterday as they had removed a case which had been previously reported twice.
“This case was initially reported on March 10. The deaths being reported today include people who have died over the previous six weeks, since April 5.”
The seven-day rolling average of reported deaths is 17.
“Of the people whose deaths we are reporting today; two people were from Northland; nine from the Auckland region; two from Bay of Plenty; two from Taranaki; one from Tairawhiti; four from MidCentral; two from Hawke’s Bay; three from the Wellington region; one from Nelson-Marlborough; four from Canterbury and two from Southern.
“One person was in their 20s; four people were in their 40s; two in their 50s; four in their sixties; nine in their 70s; nine in their 80s and three were aged over 90.
“Of these people, 10 were women and 22 were men.”
The seven-day rolling average of community case numbers is 8024 — last Wednesday it was 7533, the ministry said.
It said there are 425 people in hospital, including nine in ICU.
I got my second COVID booster shot this morning, so if I do catch this damned thing, it won’t be for lack of ducking. The CVS worker who dosed me seemed an affable sort and the coffee had just kicked in, so I decided to have a bit of sport at the expense of the medical industry. When he brought the tray with the syringe over, I asked if it was the one with the Bill Gates microchip or the one that glows to let Satan know where I am. He stared at me a long moment, looked left and right, then leaned close and said, “5G, man. 5G.”
With solemn tone and a truly daunting dot-matrix map of the lost, The New York Timesput forth the question that nobody seems prepared to deal with at this juncture: How did this country suffer one million COVID deaths, easily the most of any country in the world, in less than three years?
The answers are spread across a broad palette of shame and disgrace that, brushstroke by disgraceful brushstroke, combined to paint a mural of a nation in pinwheeling decline. COVID did not do this to us. Like water, it made for the lowest places and flooded the gaps until the walls crumbled, the floors cracked, and the “exceptional” country was forced to confront just how drab and subpar it really is… which may serve to explain the silence enveloping this grim and monstrous milestone.
“This is how it happens,” writes Indrajit Samarajiva, who watched as his home country of Sri Lanka collapsed after years of civil war. “Precisely what you’re feeling now. The numbing litany of bad news. The ever rising outrages. People suffering, dying, and protesting all around you, while you think about dinner. If you’re trying to carry on while people around you die, your society is not collapsing. It’s already fallen down.”
It was capitalism, of course, that made sure this thing would rule the day. The idea of obeying science to the point that multi-billion dollar corporations might lose custom and market share for a time was more than intolerable; it was heresy spoken against the faith of the free-marketeers and their trickle-down pabulum. Minimum-wage workers behind plexiglass at the Piggly Wiggly were hailed as heroes in the media, but they weren’t heroes… or at least they didn’t want to be. They needed the money and the insurance (if any was actually available), and so they worked. Thousands were infected, and hundreds died.
The gruesome details of COVID and the meat-packing industry are a perfect metaphor for the collision between greed and disease. According to a report by ProPublica, a cohort of meat-packing concerns combined their efforts and lobbied the Trump administration for exemptions that would allow their plants to remain open while shielding them from legal liability. Soon enough, Trump complied.
“The effect that the meatpacking plant outbreaks had on the early spread of COVID-19 is staggering,” reads the report. “ProPublica and other news outlets tracked cases and deaths involving meatpacking workers. But academic researchers have found that by July 2020, about 6 percent to 8 percent of all coronavirus cases in the U.S. were tied to packing plant outbreaks, and that by October 2020, community spread from the plants had generated 334,000 illnesses and 18,000 COVID-19-related deaths.”
Notwithstanding the towering courage and perseverance of the doctors and nurses who fought COVID on the front lines — wearing garbage bags and masks hosed down with Lysol in the early days because of supply snafus — the bleak truth of this country’s garbled medical industry has been exposed. This reaches beyond the overworked hospitals all the way down to the manner in which we as a nation care for our elders. COVID is exceptionally dangerous for older people, to be sure, but hundreds of thousands of elders died warehoused in “homes” staffed by brutally undertrained workers.
This, again, was capitalism at work, the “for-profit” medical industry championed by capitalists as the best in the world. The dead know better.
Speaking of sham capitalism, no critique of the last three years would be complete without a long look at Donald Trump himself, whose performance as president during the crisis will go down in history as one of the more spectacular failures since Icarus told his dad, “Just a little higher.”
At this moment, we have 22 patients in the United States currently that have coronavirus. Unfortunately, one person passed away overnight. She was a wonderful woman, a medically high-risk patient in her late 50s. Four others are very ill. Thankfully, 15 are either recovered fully or they’re well on their way to recovery, and in all cases they’ve been let go, and they’re home.
Additional cases in the United States are likely, but healthy individuals should be able to fully recover, and I think that will be a statement that we can make with great surety now that we’ve gotten familiar with this problem. They should be able to recover should they contract the virus. So healthy people, if you’re healthy, you will probably go through a process and you’ll be fine.
First of all, the deceased person he referred to was a man, not a woman, setting the tone for the fact-free avalanche of calamity his administration became in the ensuing months. The happy talk, though, is the tell: he made this statement weeks after telling journalist Bob Woodward, “You just breathe the air and that’s how it’s passed. And so that’s a very tricky one. That’s a very delicate one. It’s also more deadly than even your strenuous flus. This is deadly stuff.”
Hundreds of thousands of deaths, along with millions of infections, lay at Trump’s spray-tanned feet, but the dying has continued through the entirety of the Biden administration. In this, we have the perfect storm: A president weighed down by the failures of his predecessor and beset by a Republican opposition that has been more than happy to use a lethal pandemic for political purposes. It also has not helped that Biden and his fellow Democrats have raised snatching defeat from the jaws of victory into a form of performance art.
In the face of all this, frustrated silence reigns. There’s no mystery to it; a great many myths about greatness have been shredded and burned in the passage of COVID, and here we are once again confronted with a new wave of infections. New cases are exploding across the country, especially in areas where the GOP convinced people that vaccinations and masks are some sort of liberal Trojan Horse. There were more than 90,000 new infections yesterday alone, a two-week increase of 60 percent.
Biden ordered flags to be flown at half-mast to honor the million we have lost. It is as bland a recognition as any other we have seen. The longer we refuse to face what this really is — a pandemic that has attacked us at our weakest places that were supposed to be our strongest places — the longer this will continue. It is a reckoning that must be both national and personal, or there will be no recovery at all.
One of the first pickets has been outside Hutt Hospital, with workers chanting and holding signs, and getting lots of beeps of support from passing cars.
Social worker Lorraine Tetley said her team was losing social workers to higher paid jobs in the public sector.
Those left behind felt undervalued, she said.
“They’re essential workers who work on the frontline during the pandemic. Every day we work with risk and we work with vulnerable families and we’re not paid fairly for the work we do,” she said.
Working hard under covid
Dental therapist Char Blake said they had been working really hard, especially after the lockdown and covid restrictions.
“We love caring for patients but is just really hard to pay for things with the price of things going up and we’ve waited 18 months for a pay rise,” Blake said.
Today’s allied health workers strike. Video: RNZ News
Dental assistant for the School Dental Service Faye Brown said she was paid just over the minimum wage.
Her service was six people short, and in danger of losing more.
“It can be quite stressful at times — we have to do more than we are supposed to at times. We don’t want to let our patients down,” she said.
Jane McWhirter tests newborn babies’ hearing and says she is earning the same amount as her 16-year-old daughter who works at Dominoes Pizza.
She says even though she is training on the job, she is doing important, skilled work and she and her colleagues deserves better.
This article is republished under a community partnership agreement with RNZ.
Reports of her covid status follow a statement yesterday by Director-General of Health Dr Ashley Bloomfield that thousands of new cases of covid-19 were being reported every day in New Zealand, but this was likely to be half of the number of actual cases.
With a further 29 deaths with covid-19 and 7441 new cases yesterday, Dr Bloomfield said the impact of the severity of omicron was still visible.
Prime Minister Ardern has been symptomatic since Friday night, according to a statement, and has “moderate” symptoms. She returned a weak positive Friday night and a clear positive this morning on a RAT test.
Ardern will be required to isolate until the morning of Saturday May 21.
Missing the Budget
Ardern, who has been isolating since Gayford tested positive, will now have to miss the Budget announcement on Thursday and the release of the government’s Emissions Reduction Plan on Monday.
“There are so many important things happening for the government this week,” she wrote.
“I’m gutted to miss being there in person, but will be staying in close touch with the team and sharing some reckons from here.
“To anyone else out there isolating or dealing with covid, I hope you take good care of yourselves!”
Former Labour Party president Mike Williams hopes she will be well enough to travel.
“After two years of isolation, internationally she’s a rock star attraction, and it does the country a hell of a lot of good to get her out and about.”
Williams said Ardern, 41, was young and fit, so should be fine.
Deputy Prime Minister Grant Robertson will take the post-cabinet press conference on Monday.
This article is republished under a community partnership agreement with RNZ.
Vanuatu’s outgoing president, Obed Moses Tallis, has urged the government not to abolish the ministry of justice, warning against a “dictatorial system”.
His opening speech to Parliament’s first “ordinary” session of 2022 is his final duty of his mandate which will end in July.
“In my observation during my five-year term as a Head of State, the judiciary in Vanuatu under the leadership of Chief Justice has played an important role in stability, growth and progress of the nation for it uniqueness of it its independency,” he said.
“To cherish the stages of the third pillar of the constitution, I urge the government to carefully consider its decision to abolish the Ministry of Justice.
“It is important that the government maintain the Ministry of Justice. Without the judiciary, there will no effective work from the government and there will be no prosecution.
“The work of the Vanuatu Police force will have no bases and there will be a dictatorial system in place,” he said.
In his speech, Tallis also praised the country’s frontline workers for their hard work during the community outbreak of covid-19.
Frontline workers risked lives
He said frontline workers risked their lives and their families by being exposed to the virus.
He also hailed their efforts in challenging disinformation about the omicron variant.
Tallis said the hard work of the frontline workers had contributed to stabilising the outbreak in the affected provinces.
Meanwhile, Vanuatu’s Ministry of Health reports 37 new cases of covid-19.
Tallis told Parliament Vanuatu had gone through several challenges because of the covid pandemic.
He acknowledged the tourism sector for its contribution to the recovery of Vanuatu’s economy.
“Tourism has contributed a lot to economic growth but the only problem is that it is a fragile industry and cannot sustain us during total border restrictions which restricted the mobility and the movement of the tourists.
Tourism a ‘fragile industry’
“We experienced a high rate of unemployment with the closure of hotels and caused financial difficulties of the family.
“The other reason why I am saying that tourism is a fragile industry is the ongoing climate change impact across the globe which could affect this industry.
“In my humble view, I want to see government to invest more in vibrant industry such as agriculture, fisheries and utilising the natural resources in land and marine,” Tallis said.
He acknowledged government initiatives to redirect its focus in the agriculture sector and the programme of coconut replanting and cattle restocking and the establishment of the connection of the cooperative to the local farmers in order to participate effectively in the country’s economic growth.
The Prime Minister, Bob Loughman, and the Leader of the opposition, Ralph Regenvanu, both thanked Tallis for his role as Head of State during his five-year mandate.
This article is republished under a community partnership agreement with RNZ.
New COVID-19 infections are once again on the rise across the United States, according to the Centers for Disease Control and Prevention (CDC). COVID deaths in the U.S. have now reached the 1 million mark, a figure widely regarded as an undercount.
The steady increase in COVID cases underscores the perilous wrongheadedness of the recent decision by Kathryn Kimball Mizelle, the federal district court judge in Florida who struck down the national transportation mask mandate on April 18.
“The majority opinion is a result searching in vain for a plausible reason,” California Supreme Court Justice Allen Broussard wrote in 1988, dissenting from a poorly reasoned majority decision in People v. Guerrero, that broadened the factors a judge could consider when imposing a sentencing enhancement. Broussard’s statement also aptly describes the recent decision by Mizelle, who likewise reasoned backward by amassing reasons for her pre-ordained result.
Shortly after taking office, Joe Biden asked the CDC to impose a travel mask mandate to check the spread of the COVID virus. The CDC complied and imposed a mandate on February 3, 2021. For 14 months, people traveling by aircraft, train, road vehicles, and other forms of transportation and through transport hubs were required to wear masks. The CDC extended the mandate several times to give public health experts time to determine whether it should be continued.
As of April 17, the day before Mizelle’s decision, new COVID infections were averaging over 37,000 cases daily, up 39 percent from two weeks prior, according to a New York Times database.
Nevertheless, Mizelle’s ruling allows individual airlines and transit agencies to decide for themselves whether to require masks. By the end of the day on April 18, the country’s largest airlines and the Amtrak rail system had shelved their mask mandates. Some pilots announced midflight that people could remove their masks, much to the shock of many immunocompromised people and those traveling with unvaccinated young children.
The lawsuit in which Mizelle ruled was filed in July 2021 against the Biden administration by two individuals and the anti-COVID regulation organization Health Freedom Defense Fund. The two individuals claimed they suffered from anxiety and panic attacks caused by wearing masks.
In voiding the mandate, Mizelle set forth a bizarre interpretation of the authority Congress granted the CDC to promulgate rules to prevent the spread of communicable diseases, writing that “the Mask Mandate exceeds the CDC’s statutory authority.” In her 59-page ruling, Mizelle held that the CDC overreached the bounds of its authority under the Public Health Services Act of 1944 when it imposed the transportation mask mandate.
A Trump appointee and former clerk to Clarence Thomas (whom she called “the greatest living American”), Mizelle was rated not qualified by the American Bar Association before she was confirmed by Republican senators in a November 2020 party-line vote.
Her lack of qualification is clear, judging by her misinterpretation of the Public Health Services Act. The act empowers the CDC “to make and enforce such regulations as in [its] judgment are necessary to prevent the introduction, transmission, or spread of communicable diseases from foreign countries into the States . . . or from one State . . . into any other . . . State.” The statute lists examples of this authority, stating that the CDC “may provide for such inspection, fumigation, disinfection, sanitation, pest extermination, destruction of animals or articles found to be so infected . . . and other measures, as in [its] judgment may be necessary.”
Requiring masks is a “sanitation” measure, the Biden administration argued, because it keeps the air cleaner. But Mizelle consulted dictionaries and word usage in the 1940s to conclude that sanitation requires active cleaning and masks “clean nothing.”
Although Mizelle quoted the CDC’s finding that masks are “one of the most effective strategies available for reducing COVID-19 transmission,” she substituted her own construction of the act for the CDC’s. Mizelle refused to defer to the CDC as required by the Chevron deference doctrine, which requires a court to accept an agency’s interpretation of a statute when the statute is ambiguous and the agency’s interpretation is reasonable.
Instead, Mizelle relied on the “major questions” doctrine, which holds that agencies such as the CDC cannot decide questions of “vast economic or political significance” unless Congress specifically authorizes it. Right-wing judges often use this flawed doctrine to limit the power of the government to protect peoples’ rights.
Mizelle concluded that the mask mandate violated the Administrative Procedures Act (APA) which requires granting the public advance notice and the opportunity to comment before an agency promulgates a rule. She rejected the “good cause” exception to the notice and comment requirement in spite of the COVID emergency. Mizelle dismissed as insufficient the CDC’s claim that the mask mandate is in “the public interest,” which is one of the factors included in the APA’s definition of “good cause.” She wrote that “[t]he only reason” cited by the CDC for the mask mandate is “the public health emergency caused by COVID-19.”
Astoundingly, Mizelle noted, “The Court accepts the CDC’s policy determination that requiring masks will limit COVID-19 transmission and will thus decrease the serious illnesses and death that COVID-19 occasions,” but she then concluded that this doesn’t amount to “good cause.”
Stressing that the mandate “would constrain [the public’s] choices and actions,” Mizelle chose the freedom of travelers like plaintiff Ana Daza who have “anxiety aggravated by wearing a mask” over the COVID public health emergency.
On April 20, the CDC issued a statement asking the DOJ to appeal Mizelle’s ruling. “It is CDC’s continuing assessment that at this time an order requiring masking in the indoor transportation corridor remains necessary for the public health,” the agency wrote. “CDC continues to recommend that people wear masks in all indoor public transportation settings…. When people wear a well-fitting mask or respirator over their nose and mouth in indoor travel or public transportation settings, they protect themselves, and those around them, including those who are immunocompromised or not yet vaccine-eligible, and help keep travel and public transportation safer for everyone.”
Accordingly, on April 20, the DOJ filed a notice of appeal of Mizelle’s ruling. Inexplicably, the DOJ did not request a temporary pause on Mizelle’s sweeping decision pending appeal.
The conservative U.S. Court of Appeals for the 11th Circuit will hear the appeal, which could take several months. Ultimately, the case could end up at the Supreme Court. The outcome could have long-lasting significance: A federal district court ruling does not constitute binding precedent, but a court of appeals ruling and, of course, a Supreme Court ruling would.
“This sets up a clash between public health and a conservative judiciary, and what’s riding on it is the future ability of our nation’s public health agencies to protect the American public,” Lawrence O. Gostin, a public health law expert at Georgetown University, told the New York Times. “The risk is that you will get a conservative 11th Circuit ruling that will so curtail C.D.C.’s powers to fight Covid and future pandemics that it will make all Americans less safe and secure.”
Gostin also said, “If CDC can’t impose an unintrusive requirement to wear a mask to prevent a virus from going state to state, then it literally has no power to do anything.”
On May 3, the day the most recent extension of the mask mandate expired, the CDC issued a new recommendation that all individuals 2 years and older wear masks “in indoor areas of public transportation (such as airplanes, trains, etc.) and transportation hubs (such as airports, stations, etc.).” The CDC recommended that people wear masks “in crowded or poorly ventilated locations, such as airport jetways.”
But because one right-wing federal judge issued a nationwide injunction against the transportation mask mandate, the CDC could only recommend wearing masks to protect the American people against COVID, as opposed to requiring it.
Hopefully the 11th Circuit will reverse Mizelle’s decision. But if the appellate court affirms her ruling and the case is appealed to the Supreme Court, the right-wing majority may well uphold Mizelle’s decision and dangerously constrain the power of the CDC to safeguard our health. Meanwhile, we travel at our own risk.
It was also announced that visitor visas from the Pacific Islands would open online from Monday, May 16.
The Health Ministry said the seven-day rolling average of reported deaths was 15.
Of the 28 deaths reported today, two people were from Northland, five from Auckland, three from Waikato, three from Bay of Plenty, two from Whanganui, three from the Wellington region, four from the Canterbury region and six from Southern.
One was in their 40s, one in their 50s, two in their 60s, eight in their 70s, 11 in their 80s, five in their 90s.
Eighteen were men and 10 were women.
Yesterday, New Zealand recorded more than one million cases of covid-19 since the pandemic began. New Zealand’s population is 5 million.
This article is republished under a community partnership agreement with RNZ.
Covid-19 daily cases by numbers in Aotearoa New Zealand since the 23 August 2021 delta outbreak began. Image: RNZ
One million deaths. An unthinkable milestone when this pandemic started — and even this gruesome number doesn’t capture who and what we have lost. One million lives lost, dreams unfulfilled, families heartbroken and futures cut short. This loss is unimaginable, and we have only just begun to scratch the surface of how our communities will continue to grapple with this mass death and violence, surely for generations to come. According to the Centers for Disease Control and Prevention, COVID-19 has become the third leading cause of death in the United States, after heart disease and cancer.
As a working Latina mother of two, I feel the ongoing pain and frustration of the pandemic in so many ways. I have lost family members and neighbors to COVID — both old and young. My children, isolated and separated from their best friends during a time in their lives that should be filled with joy and connection, struggled with their mental health and lost critical in-person education. My elderly father had a crushing fall, and his physical therapy, and path to wellness, was greatly delayed. My aunt, Lilia, who suffered from Lupus, died alone because none of us could be with her.
Amid all of this pain, President Joe Biden has dropped most pandemic restrictions, stopped most national tracking, and failed to act on even the most basic federal actions to reign this pandemic in. Disabled and chronically ill Americans have been left adrift — in a maskless world many of my colleagues and friends are unable to safely leave their homes.
We need swift, immediate action at a global level. Fighting this pandemic as if we can defeat it alone has failed. It’s time: President Biden must work with Congress immediately to ensure that supplemental COVID funding includes significant global investments to end the pandemic. Our lives are at stake — and we cannot wait another moment.
Heading into our third year of the pandemic, billions worldwide still don’t have access to COVID vaccines and treatments, continuing to suffer even as pharmaceutical companies reach record profits. Globally, less-wealthy nations have been abandoned to vaccine apartheid, as pharmaceutical companies are selling and distributing vaccines, tests and treatments almost exclusively to wealthy nations. Here in the U.S., it’s communities of color, low-income people and the disabled who face the greatest burden of COVID-19, in terms of death rates but also economically and socially. Those working in lower-wage fields like food and agriculture, warehouse operations, transportation and construction saw higher rates of death than in most other occupations. Working in a nursing home has become one of the deadliest jobs in the country.
The consequences of this pandemic are far reaching and devastating, not just for those we have lost but for the ones they’ve left behind. We have the tools and resources necessary to support our communities and fight health inequity right now — but it’s clear that what is missing is the political will to do so.
Our nation hasn’t seen mass death on a scale like this since World War II, when about 418,000 Americans died. TheAtlantic’s Ed Yong puts it into perspective: “The U.S. reported more deaths from Covid-19 last Friday [March 4] than deaths from Hurricane Katrina, more on any two recent weekdays than deaths during the 9/11 terrorist attacks, more last month than deaths from flu in a bad season, and more in two years than deaths from HIV during the four decades of the AIDS epidemic.”
Where is our great reckoning of this mass violence and pain? And more importantly, where is the political will to fight for our futures, for our families, for a road ahead away from this destruction and toward justice, equality, health and resources for all those still suffering and at risk of death?
Since it rejected a $15 billion supplemental for pandemic preparedness that included global vaccine outreach and funding for free vaccines and testing here in the U.S., Congress has not provided us with the funding we need to continue a robust COVID response, even amid new variants and continued pandemic-related economic stress. With cases rising abroad, experts are sounding the alarm that we should expect a rise in cases here in the U.S. as well. Failure to adequately fund these efforts now will have severe and far-reaching consequences, impacting our ability to deal with a future surge.
Moreover, despite widespread messaging that COVID testing is free, many patients have found themselves facing bills for testing — some for over $1,000. According to The New York Times, about 2.4 percent of coronavirus tests billed to insurers in 2020 left the patient responsible for some portion of payment, adding up to hundreds of thousands of Americans who received unexpected bills. Patients were left with these high bills due to gaps in protections that Congress and the Trump administration put in place early in the pandemic — and our communities are still suffering. While ensuring that people trust the vaccine is a high priority, it is also critical that unexpected costs for testing and treatment don’t deter individuals from getting vaccinated.
As we work to ensure the safety of the global community, Democrats must pass supplemental funding without giving in to Republican demands to tie COVID funds to oppressive immigration policies. We cannot allow partisan distractions and anti-immigrant cruelty to distract from this urgent need. The time to act is now, and we cannot leave anyone behind.
A new way of life is here — seemingly forever. But adjusting to the “new normal” is hardly enough, not when an average of 26,000 new cases are recorded every single day, bringing with them the threat of more death, more loss, more futures taken too soon. Mask mandates are being lifted across the country. We have no national funding to support those infected. Uninsured Americans have little to no support.
The time to act has long gone by — our communities, our children and our families deserve better.
The Fiji Women’s Rights Movement warned today that the value of midwives in the Pacific country was being undermined because of a lack of training and proper planning, and little urgency over the creation of positions.
“The contribution of midwives to universal health coverage in terms of sexual, reproductive, maternal and newborn health, and strategies to fill the service gaps worldwide is rarely mentioned,” said the statement.
“The barriers they face in their professional environment are not often highlighted.”
More than 65 percent of World Health Organisation (WHO) member states were reported 2020 to have less than 50 nursing and midwifery personnel per 10,000 population (about 40 countries in the WHO African region and 25 in the WHO Americas region).
In many countries, said the statement, nurses and midwives constituted more than 50 percent of the national health workforce.
Pacific data on midwives was limited, the statement said.
Nurses resigning
Earlier this year, Fiji Nursing Association president Dr Alisi Vudiniabola warned that nurses were resigning because of stress, fatigue and lack of compensation.
“We see that nurses are leaving for greener pastures and inexperienced nurses are being promoted to lead units in divisional hospitals which means an impact on service delivery,” said the statement.
In the same article covered by The Fiji Times, Dr Vudiniabola shared a report from one hospital where the nurse manager had been working alone, looking after 28 patients as most of the nurses were “sick and tired”.
“The same is for midwives,” said the FWRM statement. “Midwife training is undertaken with no proper planning or positions being created, or positions are often held up, further undermining the value of midwives and the urgency of their work.”
According to the WHO, healthcare provided by midwives who were educated and regulated according to global professional standards was defined as a core strategy for decreasing maternal mortality rates and improving reproductive, maternal, and newborn health.
Midwives could provide 87 percent of sexual, reproductive, and maternal health services but before that can happen, such services needed to be legislated and regulated.
“An enabling environment that allows midwives to offer this full scope of services must be provided.”
Fiji’s commitments
Fiji had made its commitment to Sustainable Development Goals 3 and 4 addressing a reduction in maternal mortality rates but this had not been implemented, said the statement.
Based on reports received, midwives with relevant qualifications like such as the Post Graduate Diploma in Midwifery, Masters in Midwifery were still earning less than F$35,000 a year.
This was the case even when the scope of their work covered areas such as ante-natal clinic consultation, public awareness, births and deliveries, post-natal, retrieval of obstetric and gynecology emergencies in the field (usually handled by doctors), pediatrics, maternal child health, and public health (including immunisation to pre-school for the child).
Midwives also undertake administrative documentation, including maintenance of data repositories, which were not used by the Ministry of Economy in formulating national budgets.
As health communities in Fiji and globally marked International Midwives’ Day today, the FWRM urged the government and the health ministry to place more emphasis on the role of midwives in the health sector.
Queen’s Service Medal for NZ midwife
In New Zealand, midwives’ advocacy was marked on International Midwives’ Day when the Governor-General, Dame Cindy Kiro, presented Pukekohe midwife Claire Eyes with the Queen’s Service Medal at a Government House investiture ceremony which also recognised several covid-19 pandemic response and other service leaders.
Eyes had also assisted midwifery in the Pacific through Rotary and had organised leadership training for midwives and nurses in Australia.
Her citation said in part: “[Claire Eyes] helped prevent closure of the Pukekohe Maternity Unit in the 1990s and secured funding to start the Pukekohe Maternity Resource Centre.
“She was president of the New Zealand Nurses Organisation Franklin Branch. She was involved with negotiations for pay parity for nurses and midwives and assisted the Ministry of Health to set up a structure for midwives providing lead maternity care.
She was NZNO representative to the New Zealand Council of Women.”
Wearing glasses or getting a runny nose is enough to qualify for a mask exemption under current New Zealand’s Ministry of Health criteria — and a doctor says its time for tougher rules.
Hearing aids, hayfever or a tendency to get dry eyes are also reasons to request the legally binding card that says you do not need to wear a mask when normally required to under covid-19 rules.
Some doctors say the reasons are far too loose, with people simply needing to tick just one of the symptoms on the ministry’s website list to get an exemption card sent to them.
Northland medicine specialist Dr Gary Payinda said the card was a great idea for people who had legitimate reasons for not wearing a mask.
But the current list of criteria was so wide it was absurd — almost everyone in the country would qualify, he said.
“If we’ve made it so easy that literally anyone can click a box and say I have a ‘condition’ … we really have to ask is it still a public health measure.”
With so many other measures relaxed, masks were one of the last lines of defence against the virus, and so everyone who could wear one, should be, he said.
Compromising public health measures
He told RNZ Morning Report that compromising one of the most effective public health measures was not doing the community a good service.
“We want the right people to be protected by this law and we want masks to still be a meaningful way of reducing the burden of covid in the community.”
“If we make an exemption process so easy to get that it’s meaningless, we’re shooting ourselves in the foot.
“I want masks to be legitimate and used and trusted, and that won’t be the case if anyone can literally tick the box and say, ‘face coverings give me a runny nose’ and that’s enough to get a mask exemption.”
The criteria have come under scrutiny as the government changes the process for getting a mask exemption card.
Until now, cards were issued by the Disabled Persons Assembly but the new ones are issued by the Ministry of Health and have legal standing.
They are intended for people to show to shops or other businesses so they do not have to explain potentially sensitive reasons why they may have an exemption.
The ministry said it had tried to make the process for applying for a card uncomplicated to avoid marginalising vulnerable communities.
Small minority misuses system
The vast majority of New Zealanders had shown they wanted to do the right thing to protect their communities and only a small minority had tried to misuse the system, it said.
A spokesperson indicated the criteria may be changed as the new card comes into effect but was not able to respond with more details before RNZ’s deadline.
Existing cards, issued with the current criteria, can still be used when the new ones come into effect.
The Disabled Persons Assembly welcomed the new card system, telling Midday Report the old system had been causing distress for some in the disabled community.
Prudence Walker said people had not been believed, refused service or had the police called on them.
She hoped the new card would improve things.
Dr Payinda said there were many good reasons — because of both physical and mental health — that people could not wear masks and he supported them doing that but the current list was open to abuse.
Current criteria wideranging
The current criteria for requesting a card according to the Ministry of Health website include having the following conditions if they make wearing a mask difficult: asthma; sensitive skin or a skin condition like eczema; wearing hearing aids; getting migraines, having glasses, dry eyes or contact lenses; hay fever; difficulty breathing; dizziness, headaches, nausea or tiredness; a runny nose from wearing a face covering; a physical or mental illness, condition or disability.
Needing to communicate with someone who is deaf or hard of hearing is also one of the criteria.
Covid-19 modeller Dr Dion O’Neale said attempting to force those who were adamantly opposed to masks to wear one wouldn’t be effective.
“If they want to be difficult about it they’ll manage to tick the box and say I’m wearing it, and wear it badly.”
Most people did want to protect themselves and those around them, so it was important to keep the messaging clear on how masks work and when to wear them, he told Morning Report.
“It’s physics. The mask, if it’s well fitted, it’s going to be filtering out small particles. If those particles are viruses you’re not going to be infected by them, or if you’re breathing in a much smaller number of those particles you’re going to have a much lower exposure dose, so your infection risk is much lower.”
This article is republished under a community partnership agreement with RNZ.
“What if they think my boy is an adult and rough him up?”
We’ve heard various versions of these fears many times in our personal lives, as a Latino man and Black woman, and in our professional roles as professors who teach about race and racism in society. While the fear that causes someone to avoid the police — whether a fear of racism, deportation, homophobia, sexual violence or some combination thereof — may vary between our communities, the underlying question is always the same: If I call the police, will the outcome be worse than the problem I am trying to address?
Many people fear calling the police for legitimate reasons. In immigrant communities, many worry that a call to the police is a quick way for them or someone in their home to wind updeported. Others, often in African American communities, fear that calling the police could result in their own victimization by police. Survivors of domestic violence may fear that police could escalate an already violent situation, if their story is even believed in the first place. Amid national discussions of racism and police-perpetrated violence, many bystanders worry that calling the police could make them an accomplice to race-based law enforcement violence. And sometimes, folks are so worried about the police showing up first to an emergency that they won’t even call 911 when other services — like EMT services after a vehicle accident — are needed.
Researchhascontinued to provide evidence of what communities have been saying for decades, and health organizations have continued to speak out. The American Public Health Association, the largest organization of public health professionals in the United States, released a statement in November 2018 citing law enforcement violence as a critical public health issue that results in more than a thousand deaths a year, with disproportionate losses among people of color.
But fearing the police should not mean that you have no one to call in an emergency.
In response to the growing awareness of the biases in the policing system, non-police response programs have emerged, with examples in Austin, Texas;Eugene, Oregon;San Francisco, California and Edmonton, Canada. While these programs differ in some ways, they all work to divert individuals away from law enforcement, reduce emergency department admission and provide services such as conflict mediation, welfare checks, and non-emergency care and referrals.
Ann Arbor, Michigan, hopes to develop its own program to be added to the list. On April 4, Ann Arbor City Council approved $3.5 million in funds from the American Rescue Plan Act to develop an unarmed, non-police response to emergencies. The city council’s decision was inspiring — a testimony to the desire of our community to have a care-based response at the core of our city services. Among those who presented public comment in support of unarmed response was Kaveh Ashtari, a public health student and medical assistant, who told councilors:
One of the lasting effects of the COVID-19 pandemic is this challenge of trust. I’ve worked with individuals who don’t feel comfortable accessing emergency services during critical times due to fear of escalation, due to fear of violence, due to fear of their own safety. This fear is real. It is for this reason an alternative is needed that can ensure that an individual is able to feel safe, one that is unarmed, one that the community can trust.
Much of the effort for unarmed response in Ann Arbor has been led by the Coalition for Re-envisioning Our Safety (CROS), with whom we organize. CROS is a multiracial group of community members including social workers, public health experts, faith leaders, community builders, and others who have drawn on research, advocacy and community organizing to develop a plan for an unarmed, non-police response.
Among the key components of the plan are that the unarmed response program be supported politically and funded by city government, be separate from law enforcement and the criminal legal system, expand beyond a sole focus on providing mental health care in times of crisis, and include a public phone number separate from 911. Notably, this is not a plan that replaces 911 (or policing) but is instead additive, offering another option for those who fear that a 911 call may result in unnecessary police presence. The CROS plan, like other successful plans, draws on empirical research and prioritizes community-driven leadership.
President Joe Biden’s 2023 budget allocates an additional $30 billion to new police spending, and reports show an increasing number of cities using American Rescue Plan Act (ARPA) funds to increase their police forces. These are dollars that could have been spent supporting child care, reducing student loan debt or even providing additional COVID-19 tests to those without insurance. Instead, these funds will support further surveillance, bias trainings or community policing — all practices thathavealready proven to be unsuccessful at addressing racial inequities in policing. What’s needed is not more funding for policing but more funding for alternatives to police responses. For example, instead of using ARPA funds to expand a city’s police department, cities could opt to use ARPA funds for planning grants to apply for mobile crisis intervention services, mental health support in place of campus police for students, affordable housing to reduce recidivism, or other community-based services.
The data are convincing: Care-based safety programs aren’t just more humane, they create significant cost savings in health care, policing and legal fees, and reduce ambulance and emergency room services — costs that often otherwise fall on taxpayers. But moreover, non-police alternatives could prevent violence, deportation or ensnarement in the legal system. Everyone, no matter their relationship to the police, should have someone available to call in times of crisis.










 More
More
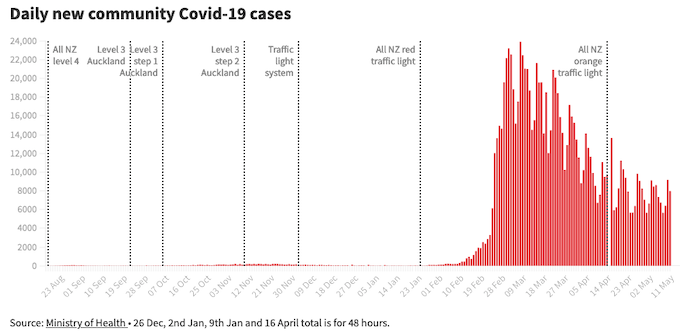
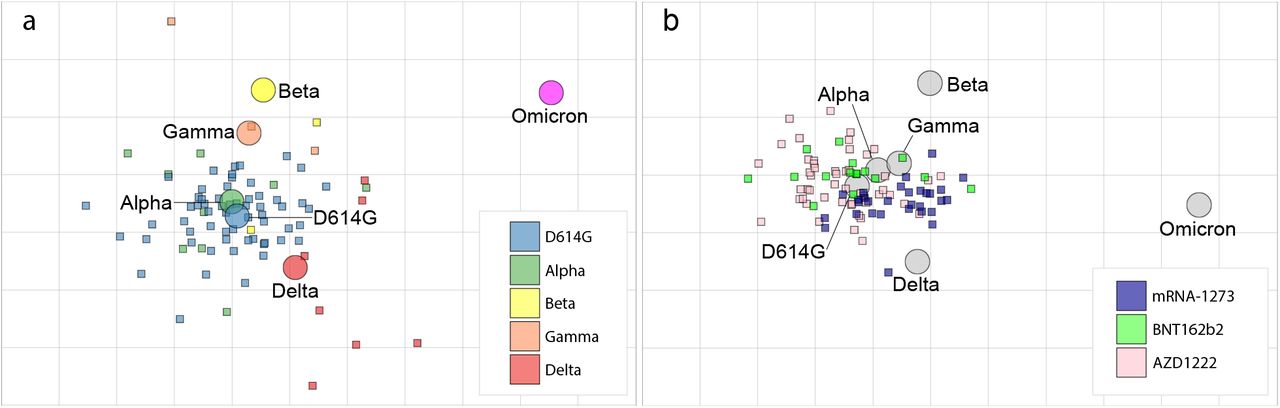{kind=link}
{kind=link}